
Remember me





The clinical and laboratory features of our five patients managed with anakinra are shown in Table 1. Four were males (80%); two had a fever (40%) and none had a skin rash. Anakinra was well tolerated without significant adverse effects. All patients achieved remission and survived.
Table 1 Off-label use of anakinra in five difficult-to-treat cases: reported laboratory values were those at start of anakinra treatment3.1.1 Case 1The first patient (P1) was a male neonate, small for gestational age, prematurely born via cesarean section at 34 weeks of gestational age, with a birthweight of 1500 g. During the pregnancy, because of persistent polyhydramnios, genetic investigations led to the diagnosis of type 1 Bartter syndrome. He presented with significant polyuria from the first days of life, so at 3 weeks of life, indomethacin therapy was started. During his NICU stay, he experienced repeated sepsis episodes due to Klebsiella pneumoniae.
Despite an apparent in-vitro antibiotic regimen and negative culture tests, severe thrombocytopenia persisted, with the need for repeated platelet transfusions daily (due to bleeding). After performing a peripheral venous smear and cytofluorimetric test, a first-line therapy with intravenous IgM-enriched immunoglobulins (Pentaglobin®, 250 mg/kg/day for 3 days) was given, but unsuccessfully. The patient continued to have thrombocytopenia and also developed hyporegenerative anemia, hyperferritinemia, hypofibrinogenemia, increased C-reactive protein, increased CXCL9 and CXCL10, hepatosplenomegaly with ascitic effusion, need for mechanical ventilation and inotropic support, and significant worsening of renal function. Secondary HLH after Klebsiella pneumoniae infection was suspected, and a bone marrow aspirate sample was taken, showing poor cellularity, mainly represented by macrophage elements with intracytoplasmic foamy vacuoles and absence of erythroblasts and megakaryocytes. Functional assays also showed greatly reduced natural killer (NK) cell degranulation with insufficient cytotoxicity. Therefore, intravenous therapy with anakinra (10 mg/kg/day in two doses) and methylprednisolone with two initial boluses of 30 mg/kg/day, reduced to 2 mg/kg/day due to the appearance of arterial hypertension, was started. We documented a rapid decrease in inflammatory biomarkers and an increase in platelets and white blood cell counts. We could also wean the patient from mechanical ventilation; we witnessed a clear reduction in hepatosplenomegaly and the fever disappeared.
Additionally, genetic testing detected the heterozygous variant of uncertain significance, c.272C>T, in the PRF1 gene, which at the protein level determines the amino acid change p.Ala91Val (rs35947132), which cannot be related to primary HLH to date. An extensive work-up excluded a primary immunodeficiency.
After 4 months of anakinra (initially intravenously and then subcutaneously) and glucocorticoid therapy (methylprednisolone 1 mg/kg/day intravenously, then orally and then gradually tapered), NK function tests showed a clear improvement, and CXCL9 and CXCL10 returned to normal values. Therefore, the therapy was gradually reduced until complete suspension 5 months after the start. The baby was discharged without any flare in a 3-year follow-up period.
3.1.2 Case 2The second patient (P2) was a male preterm neonate born via cesarean section at 23 weeks + 4 days of gestational age by a twin pregnancy, with a birthweight of 550 grams. The patient developed late-onset sepsis at a postmenstrual age of 35 + 6 weeks, with a blood culture revealing Enterobacter cloacae. Based on the antibiogram, a course of meropenem and amikacin was given for 14 days, and intravenous IgM-enriched immunoglobulins (Pentaglobin®, 250 mg/kg/day for 3 days) were administered. The infant failed to improve despite receiving in-vitro antibiotics, with respiratory distress requiring mechanical ventilation and hemodynamic instability until septic shock. Additionally, he developed severe thrombocytopenia (2 × 109/L) resistant to platelet transfusions. Repeated blood cultures showed persistence of the same bacterial strain, and many antibiotic courses were employed in an attempt to eradicate it. After 40 days of antibiotic therapy, the emergence of a strain of Enterobacter cloacae CTX-M extended-spectrum β-lactamase was reported. Thus, the antibiotic treatment was shifted to a triple regimen with meropenem, tigecycline, and gentamicin, with subsequent negative culture approximately 2 months after the onset of the sepsis.
