
Remember me



You have full access to this article via your institution.
Although CDK4/6 inhibitors have revolutionized the management of patients with locally advanced/metastatic HR+HER2−breast cancer, hematological side effects, notably neutropenia, have been challenging to circumvent. A highly selective CDK4 inhibitor has recently been shown to cause limited hematological toxicity in preclinical breast cancer models, hence enabling dose escalation in support of superior tumor control.
Three CDK4/6 inhibitors, namely, palbociclib, ribociclib, and abemaciclib, are approved by the US FDA for use in combination with hormonotherapy in patients with advanced/metastatic HR+HER2− breast cancer.1 CDK4/6 inhibitors have indeed been shown to provide an overall survival advantage to this patient population in several randomized clinical trials, de facto revolutionizing the clinical management of HR+HER2− breast cancer.1 However, hematological side effects including neutropenia have been concerning, on one hand limiting dose escalation, and on the other hand imposing the development of an intermittent treatment regimen predicated on monthly cycles that involve three weeks on and one week off treatment (in support of hematological reconstitution).1 At least partially related to these obstacles, acquired resistance mechanisms have limited the clinical benefits afforded by CDK4/6 inhibitors to patients with HR+HER2− breast cancer, calling for the development of novel strategies to safely improve disease outcome in these patients. Palmer and collaborators recently reported on the activity of atirmociclib (PF-07220060), a next-generation, orally available and highly selective CDK4 inhibitor that demonstrated superior safety and hence enabled dose escalation in support of improved tumor control in preclinical models of breast cancer.2
Palmer et al. set out to investigate whether CDK4 would constitute a pharmacologically actionable entity in HR+ breast cancer, prostate cancer and Ewing sarcoma based on a bioinformatic analysis suggesting their exquisite dependence on CDK4 (but not CDK6) signaling for proliferation. Comforting the possibility that selective CDK4 inhibition could (at least partially) circumvent hematological side effects as caused by CDK4/6 blockers, human bone marrow mononuclear cells were insensitive to CDK4 depletion by RNA interference (but succumbed to selective CDK6 or dual CDK4/6 depletion), correlating with considerably higher expression levels of CDK6 over CDK4. Based on these observations, Palmer et al. profiled the activity of atirmociclib to demonstrate superior substrate selectivity for CDK4 over palbociclib in biochemical assays, as well as (1) preserved cytostatic activity against human HR+HER2− breast cancer cells, and (2) considerably reduced antiproliferative effects against human CD34+ hematopoietic stem/progenitor cells (HSPCs). Such an HSPC-sparing effect of atirmociclib was confirmed in dogs, a setting in which tolerable neutropenia was documented with a ~ 30-fold increased dose of atirmociclib vs palbociclib.2
While palbociclib at clinically relevant plasma concentrations (∼30 nM) exhibited poor efficacy in preclinical models of CDK4-dependent tumors in vitro, escalating atirmociclib concentrations to clinically relevant doses (∼500 nM in vitro, 60 mg/kg twice daily in vivo) resulted in superior tumor growth inhibition largely outperforming palbociclib combined with the androgen receptor inhibitor enzalutamide in prostate cancer xenografts. Notably, while Palmer et al. identified CDK6 upregulation as a potential mechanism of resistance to selective CDK4 inhibition, atirmociclib remained more efficient than palbociclib as well as second-generation CDK4/6 blockers at suppressing the growth of human HR+HER2− breast cancer models, both in vitro and in vivo, irrespective of compensatory CDK6 upregulation. Despite such a pronounced activity, human breast cancer ZR751 xenografts started to grow again upon prolonged exposure (> 6 weeks) to atirmociclib in vivo, pointing to the development of acquired resistance. In line with previous findings with CDK4/6 inhibitors,3 CDK2 signaling stood out as a potential determinant of such a growth recovery. Moreover, atirmociclib-resistant xenografts displayed transcriptional and phosphoproteomic signatures of inflammatory and estrogen receptor (ER) signaling.2
