
Remember me



In September 2023, the initiative commenced, culminating in an inaugural video conference on the 14th of that month. An initial cohort of 90 experts in laser proctology was solicited, from which 60 specialists worldwide expressed interest. Ultimately, 48 of these experts actively contributed throughout the project, forming the core of the Recommendation Development Group (RDG). The composition and credentials of the RDG are summarized in Table 1
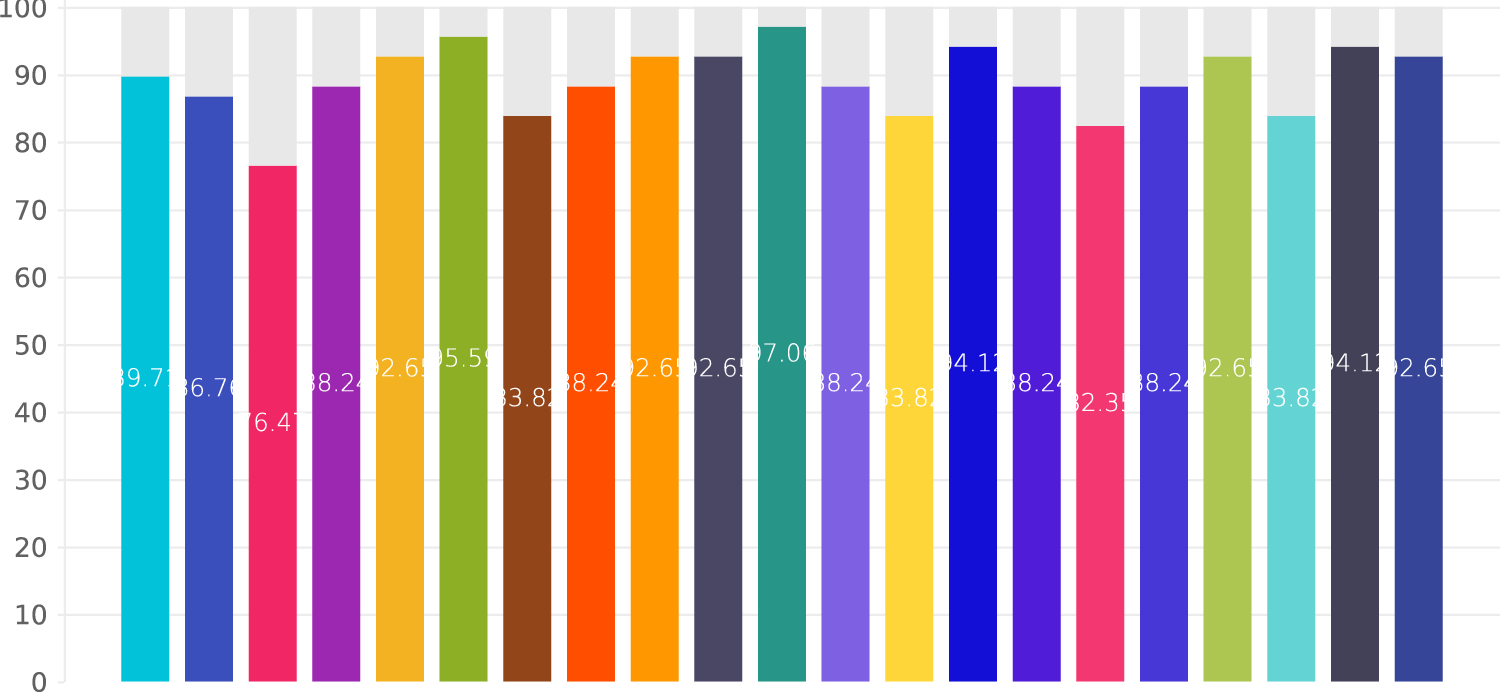
Table 1 Summary of the origins of the members of the RDGFrom the wealth of current literature and their collective expertise, the RDG formulated 21 deliberative questions (Qs) pertaining to LHP. These questions, accompanied by expert commentary, yielded 21 corresponding responses (Rs) or Delphi statements. When put to a vote among the 48 RDG panelists, all statements achieved over 75% consensus in the initial Delphi round, thereby concluding the voting process. Of these, 16 statements reached a strong consensus, defined by an agreement exceeding 85%, and the remaining five achieved consensus. The results of Delphi voting are depicted in Fig. 1.
