
Remember me


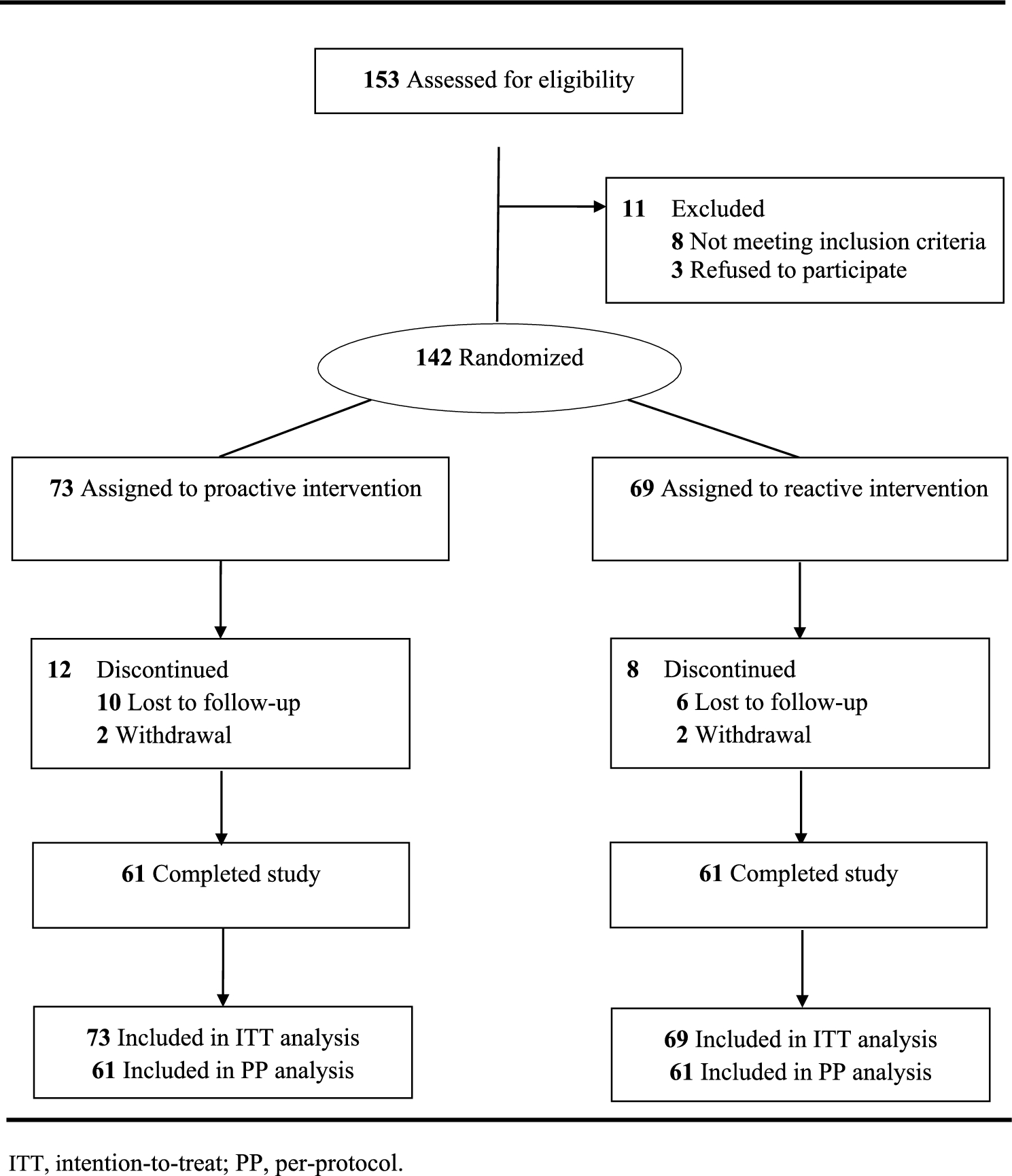



We identified 451 related records, of which 318 remained after removing duplicates (Fig. 1). Based on the abstract review, 289 records were excluded, and one could not be retrieved in full text. After thoroughly reviewing the full texts, an additional 28 articles were excluded, with the most common reason for exclusion being the inclusion of pregnant subjects. Ultimately, 12 eligible studies involving 1302 subjects met the inclusion criteria, including six RCTs [26,27,28,29,30,31] and six single-arm studies [32,33,34,35] (Table 1). The quality assessment showed that five RCTs were at a low risk of bias, and single-arm studies scored between 12 and 13, indicating that the included studies were acceptable (Tables S4 and S5 in the supplementary material). Subjects in five trials received weight- and age-adjusted oral doses of rivaroxaban equivalent to 10–20 mg for adults (NCT01684423, NCT02234843, NCT02309411, NCT02564718, NCT01145859). One trial (NCT02846532) administered a fixed dose of rivaroxaban based on body weight. Two studies (NCT02369653, NCT02981472) of apixaban determined doses based on weight groups, including weight-adjusted or fixed doses. Another study (NCT01707394) provided weight-adjusted apixaban to achieve adult steady-state exposure with apixaban 2.5 mg. One study (NCT02798471) on edoxaban used a fixed dose based on age groups. Additionally, two studies (NCT03395639, NCT02303431) administered fixed doses to subjects aged between 12–18 years and those aged between 6–18 years, and used weight-adjusted doses in younger subjects. The age- and body-weight-adjusted dosages of FXa inhibitors are shown in Table 2. The quality of all studies was acceptable (Table S4 and S5 in the supplementary material).