In line with these findings, atirmociclib synergized with the ER antagonist fulvestrant at arresting in vitro and in vivo tumor growth in various human HR+HER2− breast cancer models, which was linked to the induction of cellular senescence rather than overt cell death. Moreover, atirmociclib enabled superior control of human HR+HER2− xenograft relapse (after nearly being eradicated) upon discontinuation of the ER degrader vepdegestrant. Finally, atirmociclib outperformed palbociclib as combinatorial partner for a selective CDK2 inhibitor in immunodeficient mice bearing fulvestrant-resistant, palbociclib-resistant, or palbociclib-sensitive HR+HER2− breast cancer xenografts. Such an effect was achieved with a 6-fold higher dosage of atirmociclib vs palbociclib, yet having comparable effects on HSPCs.2 Of note, atirmociclib also outcompeted palbociclib — which mediates various immunomodulatory effects4 — at promoting the upregulation of several components of the antigen presentation machinery and the co-inhibitory ligand PD-L1, at least partially linked with the activation of cellular senescence. Accordingly, atirmociclib (but not palbociclib) positively interacted with an immune checkpoint inhibitor (ICI) specific for the PD-L1 receptor PD-1 in immunocompetent mice bearing syngeneic colorectal carcinomas.2
In summary, specifically targeting CDK4 stands out as a promising option for patients with advanced/metastatic HR+HER2− breast cancer, at least in part owing to limited hematological toxicity and hence (at least some) room for dose escalation (Fig. 1). In line with these findings, early phase clinical trials have established the safety of atirmociclib tablets (300 mg BID) delivered over continuous (rather than intermittent) 28-day cycles,5 and no less than three interventional late-phase studies are currently open to assess the clinical activity of this regimen (source https://www.clinicaltrials.gov), including a randomized Phase III trial comparing atirmociclib plus letrozole to CDK4/6 inhibitors plus letrozole in patients with treatment-naïve advanced/metastatic HR+HER2− breast cancer (FourLight-3, NCT06760637).
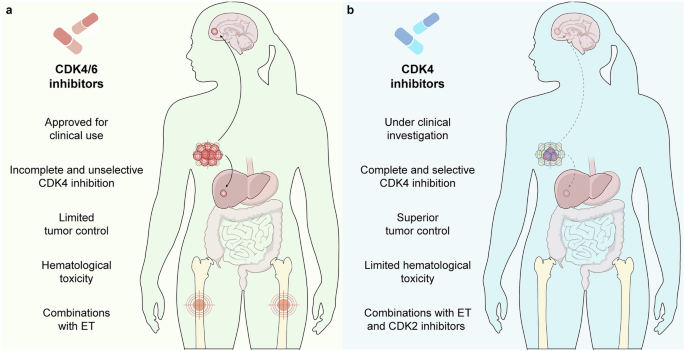
Fig. 1: Reduced toxicity may enable treatment intensification towards superior control of HR+HER2− breast cancer by selective CDK4 inhibitors.
a Currently available treatment options for advanced/metastatic HR+HER2− breast cancer target both CDK4 and CDK6, hence causing hematological side effects that constrained dose escalation and called for intermittent therapeutic regimens, potentially facilitating the emergence of acquired resistance. b Atirmociclib, a highly selective CDK4 inhibitor, effectively spares CDK6, hence being associated with limited hematological toxicity and enabling treatment intensification. Recent preclinical data support the validity of such an approach, which has already been cleared for safety in early phase clinical trials, pointing to selective CDK4 inhibition as a promising strategy for patients with advanced/metastatic HR+HER2− breast cancer. ET, endocrine therapy.
Of note, previous clinical studies attempting to combine CDK4/6 inhibitors with ICIs in this patient population were terminated prematurely owing to safety concerns,6 or failed to provide definitive data in support of a beneficial therapeutic interaction.7 At least hypothetically, such a lack of cooperation might reflect the detrimental effects of CDK4/6 inhibitors on immune cells other than neutrophils,8 including cell types actively involved in anticancer immunosurveillance.9 Thus, it will be interesting to investigate whether the exquisite specificity of atirmociclib for CDK4 enables therapeutic cooperation with ICIs in patients with HR+HER2− breast cancer.
Finally, while Palmer and colleagues reported various potential mechanisms of resistance to atirmociclib that overlap with molecular pathways limiting the activity of CDK4/6 inhibitors, e.g., CDK2 activation,3 it will be important to investigate whether immunosuppressive cells that have been linked with poor sensitivity to CDK4/6 inhibition in preclinical models of HR+HER2− breast cancer, notably γδ cells, are also at play.10
Despite this and other unknowns, selective CDK4 inhibition with atirmociclib stands out as a promising strategy to improve disease outcomes in patients with HR+HER2− breast cancer. The results of the FourLight-3 study are urgently awaited to formally address this possibility.
Comments (0)