
Remember me




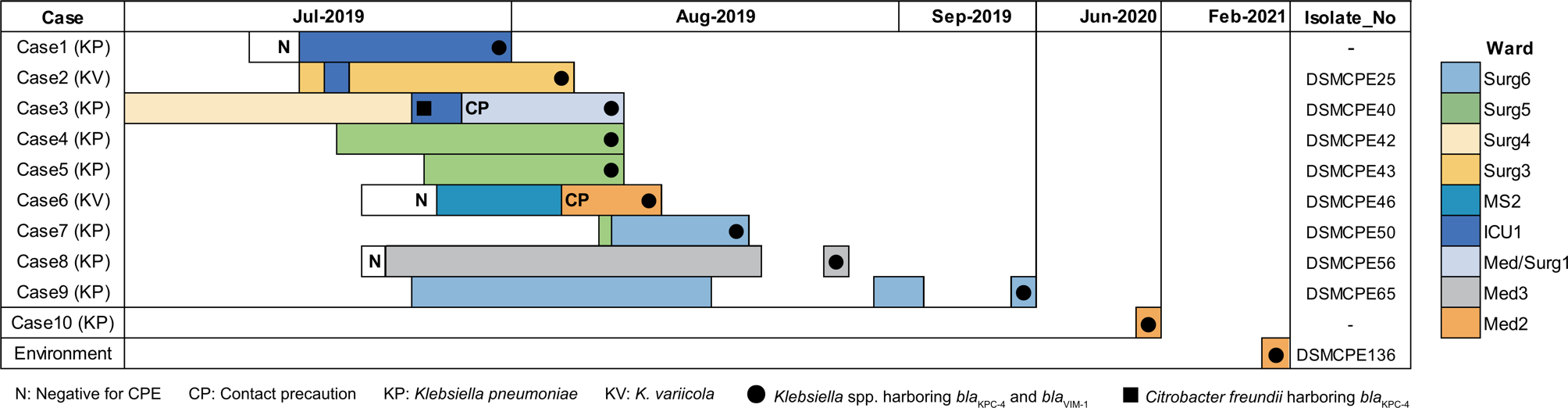




Monitoring and controlling bioaerosols is a key strategy for infection prevention in hospital settings. Figure 1 illustrates the distribution of fungal species isolated from the air. This study revealed that 45% (21/47) of air samples collected from the ICUs across various hospitals tested positive for fungal species, with an average concentration of 23 ± 16 CFU/m3. Comparatively, a Spanish hospital study reported an average fungal concentration of 14 CFU/m³ [24]. The predominant fungal species identified in the samples were Aspergillus spp. (38%) and dematiaceous fungi (36%), including Cladosporium, Alternaria, and Curvularia. Other detected fungal species included Candida albicans, Penicillium spp., Gymnascella dankaliensis, and Hamigera insecticola. As shown in Fig. 1, both Aspergillus spp. (38%) and dematiaceous fungi or one of these fungal species were present in air of all hospitals, except hospital NO. 5 where no fungi were detected during air sampling. Previous researches have similarly reported Cladosporium and Aspergillus as dominant species in hospital air. A study by Ghazanfari et al. (2022) found Aspergillus (39.5%) and Cladosporium (16.6%) to be the most commonly isolated fungi in air samples collected from various wards in 23 hospitals across 18 provinces in Iran [16]. Additionally, Sham et al. (2021) noted that Aspergillus, Cladosporium, and Penicillium spp. were among the most frequently isolated fungal species in hospitals worldwide [25]. The frequent detection of Aspergillus, dematiaceous fungi, and Penicillium in the hospital air can be attributed to their robust growth on various substrates under diverse weather conditions, coupled with their high spore production and dispersal capabilities [26, 27].