Fig. 1
Results of the Delphi process for the 21 Qs and Rs
What are the main indications for LHP?
Five randomized controlled trials (RCTs) have investigated LHP vs. excision for the treatment of symptomatic grade 2 and 3 hemorrhoids. A double-blinded RCT by Naderan et al. [21] from 2016 investigated LHP vs. hemorrhoidectomy in 60 patients with symptomatic grade 2 and 3 hemorrhoids in a 1:1 design. Another double-blinded RCT by Poskus et al. [22] from Vilnius investigated LHP vs. mucopexy vs. hemorrhoidectomy using a 1:1:1 design including 120 patients with symptomatic grade 2 and 3 hemorrhoids. Shabahang et al. [23], Lim et al. [24], and Cemil et al. [25] also included only patients with grade 2 and 3 hemorrhoids in their RCTs. Moreover, grade 2 and 3 hemorrhoids were the most common indications for LHP in published systematic reviews [26,27,28,29]. In the systematic review by Lakmal et al. [26] published in 2021 including 1937 patients from 19 studies, LHP was performed for grade 2 and 3 hemorrhoids. Similarly, grade 2 and 3 hemorrhoids represented the indications for surgery in a large majority of the studies included in the systematic review by Longchamp et al. [28]. A similar spectrum of indications was reported in the systematic reviews by Lie et al. [27] and by Wee et al. [29].
R1:Symptomatic grade 2 and 3 hemorrhoids represent the standard indications for LHP as a single intervention (without additional procedures like HAL or mucopexy).
Strong consensus: 89.71%
Should devascularizing techniques like hemorrhoidal artery ligation (HAL) be routinely used as an adjunct to LHP?
Although LHP alone represents a good procedure for symptomatic grade 2 and 3 hemorrhoids, it may be used in combination with other non-excisional techniques, especially mucopexy and/or devascularization of the hemorrhoidal tissues via ligation of the hemorrhoidal arteries. Hemorrhoidal dearterialization is generally performed via ligation of the hemorrhoidal artery as reported by Morinaga in 1995 [30] and aims at reducing blood flow into the hemorrhoidal plexus. Devascularization of the hemorrhoidal tissue during LHP may be performed with or without ultrasound guidance. In an RCT from Iran by Shabahang et al. the outcomes of LHP vs. hemorrhoidectomy were investigated in 80 patients in a 1:1 design. In that study, HAL and mucopexy were performed using a running 2-0 Vicryl in the LHP group [23]. In a recently published investigation from Austria, Jain et al. used ligation of the hemorrhoidal artery as well as mucopexy in addition to LHP in 30 patients with symptomatic grade 2–4 hemorrhoids [31].
