IPEH was originally designated as “vegetant intravascular hemangioendothelioma” by Masson and he regarded it as a true neoplasm with intermediate malignancy (applying the recent WHO nomenclature). Although it turned out very soon after the initial description that this is a benign lesion, nevertheless the debate whether it is a true neoplasm or a reactive vascular proliferation continued. However, even if many pathologists accepted the “reactive” nature of this peculiar lesion, clinically it appears as a true neoplasm, especially because of its relatively high recurrence rate.
Pathogenesis of the tumor is not clear. It may appear de novo or they may form in association with or on the basis of other pre-existing vascular lesions or it can be in extravascular form which arises in a hematoma. Other investigators [21] have argued that thrombosis occurs prior to papillary growths and the following fibrin deposition acts as a substrate for the IPEH development. Fibroblast Growth Factor and fibrinous deposits have also been proven to induce the process [25, 30]. Levere et al., [16] however, proposed an autocrine etiology of post-traumatic IPEH, involving the fibroblast growth factor (FGF) secretion. The macrophages that reach the site of trauma release the FGF, which triggers IPEH; the endothelial proliferating cells, on their turn, release more FGF, thus activating a positive feedback loop of endothelial proliferation. [3]
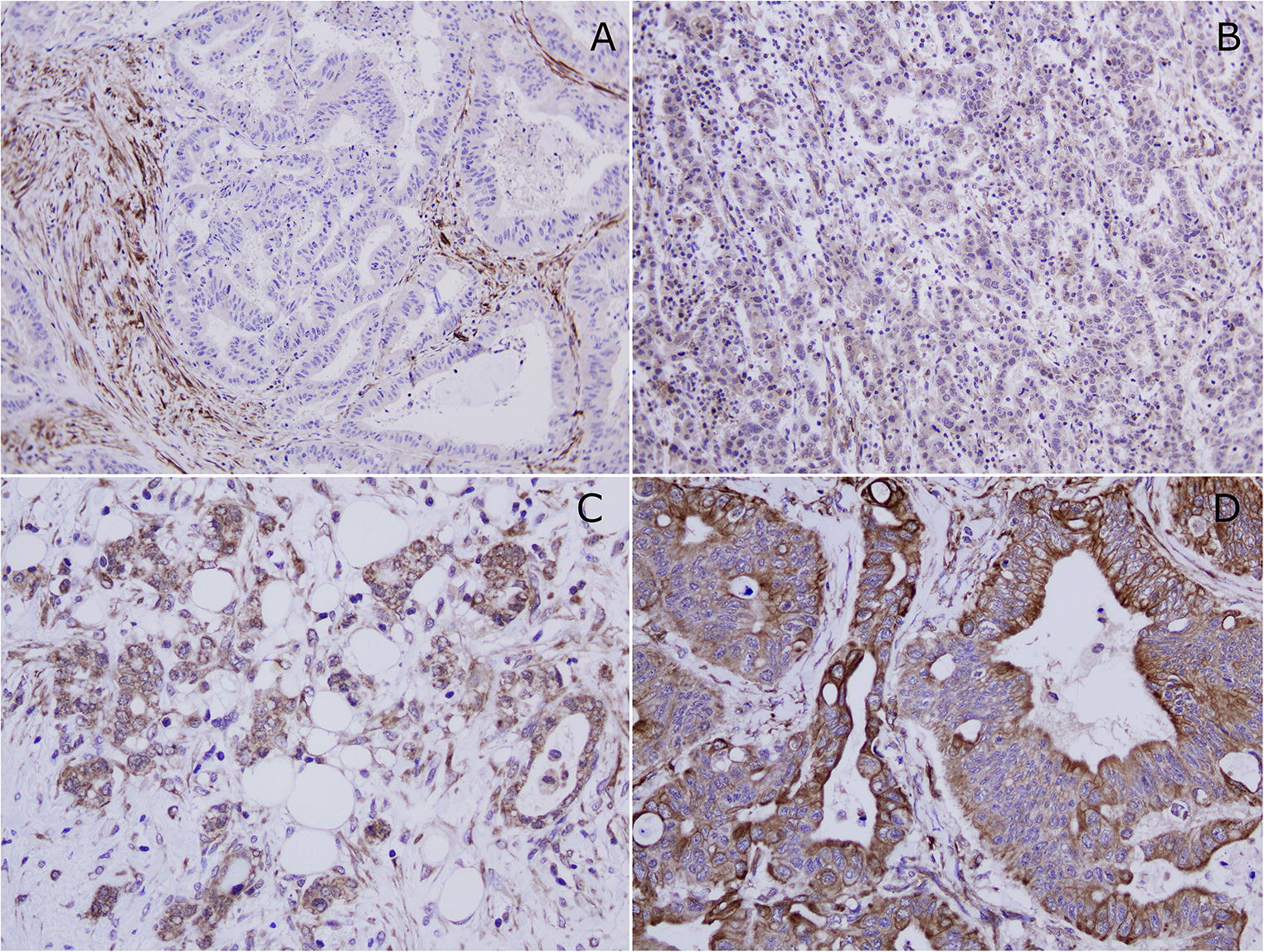
Recently, using new vascular markers combined with vascular flow parameters [23], a new classification proposal is emerging. However, no systematic examination of Masson tumor with these new vascular markers has happened so far. Currently, it is agreed that true capillary hemangioma, which is capable for spontaneous regression, should be Glut1 positive regardless of its morphological appearance [24]. Therefore, we wanted to examine the Glut1 status of our cases and no Glut1 positivity was found at all. Spontaneous regression can be characteristic for some benign tumor and also for some reactive proliferation but in our cases, we found negativity which is against indirectly to the proliferative nature of the Masson tumor. Cytoplasmic WT1 positivity is characteristic for normal endothelial cells and can be observed in many benign vascular tumors. Interestingly, Timar et al. found that malignant vascular tumors are more frequently positive with