Fig. 1
Frequency of fungal species detected in air samples
Figure 2 depicts the frequency of fungal species isolated from exhaust vent surfaces. Fungi were present in all collected samples (100%) from the vents. The most prevalent species were Aspergillus spp. (55%), dematiaceous fungi (21%), and Rhizopus spp. (6%). Additional fungal species identified included members of the Chaetomium, Pyronema, and Penicillium genera. Notably, A. niger was the most frequent species (26%), found in samples from multiple hospitals. A study by Azimi et al. (2013) on hospital air-conditioning systems in Iran identified Aspergillus, Penicillium, and dematiaceous fungi as the dominant species [28]. Similarly, Kelkar et al. (2005) found Aspergillus, Penicillium, Fusarium, and Rhizopus to be prevalent in Indian hospital air- conditioning systems [29]. Our findings indicate that exhaust vents provide conducive environments for mold growth and sporulation, making them significant sources of fungal contamination in hospital settings.
Figures 1 and 2 illustrate the presence of Aspergillus spp. and Mucorales in hospital environments, underscoring their potential role in the development of IFDs. Of the over 180 Aspergillus species, approximately 20 are recognized as opportunistic pathogens in humans. A. fumigatus, A. flavus, A. niger, and A. terreus are responsible for the majority of invasive aspergillosis (IA) cases, with A. fumigatus being the primary agent, capable of causing disease at concentrations as low as 1 CFU/m³ of air [26, 30]. Although A. fumigatus was not detected in the hospital environments studied, A. flavus and A. niger were frequently isolated from both air and surface samples, with concentrations ranging from 6 to 15 CFU/m³ (Figs. 1 and 2). In a study by Ghazanfari et al. (2022) conducted in 23 hospitals across 18 provinces of Iran, A. flavus complex (38/96, 39.6%) and A. niger complex (31/96, 32.3%) were the most dominant species isolated from air and equipment [16]. The high prevalence of A. flavus and A. niger in our study, as well as in other clinical and environmental samples from Iran, is likely due to their high adaptability to hot and dry climates [16]. Notably, A. flavus has been reported as the most common etiological agent of invasive aspergillosis in Iran [14].
Rhizopus, a mold genus from the Mucorales order, is most commonly associated with mucormycosis, with R. arrhizus accounting for nearly 60% of human cases [31]. As depicted in Fig. 2, R. arrhizus was isolated in exhaust vent samples, posing a potential risk to immunocompromised patients in ICUs.
Fig. 2
Frequency of fungal species detected in exhaust vent samples
Environmental investigation and potential impact on fungal concentrationEnvironmental monitoring for the presence of fungi, alongside the assessment of environmental parameters, can reveal potential shortcomings in infection prevention and highlight areas for improvement. Fungi, a prevalent microbial contaminant in indoor settings, have a strong capacity to proliferate on various construction materials, releasing spores that may lead to fungal infections in vulnerable patients [32]. Key factors such as temperature, relative humidity, building materials, air exchange rates, ventilation systems, and construction practices can influence fungal concentrations in hospital environments. Table 1 outlines important environmental parameters assessed using the CDC checklist. In this study, the age of hospital structures was a recurring issue, prompting renovations in some cases. Older buildings and the materials used in construction can contribute to fungal colonization [33]. Research shows that aged and deteriorating buildings exhibit higher levels of fungal contamination compared to newer constructions [34]. The most significant fungal contamination was observed in Hospital No. 4, where concentrations reached 50 CFU/m³. It is likely that construction activities, such as dust generation, contributed to these elevated fungal levels in ICU air [33]. Park et al. (2019) observed that during construction phases, including demolition and excavation, airborne fungal spore counts increased, correlating with a significant rise in invasive Aspergillus infections [4]. In hospitals 1, 2, and 7, fungal concentrations were measured at 31, 38, and 29 CFU/m³, respectively. Factors such as open ICU windows and the hospitals’ proximity to major roads may have contributed to the elevated fungal presence in these facilities. The Centers for Disease Control and Prevention (CDC) recommends implementing control measures such as sealing windows and using special ventilation systems to manage infection risk [35]. The study also revealed a lack of cleaning in the hospitals’ exhaust vents, as evidenced by the substantial fungal contamination within these systems. Given their propensity to accumulate dust and moisture, these systems are potential hotspots for microbial contamination, necessitating regular cleaning and maintenance to mitigate the spread of pathogenic microbes.
