
Remember me
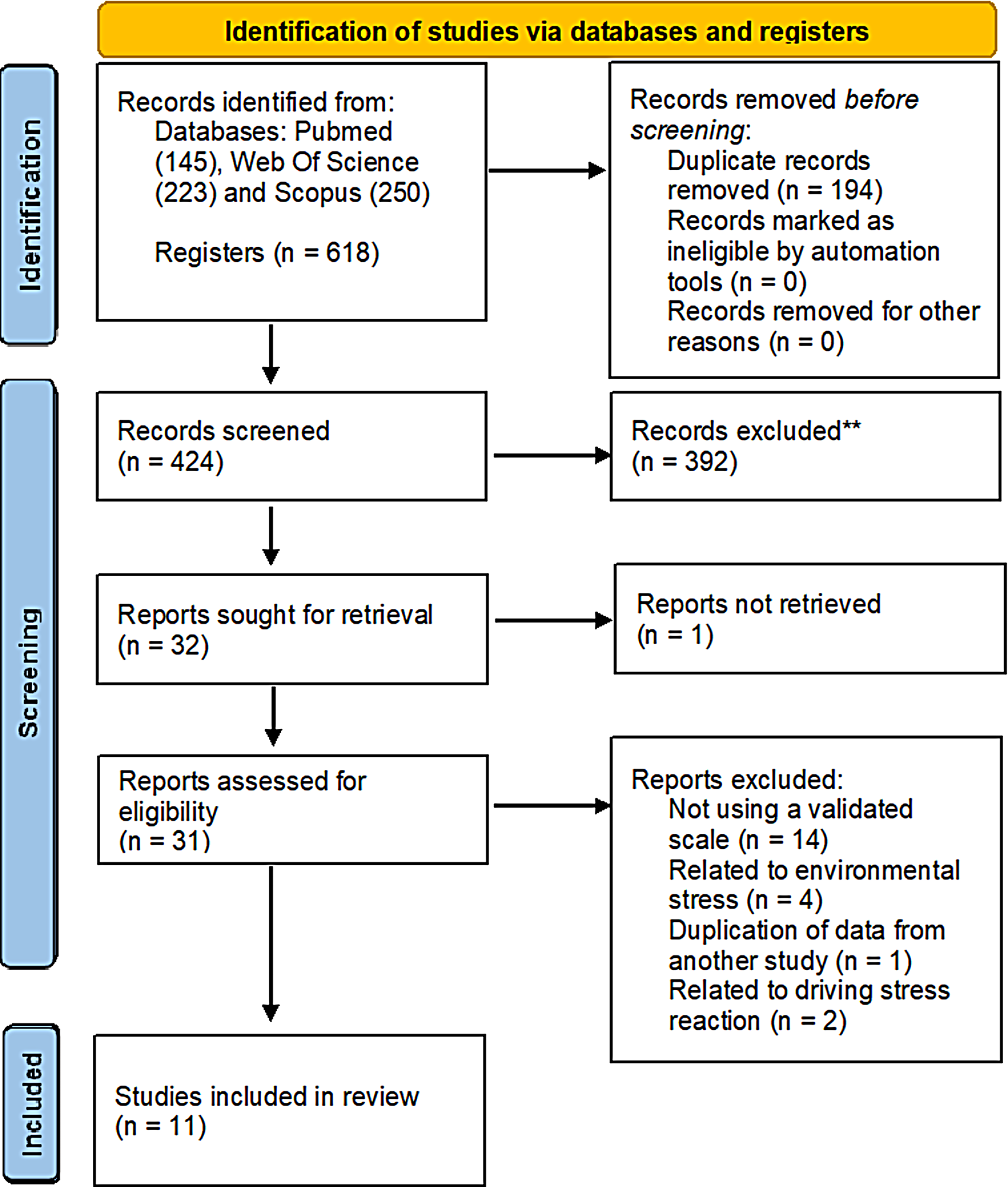

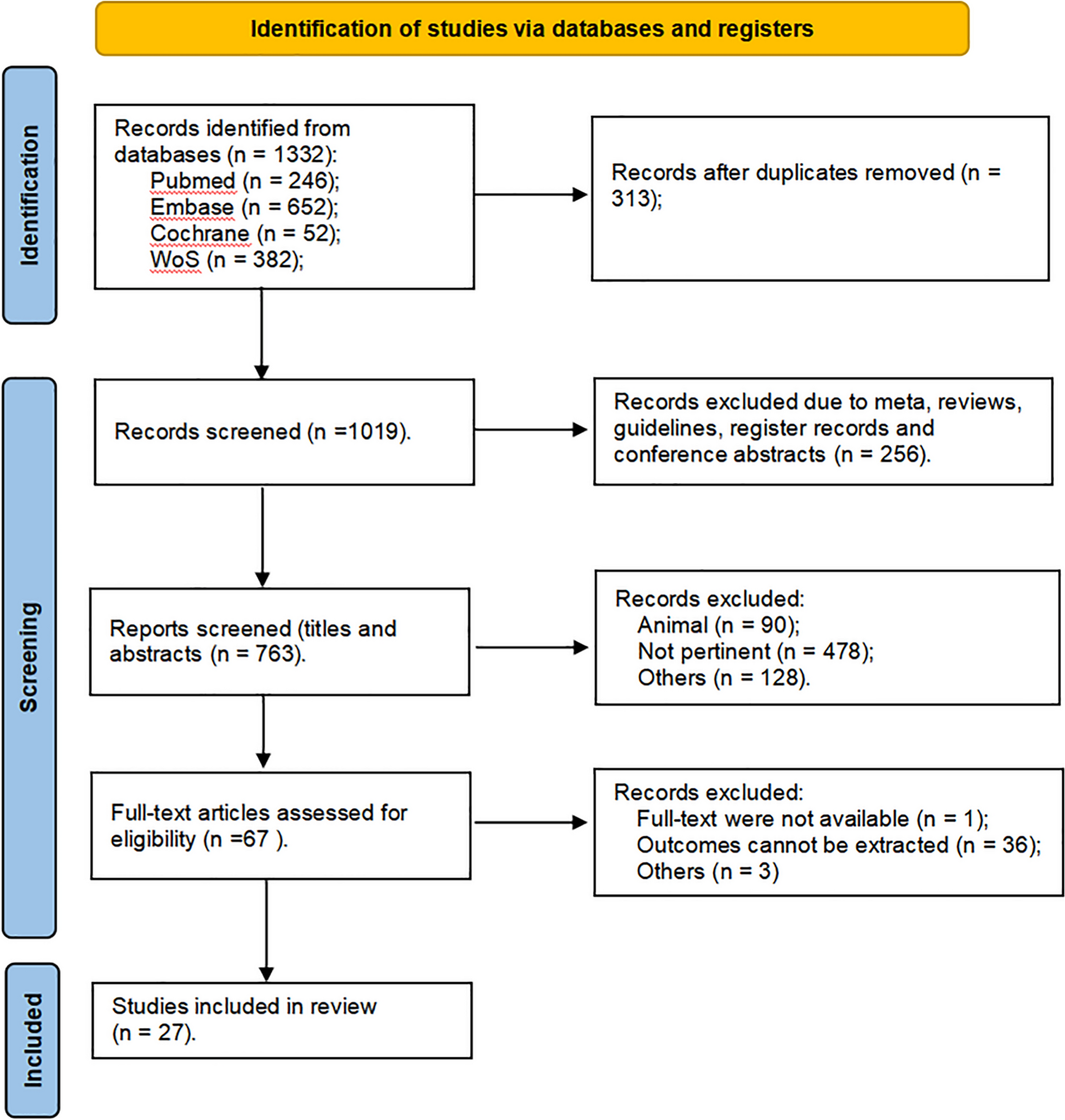
The database search yielded 21,654 potentially eligible papers, excluding 3777 duplicates. After de-duplication, 17,877 articles remained for title and abstract screenings. In total, 183 papers were screened at the full-text stage, amongst which 27 studies met the inclusion criteria (Fig. 1).
Fig. 1
PRISMA flow diagram of the selection of studies
Study characteristicsAll studies were observational, including 18 cross-sectional studies and 7 retrospective cohort studies and two studies used cross-shift cohort design. Cross-shift cohort studies investigated changes in outcomes between shifts. Studies were retrieved from: the USA (n = 8) (Britton et al. 2013a, 2013b; Butler et al. 2017; Stanley et al. 2018; Jung et al. 2021, 2023; Hasan et al. 2023a, 2023b) Australia (n = 9)(McFarlane 1989; Spurrell and McFarlane 1993; Vincent et al. 2016; Doley et al. 2016; Glass et al. 2017, 2019; Berecki-Gisolf et al. 2024; Wah et al. 2024; Jaiswal et al. 2024), Canada (n = 4)(McGillis et al. 2017; Semmens et al. 2016; Moody et al. 2019; Jeklin et al. 2020), Israel (n = 2)(Amster et al. 2013; Leykin et al. 2013), Spain (n = 2) (García-Heras et al. 2022, 2024) and one each from Portugal,(Becker et al. 2023) and Greece (Psarros et al. 2018).
