
Remember me

We assessed a natural experiment using a cross-sectional design. The study did not fall under the definition of the laws defined in Committee Act § 2 and § 1, and could be initiated without approval from The Committees on Health Research Ethics for the Capital Region of Denmark (Ref number: F-23031959). The study was registered as a clinical trial with ISRCTN (Ref number: 13586262) prior to data collection. Participants were given written information about the study and gave their consent prior to enrollment.
Recruitment and inclusion criteriaA compilation sourced from the Danish National Board of Social Services, detailed the Danish municipalities that had received funds to implement self-governing teams in HHC in 2022–2023 (Buch and Topholm 2023). Based on this we initiated contact by email with municipalities that had undergone the restructure to self-governing teams (i.e. self-governing teams) as well as teams that have not yet undergone the restructure to self-governing teams (i.e. conventional teams).
Eligibility criteria for a conventional team was: (i) working day shifts and (ii) not yet undergone the restructure to self-governing teams. Eligibility criteria for a self-governing team was: (i) divided in groups with a maximum of 12 HHC-workers, (ii) working day shifts and (iii) having worked as self-governing for a minimum of six months. All HHC-workers within the participating teams were invited to participate.
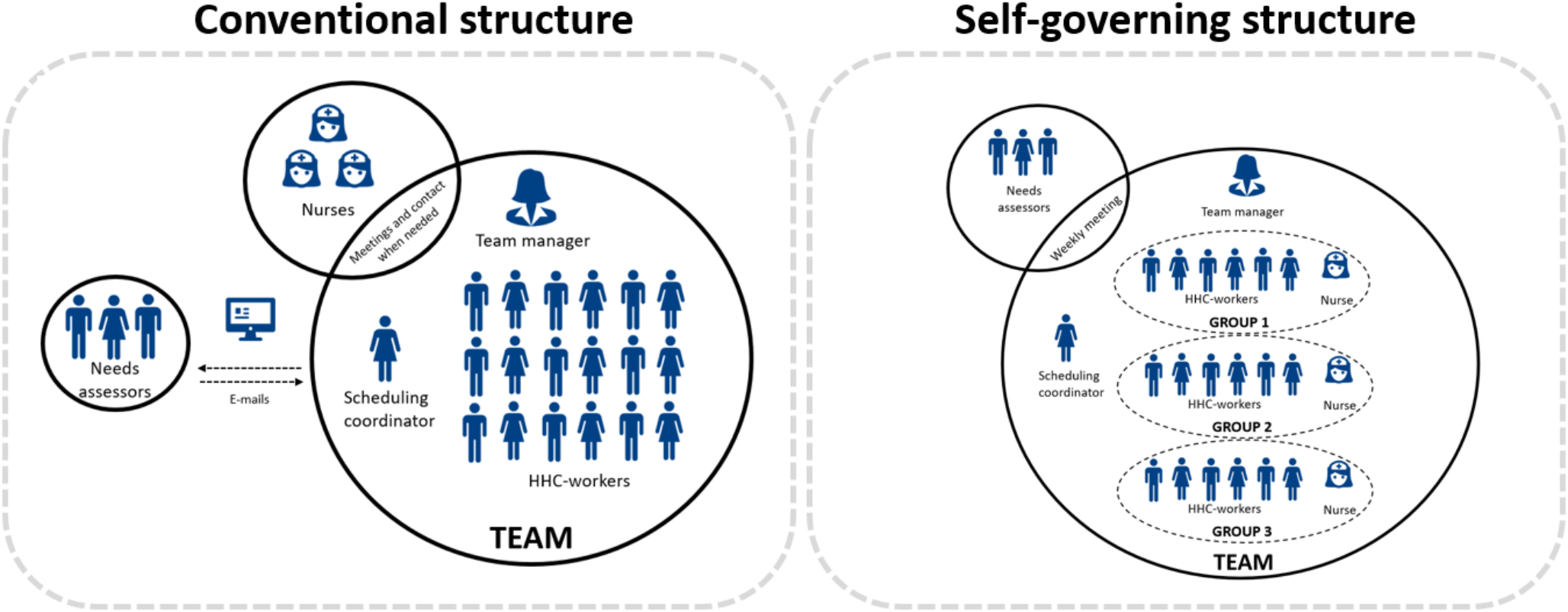
Conventional structured teams and teams structured as self-governingThere is a variation among the funded municipalities in their understanding and implementation of the self-governing elements, including team size and degree of interdisciplinary integration (Buck, M.S., Topholm, E.H., Christensen, J., 2024). However, all self-governing teams included in this study have organized their teams the same way. Figure 1 illustrates the organisational differences between the conventional and self-governing teams included in this study. In conventional teams, there is typically one team manager responsible for 20–30 HHC-workers and one scheduling coordinator. The scheduling coordinator is responsible for managing the allocation of visits and citizen care among the HHC-workers. Moreover, each team is supported by a group of nurses and needs assessors. The nurses are often located geographically close to the HHC-workers, and available for easy contact if needed. The needs assessors are often located in another geographic location. Therefore, the communication between HHC-workers and needs assessors primarily occurs in writing. In the self-governing teams, one team manager is responsible for 2–3 groups which each include one nurse and a maximum of 12 HHC-workers. Each group is responsible for planning their own work schedules on a daily basis. The scheduling coordinator assists all groups in each team with the planning of work schedules. Each team has a weekly inter-disciplinary meeting that includes HHC-workers, the nurses and a needs assessor.