Table 1 Important environmental parameters checked by the CDC checklistBoth temperature and relative humidity are critical factors affecting bioaerosol concentrations, including fungi, in the air and on surfaces [30, 36]. Throughout the study, ICU ambient temperatures ranged from 19 to 27 °C, averaging 21.7 °C, while relative humidity spanned 11 to 39%, with an average of 21.9%. Statistical analysis indicated that relative humidity significantly impacts fungal concentrations, while temperature did not show a notable correlation with fungal counts. Mirhoseini et al. (2015) also reported a significant positive association between relative humidity and bioaerosol numbers in hospital settings, but found no substantial link between temperature and fungal quantities [37]. Notably, despite Isfahan’s semi-arid climate and low humidity levels, which are generally unfavorable for fungal growth, Aspergillus species, being xerophilic, can thrive and produce spores even in environments with low atmospheric relative humidity and on substrates with minimal moisture content [38].
Antifungal drug resistance in isolated fungiThe increasing resistance of pathogenic fungi to antifungal drugs presents a growing challenge to healthcare systems. The widespread use of antifungal medications has altered the epidemiological profile of fungal infections, with a rise in drug-resistant fungal species in clinical settings, often leading to treatment failures. As hospital environments contaminated with fungal spores are a source of nosocomial fungal infections, analyzing the antifungal susceptibility profiles of isolated species can enhance antifungal stewardship efforts [39].
Table 2 presents the susceptibility profile of Aspergillus spp. to tested antifungal drugs based on the obtained MICs and the proposed ECVs for Aspergillus spp. (Supplementary file; Table S3, S5, S6, S7). Notably, 25% (4/16) of Aspergillus isolates exhibited a MIC above the ECV of 2 µg/mL recommended for A. fumigatus when tested against AmB. Alarmingly, all A. flavus isolates from the hospital environment had an MIC of > 2 µg/mL against AmB, indicating a concerning trend of emerging drug resistance among A. flavus. This finding aligns with the results of Moslem et al. (2020), who also reported resistance to AmB in environmental A. flavus isolates [40]. Additionally, one isolate each of A. tubingensis and A. luchuensis showed resistance to VRC (MIC > 1 µg/mL). All other species demonstrated drug sensitivity. Our results also showed no resistance of Aspergillus spp. to ITC and CAS (Table 2). Consistent with our findings, a study on Aspergillus spp. isolated from hospital surfaces and equipment in Iran showed no resistance in A. flavus isolates to VRC and ITC. In contrast, about half of A. fumigatus isolates had an MIC ≥ 2 µg/mL against VRC and ITC and some strains of A. tubingensis, A. luchuensis, and A. niger were resistant to ITC [14]. Ghazanfari et al. (2023) reported that, of the nine A. tubingensis isolates obtained from environmental samples (instruments and air) from different wards in four educational hospitals in Mazandaran Province, Iran, 22.2% and 44.4% exhibited an MIC of ≥ 2 µg/mL against VRC and ITC, respectively [15]. Manharpreet Kaur et al. (2024) found that 5% (3/62) fungal isolates from hospital environments had an MIC of > 2 µg/mL for AmB [24]. Monpierre et al. (2021) observed that only two out of 51 environmental Aspergillus isolates were azoles-resistant [41]. Overall, the azole resistance in hospital environmental isolates of Aspergillus, highlights a threat to patients, who are vulnerable to invasive aspergillosis.
Table 3 demonstrate the susceptibility profile of Rhizopus spp. to tested antifungal drugs based on the obtained MICs and proposed ECVs for R. arrhizus (Supplementary file; Table S3, S4, S6, S8). According to the MICs of tested antifungal drugs for Rhizopus spp., 25% (1/4) of Rhizopus isolates from environmental samples were resistant to AmB, with MIC values exceeding the ECV for R. arrhizus (Table S3). This isolate also showed resistance to ISC and PSC while no resistance was detected against ITC according to ECVs recommended for R. arrhizus [42].
