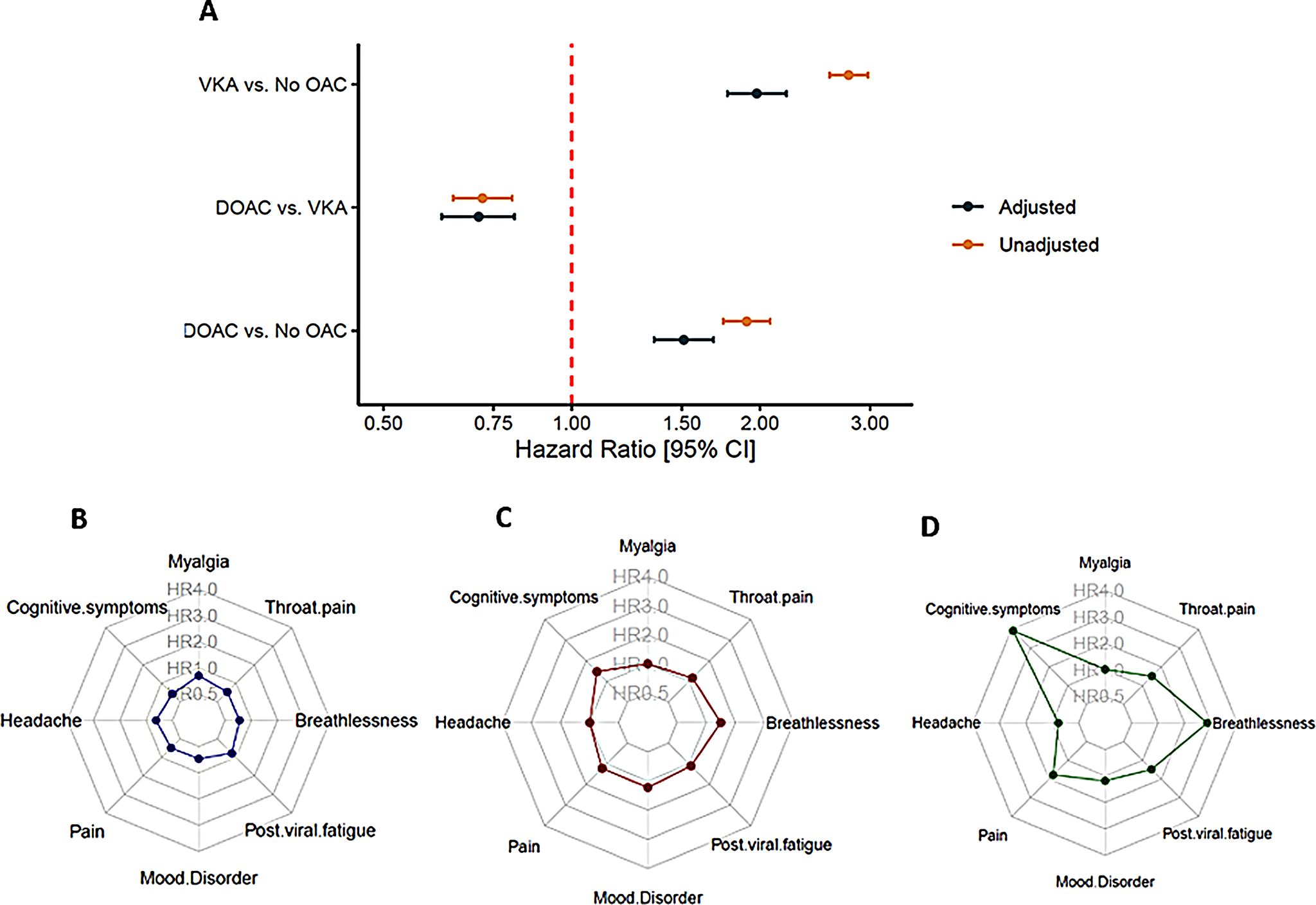
In this study, we investigated the risk of LC/PASC in people already receiving OACs at the time of acute COVID-19 infection. Our main finding is that OAC use does not appear to be associated with any reduction in LC/PASC symptom development and, in general, OAC users were associated with increased risk of LC/PASC.