Fig. 1
The structure of conventional teams versus self-governing teams included in this study
Data collectionThe study was performed as a natural experiment with a cross-sectional evaluation (Fig. 2). The data collection was performed between August 2023 and January 2024 and occurred over one working week per team (Monday-Friday). The data collection consisted of quantitative data comprising an electronic questionnaire and technical measurements of physical behaviour. All data were stored and analyzed according to the current guidelines for data protection (GDPR.EU, 2021).
Fig. 2
Timeline of activities in the self-governing and conventional teams, respectively
Start-up meetingThe interactions with both self-governing and conventional teams were initiated with a start-up meeting between the HHC-workers and a member from our research group. During the start-up meeting, the HHC-workers were introduced to the components of the study through a PowerPoint presentation presented by the researcher. Moreover, each HHC-worker was given an envelope containing information about the project, a data processing agreement, an accelerometer and a guide explaining how to attach the accelerometer.
OutcomesThe primary outcome of this study was to compare LBP intensity in self-governing and conventional team structure. Secondary outcomes included (i) LBP duration and work limitations, (ii) neck/shoulder pain intensity, duration and work limitations, (iii) stress, (iv) productivity, (v) influence at work, (vi) meaning at work, (vii) sickness absence, (viii) interpersonal collaboration, and (ix) variation in physical behaviour.
On day one of data collection (Monday), HHC-workers received a unique link to a digital questionnaire via a text message to their mobile phone (Survey Xact, sourced from Ramboll Management Consulting, Aarhus, Denmark). The questionnaire consisted of questions regarding sociodemographic factors (i.e., age, gender, ethnicity, seniority, job title), perceived influence at work, measured on a 0-100 scale (Clausen et al. 2019), meaning at work, measured on a 0-100 scale (Clausen et al. 2019), interpersonal relationships (i.e. collaboration with colleagues, manager and needs assessors), measured on a 0-100 scale (Clausen et al. 2019), well-being, measured on a 0-100 scale (Topp et al. 2015), burn out, measured on a 0–8 scale (“COPSOQ II. The scales of the SHORT COPSOQ II questionnaire”, 2007), need for recovery, measured on a 0–4 scale from “never” to “always“ (Stevens et al. 2019), physical exertion, measured on a 0–10 scale (Borg, 1982), LBP intensity, measured on a 11-point Likert scale (Kuorinka et al. 1987), duration, measured with 0–28 days/month, and work limitations (yes or no), shoulder/neck pain intensity, measured on a 11-point scale (Kuorinka et al. 1987), duration, measured with 0–28 days/month, and work limitations (yes or no), stress, measured on a 5-point Likert scale from “never” to “always” (Clausen et al. 2019; Eskildsen et al. 2015), productivity, measured on a 11-point Likert scale from 0–10 (Kessler et al. 2003), and sickness absence, measured with 0–28 days/month (Burdorf et al. 1996). The HHC-workers in the self-governing teams in addition received questions concerning appraisal of the self-governing structure (i.e. (i) to what extent do you want to continue with being organised as self-governing? and (ii) do you think that other HHC-units could benefit from introducing self-governing teams? ).
The secondary outcome; variation in physical behaviour was measured using a triaxial accelerometer (SENS Motion®, Copenhagen, Denmark) attached to the right thigh midway on the line between the anterior inferior iliac spine and the top of the patella (Skotte et al. 2014) for five consecutive weekdays (Monday-Friday). The HHC-workers logged their work and sleep hours using an app. The accelerometer recorded, sampled and stored triaxial acceleration data at a frequency of 25 Hz with a measurement range of ± 4 g. The data was processed using Motus algorithm (“ActiMotus [Computer software],” 2024), to determine physical behaviour, including time spent sitting, standing still, standing with movement, slow walking (< 100 steps per minutes), fast walking (≥ 100 steps per minutes), stair climbing, running and cycling. These physical activities were then merged into three categories: (i) sitting (sitting and/or lying), (ii) standing (standing still and standing with movements), and (iii) active (slow walking, fast walking, stair climbing, cycling and running). Additionally, we also calculated cycling separately to gain insight into the extent to which HHC-workers utilized cycling for transportation between citizens. Non-movement periods lasting for more than 60 min were considered as non-wear time or sleep. Workdays with <4 h of accelerometer recordings were excluded from the analysis.
Power calculationA power calculation was performed to assess the statistical power of a t-test comparing mean LBP intensity scores (primary outcome) between self-governing teams and conventional teams. Based on a previous study (Korshøj et al. 2018) we aimed for a difference between the two groups of 1.2 in LBP intensity (on a 0–10 NRS). The standard deviation (SD) was estimated to be 2.3, derived from data obtained in a previous trial involving HHC-workers (Stevens et al. 2022). With a power of 0.80, and a significance level of 0.05 and an intra-cluster correlation coefficient of 0.05, a minimum of 58 participants within each group was required to achieve the desired statistical power.
Statistical analysesDescriptive statistics were conducted and summarized in group means, standard deviations and percentages across the teams. T-tests were used to compare outcomes between the two groups and the significance level was set to p ≤ 0.05. We generated violin plots to illustrate the distribution of average worktime in sedentary, standing and active physical behaviours per HHC-workers within self-governing and conventional teams, respectively. Moreover, we generated a violin plot illustrating the distribution of cycling during active worktime. All analysis were conducted in R version 4.1.3 (a language and environment for statistical computing).
Comments (0)