ParticipantsThe included studies ranged in number of participants from 20 (Stanley et al. 2018) to 102,073 (Glass et al. 2017) and, in total, involved over 300,000 individuals who had fought bushfires. Studies also evaluated the health of paramedics (Jung et al. 2021, 2023) and police officers (Amster et al. 2013). Three studies compared the health of bushfire fighters with community-based controls/general population (Hasan et al. 2023a; Glass et al. 2017) (Glass et al. 2019). Two studies compared the health of female firefighters with that of female nurses from a US cohort of Nurses’ Health Study II (Jung et al. 2021, 2023). Ten of the 24 studies included volunteer bushfire fighters (Butler et al. 2017; Jung et al. 2021, 2023; McFarlane 1989; Spurrell and McFarlane 1993; Vincent et al. 2016; Doley et al. 2016; Glass et al. 2019; Becker et al. 2023; Jaiswal et al. 2024) Five studies did not report the sex distribution(McFarlane 1989; Spurrell and McFarlane 1993; Britton et al. 2013a, 2013b; Butler et al. 2017) but, in those that did, the proportion of men ranged between 50(Stanley et al. 2018; Moody et al. 2019) and 100% (Glass et al. 2017; McGillis et al. 2017; Amster et al. 2013)(Leykin et al. 2013; Psarros et al. 2018). Three studies exclusively studied female bushfire fighters to explore impacts on reproductive health (Jung et al. 2021, 2023; Glass et al. 2019). Two studies explored workers’ compensation data (Berecki-Gisolf et al. 2024; Wah et al. 2024). The age of participants was not reported in five studies (Britton et al. 2013a, 2013b; Butler et al. 2017; Jung et al. 2021; Spurrell and McFarlane 1993) but, in the others, ranged from 24.6 (4.8) (Jeklin et al. 2020) to 42.2 (10.6) years (Doley et al. 2016).
Exposure assessment measuresExposure assessment varied by type and study. Some studies estimated exposure based on average hours spent firefighting (McFarlane 1989; Spurrell and McFarlane 1993), while others assessed the impact of multi-day firefighting deployments for specific incidents or shifts (Amster et al. 2013; Leykin et al. 2013). Some studies specifically measured exposure to wildfire smoke and/or chemical flame retardants (Leykin et al. 2013) whilst others drew on historical reports from agencies like the US Department of the Interior (Britton et al. 2013a; 2013b). In specific studies, the duration of exposure ranged from 15.6 h per specific incident to multi-day exposures, with some studies examining risk from long-term exposure over 10–20 years of service (Glass et al. 2017). None of the included studies reported about use of personal protective equipment during firefighting.
Quality of included studiesThe agreed quality assessment scores (Table 1) were an average of 7.2 with scores ranging from 4 to 11. Eleven were assessed as of moderate-quality (total score: 8–11) (McFarlane 1989; Britton et al. 2013a, 2013b; 2017, 2019; Jeklin et al. 2020; Becker et al. 2023; Hasan et al. 2023a, 2023b; Berecki-Gisolf et al. 2024; Wah et al. 2024) and the remaining 16 as low-quality (total score ≤ 7). (Spurrell and McFarlane 1993; Amster et al. 2013; Leykin et al. 2013; Vincent et al. 2016; Doley et al. 2016; Semmens et al. 2016; Butler et al. 2017; McGillis et al. 2017; Stanley et al. 2018; Moody et al. 2019; Jung et al. 2021, 2023; García-Heras et al. 2022, 2024; Psarros et al. 2018; Jaiswal et al. 2024).
Table 1 Quality assessment of included studies of non-respiratory health risks and mortality amongst bushfire fightersThirteen of the low-quality studies were cross-sectional, including a wide range of methods for exposure assessment, outcome measurement, and methods to consider confounding (Amster et al. 2013; Leykin et al. 2013; Semmens et al. 2016; Butler et al. 2017; McGillis et al. 2017; Stanley et al. 2018; Moody et al. 2019; Jung et al. 2021, 2023; García-Heras et al. 2022, 2024; Psarros et al. 2018; Jaiswal et al. 2024).
Seventeen studies relied predominantly on self-reported exposure (McFarlane 1989; Spurrell and McFarlane 1993; Britton et al. 2013a, 2013b; Amster et al. 2013; Leykin et al. 2013; Doley et al. 2016; Semmens et al. 2016; Butler et al.
Comments (0)