
Remember me

Modern-day drug development requires investments in methods [1, 2] that best capture and represent a drug’s effects on patients. For example, questionnaires for patients to report fatigue symptoms and daily physical limitations for heart failure [3]; report symptoms for cough, pain, dyspnea, fatigue, and appetite for non-small cell lung cancer (NSCLC) [4]; or reports of frequency, severity, and duration of COPD exacerbations [5].
For many diseases, there are currently no universally accepted methods to assess disease manifestation [1] and therefore drug efficacy. While there may be accepted approaches to measure clinical outcomes that indicate benefits for diseases that have a good understanding of the underlying biology, there is still a need to incorporate patient perspectives [6,7,8] on symptoms that matter most to their lives as well as their desired treatment outcomes. Further, for drugs that have novel mechanisms of action, there is a growing expectation to understand how patients perceive improvement/patient tradeoffs to provide a rationale for the endpoint development strategy. As a result, there is a growing emphasis on incorporating patients’ own perspectives in drug development [9] in order to evaluate a drug’s efficacy based on its improvement in patients’ daily life and functioning.
Recognizing the importance of incorporating the patient voice into drug development, the FDA initiated its Patient-Focused Drug Development (PFDD) [10] effort, as part of the Prescription Drug User Fee Act V (PDUFA V) [11], to capture patients’ voices and experiences in drug development. Compared to a biomarker, which is a defined characteristic that can be measured as an indicator of biological processes, a Clinical Outcome Assessment or COA, is a measure that describes or reflects how a patient feels, functions, or survives, capturing the full spectrum of a disease’s impact on a patient’s life [12]. The assessment can be made in various ways. If made through a report by a clinician, it is a Clinician Reported Outcome or ClinRO. If reported by a patient, whether by self-report or by interview, then it is a Patient Reported Outcome or PRO. If made by a non-clinician observer, it is Observer Reported Outcome or ObsRO. If it is a measurement based on standardized task(s) actively undertaken by a patient according to a set of instructions, it is a Performance-Based Assessment or a PerfO. PerfOs that leverage a Digital Health Technology (DHT) as a data-capturing tool are referred to by the FDA as DHT-Passive Monitoring COAs. The unifying factor between all the different types of COAs is that, after undergoing rigorous testing and validation, they are an accepted measure of how patients feel, function and/or survive and can be used in regulatory-decision making.