Fig. 1
Flow diagram of meta-analysis
Table 1 Characteristics of eligible studiesTable 2. Factor Xa inhibitor age- and weight-adjusted dosing regimens3.1.2 Safety OutcomesThe overall pooled incidence of AEs and serious AEs in pediatric patients using FXa inhibitors were 50.6% (95% CrI 33.1–67.2, τ = 0.80) and 9.9% (95% CrI 3.9–19.5, τ = 0.55), respectively (Fig. 2). To explore potential heterogeneity among the drugs, we conducted a subgroup analysis. An estimated 55.0% (95% CrI 27.0–78.9, τ = 0.67) of patients treated with rivaroxaban experienced at least one AE, compared with 56.8% (95% CrI 22.0–87.6, τ = 0.67) for apixaban and 35.5% (95% CrI 10.1–68.0, τ = 0.83) for edoxaban. The incidence of serious AEs was 10.4% (95% CrI 2.6–24.3, τ = 0.71) for rivaroxaban, 19.3% (95% CrI 3.3–50.7, τ = 0.82) for apixaban, and 7.5% (95% CrI 0.6–28.8, τ = 0.43) for edoxaban. Four studies (NCT02369653, NCT03395639, NCT02846532, NCT02981472) allowed the administration of experimental drugs to patients without prior exposure to the other anticoagulants. The incidence of AEs and serious AEs in patients who did not receive other anticoagulants was 65.7% (95% CrI 36.3–87.7, τ = 1.18) and 22.0% (95% CrI 6.0–50.7, τ = 0.88), respectively (Fig. 2). These rates were higher than those in patients who had previously received other anticoagulants. Six studies (NCT02234843, NCT02369653, NCT02981472, NCT01707394, NCT02798471, NCT03395639) did not report age-specific AEs, and one study (NCT02846532) focused on subjects aged 2–8 years, which did not fit into any specific age group. AE rates were 25.2% (95% CrI 5.9–56.3, τ = 0.78) for the birth to 6 years age group, 45.8% (95% CrI 15.0–80.8, τ = 0.84) for the 6–12 years age group, and 43.4% (95% CrI 9.2–83.3, τ = 0.49) for the 12–18 years age group (Fig. 2). The incidence of serious AEs was 2.4% (95% CrI 0.2–8.6, τ = 0.67), 2.4% (95% CrI 0.1–10.7, τ = 0.96), and 2.7% (95% CrI 0.0–13.5, τ = 0.65) from the youngest to the oldest age groups.
Fig. 2
Incidence of adverse events and bleeding-relevant adverse events. CrI credible interval, CRNM clinically relevant non-major
The estimated rate of major and CRNM bleeding was 2.4% (95% CrI 0.8–4.8, τ = 1.61). The incidence of major and CRNM bleeding was 2.8% (95% CrI 0.4–8.8, τ = 0.64) for rivaroxaban, 4.3% (95% CrI 0.3–19.0, τ = 0.70) for apixaban, and 2.1% (95% CrI 0.1–9.5, τ = 0.72) for edoxaban. The estimated incidence of major and CRNM bleeding was 1.9% (95% CrI 0.3–6.2, τ = 0.69) for patients who had previously received other anticoagulants compared with 3.0% (95% CrI 0.4–10.4, τ = 1.46) for those who had not received them. Because of the limited data, an age subgroup analysis for major and CRNM bleeding was performed.