However, the general condition of the infant did not improve, with a systemic inflammatory response (SIRS) characterized by the persistence of elevated inflammatory markers despite negative cultures. An extensive laboratory work-up showed leukopenia, thrombocytopenia, hyperferritinemia, and hypofibrinogenemia, whereas abdominal ultrasound documented hepatosplenomegaly. Because of suspicion of a secondary hemophagocytic lymphohistiocytosis (HLH) induced by bacterial sepsis, bone marrow aspirate was performed, showing hemophagocytic activity of blood cells with a 56% HLH-like (CD8+CD38 high HLA DR+) population. Peripheral blood smear did not show blasts. In addition, slightly reduced NK cell degranulation and cytotoxicity were detected in a further immunological assessment. An anti-inflammatory therapy was started with dexamethasone (0.8 mg/kg/day in two doses) and anakinra (10 mg/kg/day in two doses intravenously). We documented a rapid decrease in inflammatory biomarkers and a normalization of platelet count and white blood cell count, which was associated with a rapid reduction in splenomegaly and with a favorable evolution of respiratory symptoms and successful extubation. The genetic work-up for HLH tested negative. Dexamethasone (0.1 mg/kg/day and then gradually tapered) was given for a total of 24 days, and anakinra was given initially intravenously and then subcutaneously three times per week upon discharge at about 6 months of corrected age, without any inflammatory relapses. The baby will be weaned from anakinra during follow-up.
3.1.3 Case 3The third case (P3) was a full-term newborn (38 weeks, birthweight 3070 g) referred to our hospital because of multiple congenital anomalies: interruption of the aortic arch type A, patent ductus arteriosus, ventricular septal defect, right hydronephrosis and left multicystic kidney, cleft lip, and left vocal cord paralysis. He underwent cardiac surgery at 6 days of life. He postoperatively developed increasing pericardial effusion, requiring pericardiocentesis on the second postoperative day (about 40 mL of citrine liquid). The child also presented with chylothorax, which required drainage. The genetic work-up for genetic fever syndromes or collagen disorders was negative.
After a multidisciplinary discussion, given the persistence of polyserositis (despite drainage) associated with increased inflammatory markers (in the absence of infections), the child was treated with anakinra (10 mg/kg once/day, subcutaneously) for 15 days with complete resolution of pleural and pericardial effusion.
At about 2 months of age, as a result of persistent fever and increased inflammatory markers, and in the absence of any evidence of infection, it was indicated to resume a course of anakinra to be continued for 12 months until further discussion with the cardiothoracic surgeons to establish the surgical program. A rapid clinical improvement was observed with the disappearance of fever and normalization of inflammation indices. The absence of pericardial effusion was confirmed on the last echocardiogram before discharge. He was discharged at about 9 months of life in good condition, with no evidence of polyserositis.
3.1.4 Case 4The fourth case (P4) was a male neonate, born at 37 weeks’ GA via vaginal delivery from a medically assisted pregnancy (embryo donation), complicated by insulin-dependent gestational diabetes and SARS-CoV-2 infection that occurred in the last month of gestation. At birth, the neonate developed progressive respiratory distress and pulmonary hypertension, poorly responsive to mechanical ventilation (synchronized intermittent positive pressure ventilation and then high-frequency oscillatory ventilation) and pulmonary vasodilator therapies (inhaled nitric oxide, milrinone, diuretics, sildenafil, and bosentan). Due to the insufficient response to these treatments, the baby required extracorporeal membrane oxygenation (ECMO) for 7 days. Antibacterial therapy was administered, suspecting septic shock secondary to a vertical infection. All cultures (blood, urine, bronchoalveolar lavage) were negative. Metabolic tests (urine organic acids, plasma acylcarnitine, amino acids, purines, pyrimidines, homocysteine) were within normal range. Genetic analysis was negative for surfactant protein deficiency, primary ciliary dyskinesia, and cystic fibrosis. A heterozygous missense mutation in gene KCNK3 (c.607G>A; p.Gly203Ser) was found and was considered as probably pathogenetic (class 4), according to current knowledge. Indeed, the gene KCNK3 (Potassium Two Pore Domain Channel Subfamily K Member 3) is a protein-coding gene, and its mutations have been associated with primary pulmonary hypertension [16].