Table 2 Susceptibility profile of Aspergillus spp. to tested antifungal drugs (resistance indicates the isolates with MIC greater than the ECV proposed for Aspergillus spp. against the specific antifungal drug)Table 3 Susceptibility profile of Rhizopus spp. to tested antifungal drugs (resistance indicates the isolates with MIC greater than the ECV proposed for Rhizopus spp. against the specific antifungal drug)Efficacy of disinfectants against fungal isolatesThe misuse or inappropriate concentration of disinfectants can lead to suboptimal decontamination in hospital environments, posing a health risk to patients by allowing the persistence of opportunistic or pathogenic microorganisms. Recent studies have indicated that continuous exposure to sublethal concentrations of disinfectants can lead to microbial resistance, and in some cases, co- or cross-resistance to antimicrobial drugs [43]. Table 4 details the effects of nine disinfectants on Aspergillus spp. and Mucorales isolates from air and exhaust vent surfaces across various hospitals. The fungi exhibited a broad sensitivity spectrum, with some isolates showing no inhibitory zone and others displaying zones up to 26 mm. Resistance to disinfectants ranged from 43.5 to 73.9%, with IS and SHI showing the highest and lowest resistance, respectively. Figure 3 illustrates that Aspergillus spp. had high resistance to many disinfectants, while Rhizopus spp. were resistant to all tested agents. These findings underscore the need for further research into disinfectants capable of effectively eradicating fungal spores.
Table 4 Sensitivity analysis of fungal species isolated from the environmental samples (frequency) to common disinfectantsFig. 3
Network analysis of simultaneous resistance to antifungal drugs and disinfectants of environmental isolates of a) Aspergillus spp. b) Rhizopus spp. (The size of nodes and the width of edges is related to the relative abundance of resistant fungi)
Interestingly, isolates of the same species collected from different environments (air and exhaust vents) responded differently to disinfectants. For example, A. flavus and A. tubingensis from air samples were relatively sensitive to most disinfectants, whereas their counterparts from exhaust vents exhibited greater resistance. This increased resistance among exhaust vent isolates may be attributed to prior disinfectant exposure. The CDC reports that environmental Aspergillus can develop resistance to antifungal drugs following exposure to fungicides similar to medical antifungals, raising significant concerns about patient inhalation of these resistant spores. Consequently, it is crucial to employ disinfectants that effectively eliminate fungi on surfaces, as exposure to sublethal fungicide concentrations may induce antimicrobial resistance.
Network analysis of simultaneous resistance in Aspergillus spp. and rhizopus spp. to antifungal drugs and disinfectantsThe presence of fungal pathogens in hospital environments, coupled with their simultaneous resistance to both antifungal drugs and disinfectant agents, raises significant concerns for the care of vulnerable patients. As depicted in Fig. 3a, Aspergillus spp. exhibited the highest resistance (25%) to AmB, with 100% of the species also showing resistance to SHI, SHP, and HP disinfectants. Notably, Aspergillus spp. did not exhibit resistance to CAS and ITC. Furthermore, 37.5% of isolates resistant to disinfectants did not show resistance to antifungal drugs, suggesting that, fortunately, these species are not yet drug-resistant. Additionally, Fig. 3b shows that one isolate of R. arrhizus which was simultaneously resistant to AmB, ISC, and PSC also demonstrated resistant to all tested disinfectants, highlighting the simultaneous resistance of Mucorales to both antifungal drugs and disinfectants. The simultaneous resistance of Aspergillus spp. and Mucorales to antifungal drugs and disinfectants may pose a significant challenge in controlling IFDs in hospital environments, necessitating further research in the future.