To our knowledge, this is the first study to investigate the potential for prevalent OAC use at the time of COVID-19 infection to modulate the risk of LC/PASC. Acute COVID-19 infection is recognised a major risk factor for acute thrombotic complications including both arterial and venous thromboembolic disease and sustained prothrombotic changes have been reported long after resolution of acute infection [2, 3]. Thrombotic disease has been implicated in the pathophysiology of LC/PASC in a number of studies, for example Pasini et al. described persistence of altered D-Dimer profiles in people living with LC/PASC and Pretorius et al. described persistent microclot deposits in people living with LC/PASC [4]. These findings have led the putative suggestion of long-term intense anticoagulation as a treatment for LC/PASC however to date this approach has not been tested in clinical trials [5].
Our findings of no benefit for prevalent OAC use on PASC should not be interpreted as evidence for a lack of effect of OAC for PASC. For example, a mechanistic clotting study found extremely high resistance of LC/PASC microclots to fibrinolysis and the same study group have suggested intense anticoagulation incorporating dual antiplatelet therapy alongside OAC may be indicated on that basis. We found insufficient people receiving such regimens within the TriNetX platform to conduct analyses, likely due to the established bleeding risk associated with this therapeutic combination [6].
Another unresolved question, not covered by our study, is the potential role of OAC when a diagnosis of LC/PASC is already made. Following COVID-19, chronic inflammation may persist and contribute to endothelial cell activation, platelet stimulation, and increased inflammatory responses. This process can upregulate procoagulant factors and impair the protective function of the vascular endothelium, leading to abnormal coagulation [7]. Under such conditions, starting OAC -or maintaining this therapy if already prescribed- may lead to lower risk of worse clinical outcomes [8, 9]. However, it should be noted that the overall incidence of vascular thromboembolic events after hospital discharge for COVID-19 remains low (approximately 2%) [10]. What kind of anticoagulation could be employed in this clinical context required further investigation. Hence, our results should be taken to confirm the urgent need for robust data from randomised clinical trials to determine the role for DOACs in the management of LC/PASC associated microclots. Importantly, since COVID-19 is an endothelial problem, it could be hypothesized that if infection quickly overcomes tenuous anticoagulation triggering a cytokine storm and leading to excessive inflammation, the underlying systemic/tissue hypercoagulability conditions of patients requiring previous OAC would quickly synergize with SARS-CoV-2, increasing the likelihood LC/PASC.
There are limitations to consider for this study. First, the data were gathered from healthcare organizations EMRs, potentially leading to underreporting of certain health conditions. Thus, despite we accounted for well-known confounders, residual confounding may still exist due to unmeasured variables. TriNetX does not represent territory wide healthcare systems so follow-up, presentation and recording of some LC/PASC outcomes could have theoretically occurred but not been captured here, potentially leading to underestimation of LC/PASC. Similarly, TriNetX is enriched with secondary care institutions meaning COVID-19 infections may be unrepresentative in terms of severity. We are unable to distinguish dose, and we therefore are unable to assess impact of DOAC dosage on outcomes. There is no agreed definition of the constituent components of a long-covid or LC/PASC diagnosis, and although we aligned our analyses with previously reported algorithms, our results may be confounded by heterogenous reporting of conditions.
In conclusion, we found no evidence prevalent OAC at the time of acute COVID-19 infection is associated with reduced risk of LC/PASC. However, patients on OAC have an enhanced pro-inflammatory and pro-thrombotic state and are more fragile and vulnerable. Therefore, OAC could have played a protective role in this high-risk population, limiting the appearance of more severe LC/PASC. Further work is needed to understand whether there is a role for OAC therapy in the management of LC/PASC.

Comments (0)