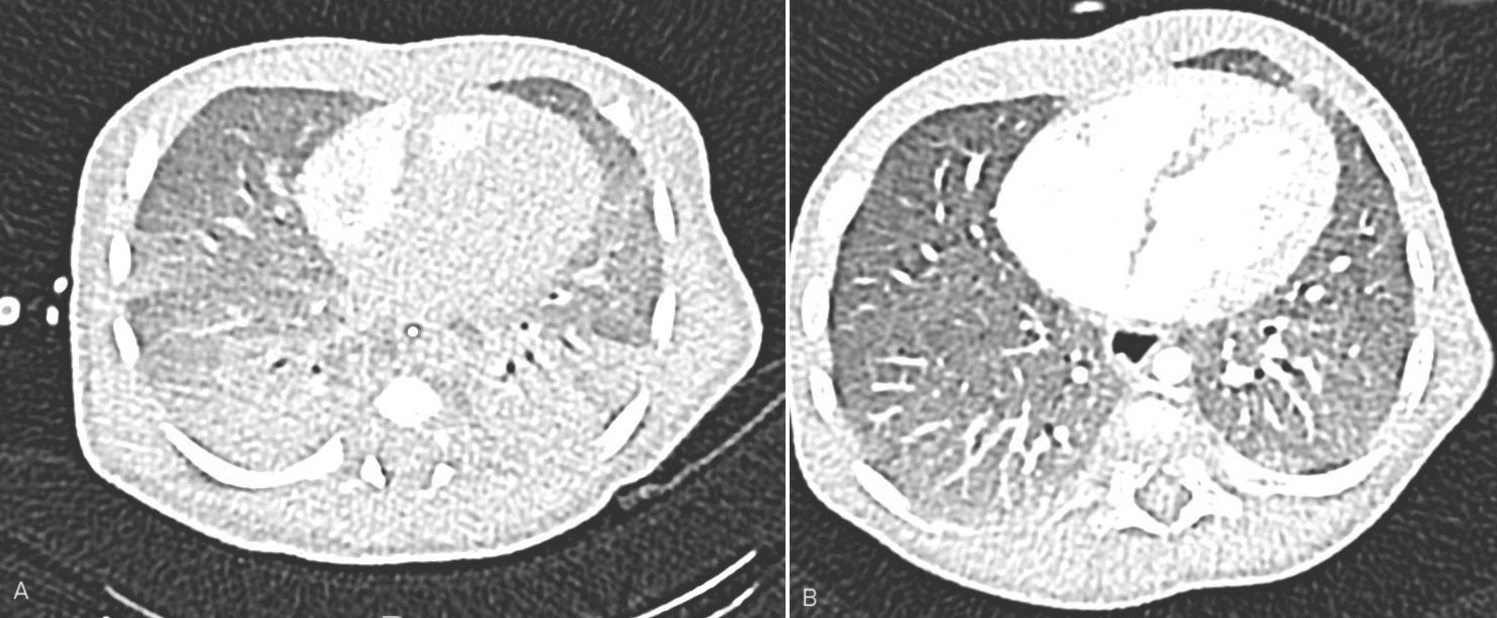
Pulmonary computed tomography (CT) performed on day 38 of life showed severe bilateral dysventilation with consolidative areas (Fig. 1a). Considering the persistent need for ventilatory support and oxygen supplementation, the KCNK3 mutation and the anamnestic data about maternal SARS-CoV-2 infection during pregnancy, suspecting a component of inflammatory pulmonary interstitial disease, treatment with anakinra (10 mg/kg/day, intravenously) was administered beginning on the 31st day of life and continued for 43 days. Both clinical and radiologic improvements were soon recorded, including successful weaning from mechanical ventilation. Overall, the infant required 35 days of invasive ventilation, and afterward, non-invasive ventilatory support was provided (nasal-IPPV, CPAP) and was progressively decreased. Pulmonary CT, repeated at 3 months of life and after 2 months from the start of therapy with anakinra, demonstrated a significant decrease in pulmonary consolidative areas (Fig. 1b). The infant was discharged from NICU at 4 months of life with domiciliary administration of low-flow oxygen delivery. He is now 2 years old and still needs low-flow oxygen during the night (0.25 L/min). Neurological development and anthropometric growth are within normal limits.