WT1 as compared to benign ones [2]. On the other hand, Al Dhaybi et al., evaluating the expression of WT1 in 126 vascular lesions, found that WT1 positivity allows the distinction of vascular tumors from vascular malformations [29]. WT1 positivity of our cases proves that Masson tumor is not a vascular malformation and also favours the concept of true neoplasm. Pericytes have an important role in the formation of vascular tumors. Usually benign vascular tumors can be characterized by the accompanying pericytes, however, the lack of a pericytic layer is quite specific for the malignant vascular tumors. Because Masson tumor is a benign entity and pericytes may appear both in proliferative and benign vascular lesions (but it is more characteristic for benign ones), the presence of pericytic layer also speaks for the neoplastic nature.
Considering the long-standing condition of Masson tumor, the relatively high recurrence rate, the appearance in preexisting vascular tumors, the Glut1 negativity and WT1 positivity and the accompanying pericytic layer and furthermore the constant positivity with different vascular markers (CD31, ERG), it seems that Masson tumor begins as a proliferative process but with time it transforms into a true benign neoplasm. It is also important to consider Masson tumor as a benign tumor because the possibility for further transformation into a malignant one cannot be excluded, however, there has been no report of this phenomenon so far.
In our series, pre-operative radiological examinations were unable to establish the exact diagnosis of Masson’s tumor - even the FNAB did not point directly to this lesion. Our 7 cases also demonstrate that there are 2 major etiological factors behind the IPEH. The lesion can develop de novo (5 out of 7 cases) or on the basis of pre-existing vascular malformations (hemangiomas, 2 out of 7 cases). The clinical appearance can be from no symptom to a limited of range of motion. In hand surgery, it is very important to plan the appropriate surgical solution to prevent recurrence.
The main problem during the differential diagnostic process is not that Masson’s tumor may be misinterpreted as a different benign malformation e.g.: hemangioma, but that due to radiological appearance and sometimes features of FNAB, it may be over-diagnosed. This may open the gate for overtreatment if it is presumed to be a malignant tumor (e.g.: angiosarcoma) [20, 22].