FDA’s Drug Development Tools (DDTs) Qualification Program was formalized via the passage of the 21st Century Cures Act (Cures Act) Sect. 3011 [13] in 2016. This program was established to allow the FDA to review and qualify DDTs such as biomarkers, COAs, and animal models [14]. We focused our analysis on COAs because of the growing importance of incorporating patients’ voices into drug development. Qualified DDTs are made publicly available to improve understanding of emerging regulatory science and to enhance drug development. Further, DDTs can be used in the review of regulatory applications such as Investigational New Drug (IND) Application, New Drug Application (NDA), or Biologics License Applications (BLA) to aid in assessment of a product’s benefit versus risk to patient.
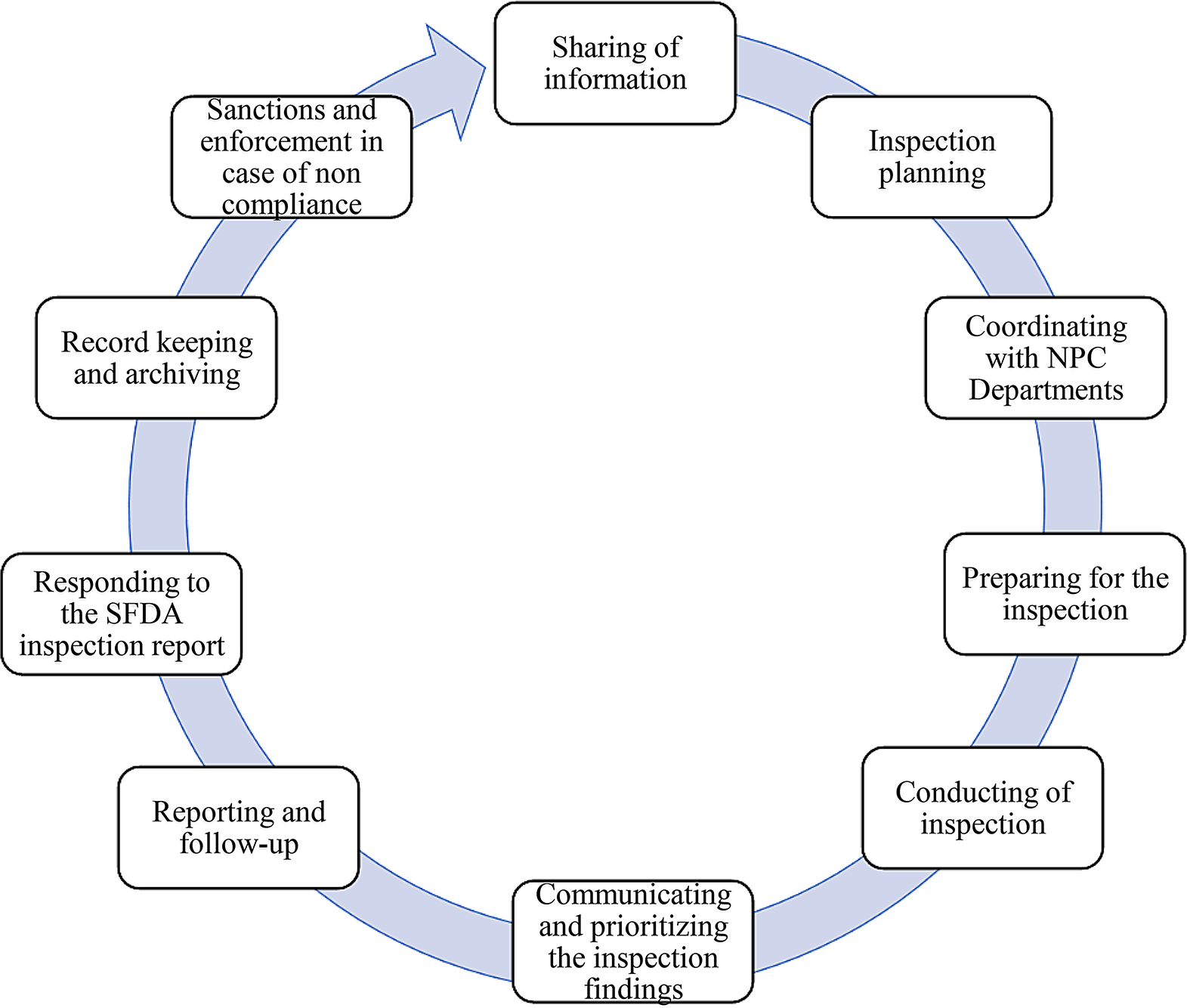
As part of its efforts in codifying the DDT program, FDA issued a guidance document entitled “Qualification Process for Drug Development Tools” (the DDT guidance) in 2020 [15]. The DDT guidance outlines the step-by-step process, materials, and timelines for review (Fig. 1). In brief, the process involves; (1) Letter of Intent (LOI), (2) Qualification Plan (QP), and (3) Full Qualification Package (FQP). Prior to the review of each submission type, FDA will assess the completeness of the submission and readiness for review, which we are defining here as the Completeness Assessment (CA) step. Figure 1 shows the review timelines for LOI, QP, and FQP which are 3 months, 6 months, and 10 months, respectively. CA review timelines for each step are not specified in the DDT guidance. In the current process, there are no limits to the number of submissions per requestor, no submission fees, and no fixed deadlines by which a requestor needs to submit documents for subsequent steps after receiving the FDA determination letter.
According to FDA, COA qualification is a regulatory conclusion that the COA is a well-defined and reliable assessment of a specified concept of interest for use in adequate and well-controlled (A&WC) studies in a specified context of use (COU) [14]. COA qualification represents a conclusion that within the stated COU, results of assessment can be relied upon to measure a specific concept and have a “specific interpretation and application in drug development and regulatory decision-making.” Once a COA is qualified, it will be publicly shared via the FDA website and can subsequently be used not just by the requestor but by all sponsors and developers to support drug and biologic development [13, 14]. However, we note that, in determination letters from FDA, COAs are qualified as a measure for exploratory use.
Fig. 1
Process Map for DDT submission and qualification This process map is based on the FDA DDT Guidance [15] and provides the COA developer/requestor the steps they need to follow if they want to submit a DDT for review. Acronyms Used: LOI = Letter on Intent; CA = completeness assessment; QP = Qualification Plan; FQP = Full Qualification Package
Since the DDT program is now well-established, we decided to analyze its impact on drug development. Specifically, we chose to examine the performance and impact of the COA Qualification Program on innovative drug development, including the timeline and utilization of qualified COAs in drug clinical trials.
Comments (0)