
Remember me

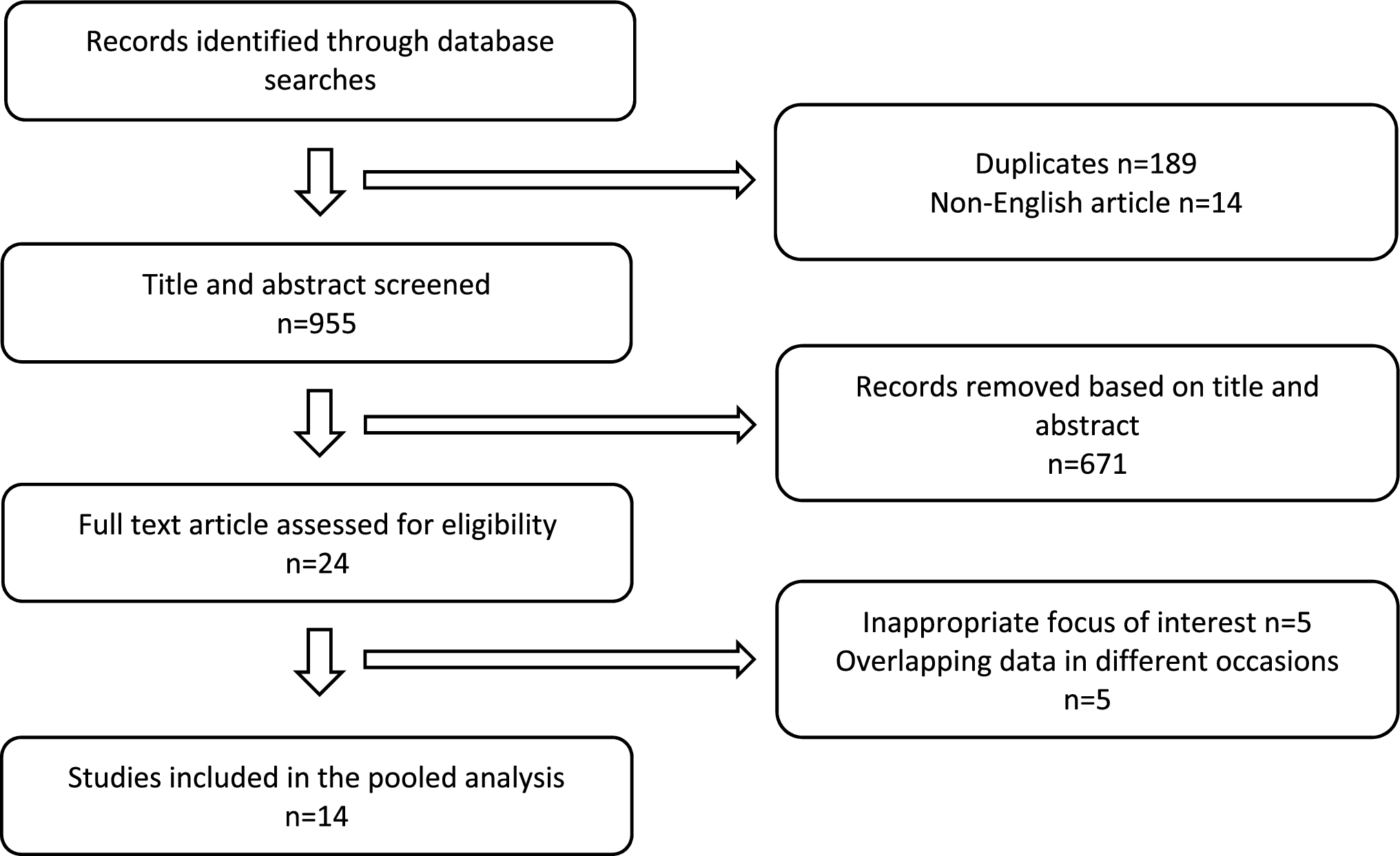
A total of 1158 articles were identified from PubMed, Embase, and Cochrane Library for title screening. There were 14 non-English and 189 duplicated articles, which were excluded. After screening the titles and abstracts, 260 were reviews, commentaries, or conference abstracts, and 671 were found irrelevant. A total of 24 articles were eligible for full-text review. Among these, the oncological outcome of patients with successful nodal conversion and axillary surgery de-escalation was not clearly described in five studies. Another five articles were excluded for overlapping data published on different occasions [14,15,16,17,18]. As a result, 11 retrospective studies [20,21,22,23,24,25,26,27,28,29,30] and 3 prospective studies [19, 31, 32] matched the inclusion criteria and were included in this meta-analysis (Fig. 1). Detailed information on the reviewed articles is displayed in Table 1.
Fig. 1
PRISMA flowchart for the study
Table 1 Characteristics of included studiesStudy characteristics and quality assessmentThe included cohorts consisted of 14 studies published between 2018 and 2023. All studies achieved an overall score of 7 or above on the Newcastle–Ottawa Scale [13] (Table 1). Eleven studies focused on the oncological outcomes of SLNB alone [19,20,21,22,23,24,25,26,27,28,29], while the remaining three articles assessed newer surgical modalities of MARI [30] and TAD [31, 32]. They comprised a total of 4268 patients with node-positive breast cancers before NST.
Clinical and radiological assessmentMajority of the recruited patients had clinical T1-3 (95.0%) and N1 (78.9%) breast cancers (Table 1). Eleven studies reported on the biological subtypes of primary breast tumors [20, 21, 23, 25,26,27,28,29,30,31,32]. Among these, 39.6% were hormone receptor (HR)-positive and human epidermal growth factor receptor 2 (HER2)-negative tumors; 20.9% were HR-positive and HER2-positive; 16.2% were HER2-positive only and 23.0% were triple negative. Five studies only recruited patients who were converted to clinical or pathological node-negative breast cancers after NST [19, 22, 23, 25, 27]. Patients with inflammatory breast cancers [23, 25, 27,28,29, 32], other prior malignancies [19, 23, 25, 28, 30], prior ipsilateral axillary surgery [26, 27, 29], or distant metastases at diagnosis [19, 21, 23,24,25,26,27,28,29, 31, 32] were largely excluded.
Axillary ultrasonography (AUS) was the most commonly used imaging modality for nodal assessment [19, 21,22,23, 25,26,27,28,29,30,31,32] (Table 2). In most studies, positive needle biopsy of suspicious axillary lymph nodes was mandatory to confirm nodal metastases [20, 21, 24, 27,28,29,30,31,32]. Abnormal AUS [19, 22, 25, 26], magnetic resonance imaging (MRI) [22, 25], or positron emission tomography (PET) scan [23] were used otherwise to define clinical node-positive status. After completion of NST, nodal response was reassessed with physical examination only [20, 27] or with the addition of AUS [
Comments (0)