Masson’s tumor usually occurs in adults aged 30–40 years and is slightly most common in women, just as hemangiomas, suggesting a hormonal factor in development of this kind of lesions [6, 9]. Females are slightly more affected than males (ratio 1.14: 1) [9, 13] according to the literature. In our series, 4 out of 7 patients were female and the average age was 40 years. According to the literature, Masson’s tumor is a rare lesion in the hand (among other vascular tumors) [1], but we found 7 cases (5 of out 7 cases were on the fingers (thumb and ring finger); 2 of out 7 cases were on the thenar during the examined period, which is relatively high, considering that Masson’s tumor accounts for approximately up to 2%–4% of benign and malign vascular tumors of the skin and subcutaneous tissues [27, 30]. In the literature, the frequency of Masson tumor on the hand is about 7%. [5, 30]
In 2 of out 7 cases, the Masson tumor appeared in a previously present hemangioma. This is relatively high, but there is no exact ratio about it in the literature.
All 7 cases included a palpable mass and tenderness to palpation. In 4 cases, the lesion demonstrated growth which resulted in impaired finger function. Remarkably, symptoms can enhance drastically on the hand, compared to other regions of the body, since even a small lesion may interfere with harmonious hand function due to discomfort and a limited range of motion.
Marginal surgical excision is the hallmark of treatment for these lesions in the hand. Total excision would theoretically reduce the risk of recurrences. However, this may be technically difficult to perform due to location and the tumor being interwoven with the vasculature of the finger. We encountered this limitation when performing excision of expansive lesions. [7, 13] As an alternative treatment, sclerotherapy may be considered. However, due to the characteristics of the vascular anatomy of the fingers, this procedure may carry the risk of circulatory problems and even necrosis [14] of the fingers in certain cases. In our series, 2 patients had sclerotherapy but as the lesion progressed on the fingers, this was no longer an acceptable option.
FNAB was performed in one of our cases and it did not raise the possibility of Masson tumor, but suspected hemangioma. In 2 other patients who underwent diagnostic tests (US, MR) before surgery, hemangioma was suspected too. Unfortunately, neither the clinical examination, nor the FNAB could give an absolutely accurate diagnosis. The final exact diagnosis was given by postoperative histology in all 7 cases. It is difficult to plan the surgery in the absence of an accurate diagnosis, but if there is no evidence for malignancy, as it happened in our cases, the proper route can be chosen. During surgery, care should be taken of the surrounding anatomical structures; especially with digital terminal arteries because they are responsible for the blood supply of the fingers and as these may be interwoven with the vessels of the vascular tumor. Dissecting them from the vessels of the Masson tumor may be quite an intricate task.
In each case, a discussion with the patient and an individual consultation must precede the operation as these are slowly increasing lesions which cause progressive symptoms over time. Most of the symptoms are increasing pain, discomfort and consequently, a limited range of motion. Once the diagnosis has been made, patients also need to be informed regarding expected outcomes and recurrence rates, the necessity of radiological follow-up or the possibility of further operations. We plan to follow our cases every 3–6 months for 1 year, and once a year for the next 3–4 years. If clinical progression is suspected, the patient is referred for further imaging studies. Patients are also advised to register for a check-up if they notice any growth or in case if new symptoms appear. According to the literature, the expected recurrence rate of these lesions is around 15%. It has been described that if IPEH arises in a pre-existing vascular lesion, the recurrence rate depends on the technical difficulties as to how someone can remove the original vascular tumor. In our series no recurrence appeared during follow-up. However, this period was not a long-term one. We expect especially that in the patients who had pre-existing vascular lesions, recurrence may appear in the subsequent years, therefore, radiological follow-up is recommended [4, 11, 12, 18, 26]. Physiotherapy to regain range of motion and strength may be necessary.









Comments (0)