In total, over 100 AEs were reported in the eligible studies, but only AEs reported by more than two studies were included in our meta-analysis. Estimates for the top 30 non-hemorrhagic AEs and the top 20 bleeding AEs are presented in Fig. 3. The most common non-hemorrhagic AEs were pyrexia at 9.2% (95% CrI 4.6–15.3, τ = 1.18), vomiting at 7.8% (95% CrI 4.0–12.3, τ = 0.08), and abdominal pain at 7.4% (95% CrI 1.5–19.4, τ = 0.84). The incidence of any bleeding event was 20.7% (95% CrI 5.1–46.1, τ = 0.75). Nine non-composite hemorrhagic AEs had rates of over 1%. The most common bleeding AE was epistaxis at 8.4% (95% CrI 3.9–14.9, τ = 1.96), followed by subcutaneous hematoma at 6.4% (95% CrI 0.5–26.2, τ = 0.54) and wound hemorrhage at 3.7% (95% CrI 0.4–13.3, τ = 0.55) (Fig. 3). Heterogeneity (τ) was < 1.5 for all AEs except fatigue, epistaxis, and major and CRNM bleeding.
Fig. 3
Incidence of A non-hemorrhagic and B hemorrhagic adverse events. CrI credible interval, CRNM clinically relevant non-major
3.2 Results of FAERS3.2.1 AEs in FAERSA total of 20,755,633 reports were retrieved from FAERS, documenting 672 AEs in patients aged < 18 years (Figure S1 in the supplementary material). The first report of AEs in pediatric patients receiving FXa inhibitors was recorded in 2012, followed by a rapid increase in such events (Fig. 4). As shown in Table S6 in the supplementary material, a total of 279 pediatric patients were involved in all the reports, with a median age of 7 years. Among these patients, 131 (46.95%) were female, 125 (44.80%) were male, and 23 (8.24%) had an unknown gender. Most patients were from North America (138 [49.46%]), followed by Europe (91 [32.62%]), and Asia (19 [6.81%]). Reporting individuals were primarily physicians (90 [32.26%]), followed by consumers (85 [30.47%]), and pharmacists (74 [26.52%]). The three most common indications were unknown indication (95 [34.05%]), deep vein thrombosis (38 [13.62%]), and thrombosis prophylaxis (20 [7.17%]). A total of 217 (77.8%) cases were classified as serious AEs, with 115 (41.22%) resulting in initial or prolonged hospitalization. The numbers of reported AEs for rivaroxaban, apixaban, and edoxaban were 175 (62.72%), 102 (36.56%), and 2 (0.72%), respectively.
Fig. 4
Number of adverse event reports for factor Xa inhibitors from the US Food and Drug Administration Adverse Event Reporting System database
3.2.2 Scanning for AEsA total of 39 AE signals were identified according to the 2.2.2 criteria (Table 3). The most frequently reported AEs were off-label use, accidental exposure to the product by children, and deep vein thrombosis, with 37, 28, and 18 cases, respectively. A disproportionality analysis was conducted using the full FAERS database, but edoxaban was not individually analyzed because it had fewer than three cases (Fig. 5). The top three highest overall ROR for AEs were observed for hemorrhoidal hemorrhage (1211.82 [95% CI 312.69–4696.29]), thrombophlebitis (134.64 [95% CI 42.18–429.81]), and deep vein thrombosis (68.3 [95% CI 42.53–109.68]). All AEs were categorized into bleeding, thrombosis, and other AEs (Table S7 in the supplementary material). Bleeding AEs with higher ROR values included heavy menstrual bleeding (17.91 [95% CI 8–40.11]) and hematuria (15.65 [95% CI 6.99–35.05]). Thrombotic AEs with higher ROR values included ischemic stroke (66.27 [95% CI 21.04–208.72]).
Table 3 Signal strength of adverse events (AEs) of factor Xa inhibitors in pediatric patientsFig. 5
Scanning adverse events for factor Xa inhibitors based on the US Food and Drug Administration Adverse Event Reporting System database. NA not applicable, ROR relative odds ratio
3.2.3 Descriptive Analysis of Cases with AEsWe performed a descriptive statistical analysis of the clinical characteristics of patients (Table 4). Among those experiencing thrombosis AEs, the median age was the highest at 16 years, followed by patients with bleeding AEs at 11 years; those with other AEs had the lowest median age at 7 years. For patients whose age and drug dosage were disclosed, those experiencing bleeding AEs had the lowest mean dosage per kilogram of body weight, with rivaroxaban at 0.16 mg/kg and apixaban at 0.08 mg/kg. The characteristics of patients using edoxaban were not presented individually because of the small sample size. The median time to onset was 6 days for the bleeding AEs and 18 days for the thrombosis AEs. The Kaplan–Meier survival curve is shown in Fig. 6.
Table 4 Characteristics of patients with adverse events (AEs).Fig. 6
Kaplan–Meier survival curve of bleeding and thrombosis adverse events
Comments (0)