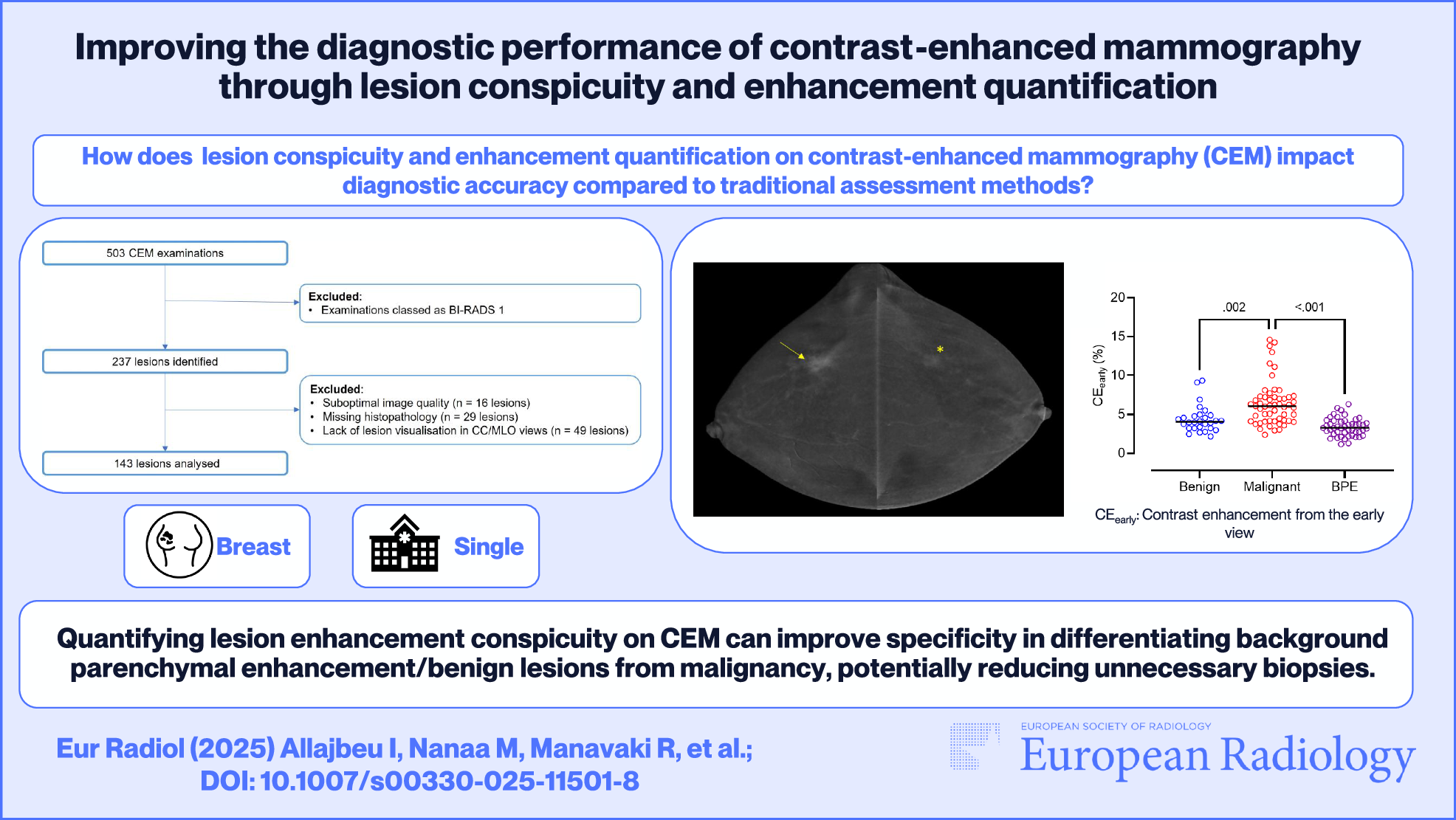
This retrospective analysis of selected lesions from screening and symptomatic CEM research studies suggests that quantifying lesion enhancement using contrast can enhance CEM specificity and overall diagnostic performance in differentiating benign lesions or BPE from malignancy. Lesion contrast from the early recombined view outperformed other metrics in differentiating malignancy from benign lesions or BPE, with AUC values of 0.83 and 0.88, respectively, and a specificity of 90% when discriminating malignant lesions from BPE.
CEM is an emerging contrast-enhanced imaging technique, with high diagnostic sensitivity but relatively low specificity [22]. Its growing utilization in diagnostic and screening settings necessitates additional methods to improve specificity and reduce unnecessary recalls [23]. Previous studies have investigated qualitative and quantitative lesion enhancement on CEM for predicting malignancy with variable results [13, 14, 24,25,26]. To our knowledge, this is the first comprehensive study analyzing conspicuity in relation to quantitative metrics of lesion enhancement on CEM recombined images and comparing their diagnostic performance.
Conspicuity is a novel descriptor introduced in the recent BI-RADS CEM lexicon that could potentially enhance lesion characterization. Recent studies suggest that lesion conspicuity on CEM demonstrates satisfactory diagnostic performance in predicting malignancy, with high conspicuity significantly correlating with ER/PR-negative or grade 3 cancers [19], while the low conspicuity of benign lesions on CEM has been found to potentially help reduce false positives in clinical practice [27]. Similarly, our study revealed a significant correlation between conspicuity and lesion histology, with most low-conspicuous lesions being normal/benign, and malignant lesions showing predominantly high conspicuity. Although the limited number of cancers in our study may explain the lack of a significant association between conspicuity and tumor histopathology, our results are broadly consistent with those of previous studies [19, 28], which also reported non-significant associations between conspicuity and cancer histopathology, along with a significant positive correlation between conspicuity and cancer grade [19].