Clinical cases of aspergillosis and mucormycosisInvestigating the sources of aspergillosis and mucormycosis infections in healthcare settings is particularly challenging due to patients’ complex medical histories and the uncertain incubation period of these IFDs [43, 44]. Despite these challenges, the significance of nosocomial mycoses led us to investigate the potential role of hospital environment in acquiring of fungal infections. We compared environmental data with clinical cases in two hospitals (Hospital No. 1 and Hospital No. 5), which had the highest reports of invasive aspergillosis and mucormycosis cases. As detailed in Table S9, 23 cases were identified, with the majority occurring in Hospital No. 1. Notably, the species of Aspergillus and Mucorales most frequently identified in clinical cases mirrored those found in the environmental isolates (Tables 2 and 3, and S9). This similarity may indicate that the hospital environment could be a potential source of nosocomial fungal infections.
In environmental microbiology, antimicrobial profiling is commonly used as a phenotypic method for microbial source tracking [39]. It has been reported a rise in azole-resistant Aspergillus fumigatus among patients, reflecting an increase in azole resistance in environmental isolates [45]. Snelders et al. (2009) suggested that since inhalation of airborne Aspergillus spores is the common route of infection, the dominance of a single resistance mechanism in clinical azole-resistant isolates may indicate acquisition from a common environmental source [46]. Therefore, we compared the antifungal sensitivity profiles of similar species isolated from both the environment and clinical samples (Tables 2 and 3).
The antifungal susceptibility profile of clinical isolates against AmB showed that 100% of Aspergillus spp. had MIC higher than ECV for A. fumigatus, indicating resistance (Table 2). A review by Fakhim et al. (2022) reported that approximately 25% of clinical Aspergillus spp. are resistant to AmB [47]. Our results also indicated that all Rhizopus spp. isolates are resistant to ISC (Table 3). Notably, all clinical A. flavus isolates exhibited resistance to AmB, consistent with the antimicrobial resistance pattern of A. flavus isolates from environmental samples. Furthermore, two R. arrhizus isolates from clinical samples shared an antimicrobial profile with an R. arrhizus environmental isolate, showing resistance to both AmB and ISC.
Although our findings revealed more resistance in clinical isolates, the comparable antifungal resistance profiles of clinical and environmental isolates of A. flavus and R. arrhizus underscores the potential role of the hospital environment as a source of nosocomial fungal infections. It is noteworthy that at least two-thirds of patients with azole-resistant infections have not received prior azole therapy, suggesting an environmental route of acquisition [45]. Snelders et al. (2009) provided evidence that patients with invasive aspergillosis due to azole-resistant A. fumigatus likely acquired the fungus from the environment [46]. In another study of four cases of mycotic endocarditis among open-heart surgery patients within a single year, including one case involving Mucor sp., investigators discovered Mucor sp. and Aspergillus sp. in dust from an air conditioner duct and in air samples. They concluded that the air filter in use was likely insufficient to trap spores [44].
Mitigating the risk of transmission of fungal sporesTo mitigate the risk of nosocomial transmission of Aspergillus and Mucorales through hospital environments, it is imperative to implement infection control measures swiftly to curb their spread in healthcare settings. Contaminated surfaces with fungal growth may be a significant source for the release of fungal spores and subsequent acquisition of fungal infections. Therefore, healthcare facilities must follow strict cleaning protocols, especially for humid surfaces such as exhaust vents.
A major challenge in clinical wards is preventing the entry of fungi that are ubiquitous outdoors. By keeping windows closed and employing high-efficiency particulate air (HEPA) filters in areas housing high-risk patients, it is feasible to improve air quality within clinical units.
During the disinfection process of hospital environments, it is crucial to assess both the efficacy and appropriate concentration of disinfectants to combat opportunistic and pathogenic microorganisms. This evaluation is particularly vital for controlling resistance mechanisms, which may develop due to repeated exposure to sub-lethal concentrations of antimicrobial agents.
Since, transmission-based precautions are a critical component in the prevention and control of airborne pathogens, such as Aspergillus and Mucorales [48], proactive environmental surveillance to identify potential sources of fungal spores before they lead to infections is a key strategy in high-risk wards. Regular monitoring, combined with appropriate infection control measures, can help to minimize the risk of fungal transmission in healthcare settings.
Comments (0)