Fig. 1
Pulmonary computed tomography (CT) performed in patient P4 showed severe bilateral dysventilation with consolidative areas on the 38th day of life (a) and a significant decrease in pulmonary consolidative areas at 3 months of life (b)
3.1.5 Case 5The fifth case (P5) was a female neonate, born at 39 weeks’ GA via vaginal delivery from a physiologic pregnancy. At birth, meconium-stained amniotic fluid was detected. However, she had a normal transition to extrauterine life, with an Apgar score of 8 in the first minute and 9 in the fifth minute. Within the first hour of life, she presented respiratory failure requiring oxygen and surfactant treatment, as well as mechanical ventilation. Due to hemodynamic instability, inotropic support was added. Despite medical treatment, the clinical conditions worsened, and the baby was placed on veno-arterial ECMO and transferred to our center.
The patient was able to be weaned off ECMO after 7 days, but mechanical ventilation was still necessary. Intravenous sildenafil infusion and inhaled nitric oxide therapy were started because of persistently increased pulmonary pressure. Extensive microbiological work-up excluded sepsis and neonatal pneumonia (repeated negative broncho-alveolar lavage). A pulmonary CT scan confirmed the extensive interstitial lung disease shown on the first chest X-ray (Fig. 2).
Fig. 2
The first chest X-ray at birth showed signs of respiratory distress (a), with pulmonary computed tomography (CT) highlighting an extensive interstitial lung disease (b)
Genetic analysis was negative for surfactant protein deficiency, genetic pulmonary hypertension, and interferonopathies. All inflammatory biomarkers were negative or in normal ranges, including an autoantibodies extensive panel, C3, C4, and sialic-acid-binding Ig-like lectin 1 (SIGLEC-1).
She failed extubation twice, although administered steroids (betamethasone, 0.1 mg/kg/day). Considering the CT scan findings and the non-benefit from steroidal therapy, treatment with anakinra (10 mg/kg/day in two doses, subcutaneously) was administered beginning on the 62nd day of life and continued until discharge. A few days after the first administration of anakinra, it was possible to wean the patient from mechanical ventilation, and we observed rapid radiological improvements. Overall, the infant required 20 days of invasive ventilation, and afterward, non-invasive ventilatory support was provided and progressively decreased. She was discharged from NICU at 3 months of life without the need for respiratory support or oxygen therapy. She continued taking anakinra at home with slow taper and a suspension after a further 4 months of therapy.
3.2 Review of the LiteratureThe literature reported 12 cases before our five cases, from 1990 onwards [17,18,19,20,21,22,23,24,25,26]. We summarized these cases of neonates and infants treated with off-label anakinra in Table 2.
Table 2 Previously published cases of off-label use of anakinra in neonates and infants up to 3 months of age. Cases are reported according to diagnosisThere were four published reports (33.3% of the cases) of off-label use of anakinra for secondary HLH or MAS [18, 20,21,22], in addition to P1 and P2 reported here; five cases of MIS-C (41.7%) [17, 23, 25]; and three cases of Kawasaki disease (25.0%) [19, 24, 26]. We also reported one case of chronic lung disease with pulmonary hypertension, one case of interstitial lung disease with pulmonary hypertension, and post-surgical polyserositis in a further case.
Among all these patients, five infants (29.4%) were born preterm and nine (52.9%) had fever. anakinra was effective in 14/17 (82.4%) infants; all the responders survived and were discharged from the NICU.
Comments (0)