Conspicuity assessment showed strong interobserver agreement (W = 0.87), with full consensus for B3 and non-enhancing lesions. However, reader agreement was lower for BPE (W = 0.55) than benign (W = 0.87) or malignant lesions (W = 0.88). The moderate inter-reader agreement regarding BPE conspicuity likely arises from differing perceptions of mild and moderate BPE among readers, consistent with observations from a previous study on BPE classification on CEM [29].
We observed a significant correlation between lesion histology and contrast enhancement from both the early and late recombined views. Despite methodological differences in the quantitative assessment of CEM enhancement between published studies, our findings align with those of previous reports [6, 13, 14, 24, 30], showing significantly higher signal enhancement in malignant than benign lesions. The contrast from the early recombined view (CEearly) allowed better differentiation between benign and malignant lesions, indicating that lesion enhancement measured within 3 min after contrast administration can provide important information about malignancy. However, unlike Liu et al [13], quantitative metrics or CEM enhancement type were not significantly associated with tumor histopathology. This may be attributed to the limited number of cancers in our study, mostly hormone receptor-positive ductal carcinomas.
Lesion histology was significantly associated with CEM enhancement pattern, with normal/benign lesions exhibiting progressive enhancement, while cancers predominantly followed plateau or wash-out patterns. This observation is in agreement with Deng et al [14], who reported an association between decreasing enhancement patterns on CEM and malignancy and is consistent with DCE-MRI results, where wash-out enhancement typically indicates malignancy [31, 32].
Consistent with Liu et al [13], we found non-significant differences in quantitative metrics between invasive and non-invasive cancers, with 56% of non-invasive cancers showing progressive enhancement. However, there is conflicting literature regarding the differentiation between invasive and non-invasive diseases using CEM. Rudnicki et al [24] found significant differences in quantitative metrics between invasive and in situ carcinoma, while Liu et al [13] noted differences in enhancement intensity between benign and in situ disease, but not between non-invasive and infiltrating cancers. Our findings mirror observations from contrast-enhanced MRI, where approximately half of the non-invasive lesions exhibit persistent enhancement [33, 34].
Despite insufficient data on the diagnostic performance of CEM, previous studies indicate high sensitivity and moderate specificity that is comparable to MRI [35, 36]. In our study, CEearly showed superior performance in differentiating normal/benign from malignant lesions (AUC = 0.83) than other metrics, in agreement with reported AUC values (0.70–0.88) in previous studies [13, 19, 24, 25]. Furthermore, we could differentiate between BPE and cancers with a specificity of 90%. Our results broadly agree with those of Boca et al, who used CEM-based radiomics to differentiate BPE from malignancy [37].
In a subgroup of 66 lesions, the agreement between DCE-MRI and CEM enhancement types was fair-moderate (Cohen’s κ = 0.35), which is lower than the value reported in Liu et al (Cohen’s κ = 0.52) [13]. This difference was possibly related to the smaller sample size (n = 28) investigated with MRI in the latter study, which included only symptomatic cases. Interestingly, we observed higher agreement between CEM and DCE-MRI enhancement patterns for lesions exhibiting wash-out enhancement (Cohen’s κ = 0.5) than those with progressive (Cohen’s κ = 0.30) or plateau enhancement (Cohen’s κ = 0.31).
Similar to a previous study [13], we utilized the maximum value within the lesion for contrast enhancement calculations rather than the average, as the former is independent of region placement, lesion shape, and size, thereby providing a consistent and reproducible approach for lesion enhancement quantification. Furthermore, the maximum value better represents peak contrast in heterogeneous lesions, although it is more susceptible to noise. While the average would better reflect overall lesion intensity, it is also more significantly affected by partial volume effects and region-boundary inconsistencies.
Our study has several limitations. First, it is a single-center retrospective study with a limited number of cancers and benign lesions. Second, the lack of standardization in contrast injection times and dose are known limitations of CEM that might affect the quantification of enhancement intensity and patterns [38, 39]. Third, our investigation focused exclusively on assessing lesion enhancement on recombined images, without taking into consideration features such as shape, margins, calcifications, or distortion in low-energy images. Given the significant role of low-energy images in the evaluation of CEM in clinical practice, combining features from low-energy mammograms with the degree of enhancement, along with consensus reading for discordant cases, could lead to more accurate results [40]. Fourth, approximately 40% of lesions were excluded at initial screening due to issues such as the lack of lesion visualization on CC and MLO views, suboptimal image quality, or missing histopathology. While these exclusions may have affected the representativeness of our lesion sample, applying these exclusion criteria was necessary to maintain the accuracy and reliability of our results. Lastly, the retrospective nature of our investigation prevented us from evaluating the effect of differences in lesion configuration between CC and MLO views on contrast measurements and RSD at individual time points. However, a previous study found non-significant differences in signal enhancement and contrast between the two views [22]. Additionally, our methodology for contrast determination was comparable between the two views.
In conclusion, our results indicate that quantifying lesion enhancement conspicuity and patterns can improve CEM specificity and diagnostic performance in differentiating BPE or benign lesions from malignancy, potentially reducing unnecessary recalls and benign biopsies. Incorporating lesion conspicuity into routine CEM reporting could enhance lesion evaluation and diagnostic accuracy. Standardization of CEM protocols combined with AI-assisted tools for prompt lesion delineation and enhancement quantification may boost robustness and streamline clinical implementation [41]. Large multicenter studies are needed to establish reliable conspicuity thresholds and validate their integration with AI tools to optimize clinical workflows.

Comments (0)