Bleeding complications, e.g., postoperative hemorrhage, hematoma, and acute thrombosis, represent the most common short-term morbidities following LHP. The rate of postoperative bleeding following LHP has been reported at about 0–7.6% [32,33,34], while the incidence of acute thrombosis has been reported to be as high as 4–10% [35, 36]. The risk of postoperative bleeding following LHP with and without HAL was investigated in a recently published RCT by Lim et al. from Malaysia. The outcomes of 38 patients undergoing LHP alone were compared to those of 38 patients undergoing LHP followed by HAL using 2-0 Vicryl without Doppler guidance. Postoperative bleeding in this study was graded using a visual rating score where “0” corresponded to no bleeding, “1” indicated mild bleeding defined as minimal trickling or spotting, bleeding not requiring surgical intervention was graded as moderate “2”, while any bleeding with a drop in hemoglobin level and/or requiring surgical intervention was graded as severe “3” [24]. Irrespective of potential limitations regarding the rather subjective nature of the grading system used in that study, no significant difference was seen amongst both arms regarding the risk of postoperative bleeding. In contrast, the overall rate of postoperative hemorrhage (36.8% vs. 23.7%) was higher in the LHP-HAL group compared to the LHP group in that RCT. The findings from that RCT therefore suggest that there is little evidence for the routine use of HAL following LHP with the goal of reducing postoperative bleeding complications. However, the data reported in that RCT must be interpreted with caution due to possible bias in grading of postoperative hemorrhage. A crucial issue regarding the risk of postoperative bleeding complications following LHP with HAL seems to be the sequence of events. In both RCTs by Shabahang et al. and Lim et al., HAL was performed after LHP [23, 24]. A reversed sequence, starting with HAL prior to LHP, was chosen by Jain et al., who reported just one case of mild postoperative bleeding and acute thrombosis each in the LHP group with 30 patients [31]. The findings reported by Jain et al. are largely in accordance with the experience of a large majority of the experts in the RDG.
The techniques discussed above should not be confused with the Doppler-guided technique of hemorrhoidal devascularization (HeLP) using laser energy [37, 38]. Proponents of this technique see advantages in the minimally invasive means of addressing the terminal hemorrhoidal arteries without the need for sutures. Another aspect of this technique is the possibility of managing all the terminal branches of the superior hemorrhoidal artery. This procedure, however, is totally different from the standard LHP and therefore is out of the scope of this project.
R2:HAL with or without ultrasound guidance can be performed in combination with LHP for grade 2/3 hemorrhoids, beginning with HAL prior to LHP.
Strong consensus: 86.76%
What is the role of LHP in the management of grade 4 hemorrhoids?
The management of grade 4 hemorrhoids with LHP has been reported in the current literature in a rather small number of cases. Patients with grade 4 hemorrhoids represented 23% of the LHP group in the study by Jain et al. [31]. Patients with grade 4 hemorrhoids constituted 38% and 46% of the study population in two prospective investigations by Mert [39] and Khan et al. [36], respectively. The available literature thus seems to support the use of LHP in selected patients with grade 4 hemorrhoids.
Because addressing the prolapse represents a relevant outcome from the patient’s perspective, the RDG recommends combining LHP with HAL and mucopexy. This technique was used in a German cohort by Weyand et al. to manage grade 4 and prolapsed hemorrhoids [40]. A short segment mucopexy was needed in 253 of the 499 patients included in their study. The findings from that study suggest that the management of grade 4 hemorrhoids using LHP in combination with mucopexy is feasible. However, there seems to be some increase in the risk of morbidity, especially in this cohort.
According to expert opinion, LHP can be used with additive techniques like HAL and/or mucopexy to manage grade 4 hemorrhoids by experienced surgeons, especially after conservative management of an acute prolapse. The patient must be informed not only about the increased risk of morbidity and recurrence but also about the increased risk of pain associated with the use of additional techniques besides LHP.
R3:Grade 4 hemorrhoids can be managed via a combination of LHP, HAL, and/ or mucopexy based on surgeon’s expertise and patient’s expectation.
Consensus: 76.47%
How many piles can be managed at the same time?
While the indication for LHP is largely stated in most of the available publications, the number of piles managed was reported in very few articles. In the article by Weyand et al. two and three segments (piles) were managed in 1/3 and 2/3 of their study population, respectively [40]. Mert on the other hand reported treatment of just one quadrant in 28%, two quadrants in 28%, three quadrants in 20%, and four quadrants in 4% of her study population [39], while a median of three piles (range 1–6) were treated in the study by Faes et al. [33]. In the latter study, one case of continence disturbance was reported following LHP [33]. This rather uncommon complication after LHP may be secondary to shrinkage of many piles following extensive LHP treatment (multiple piles) in a patient with preoperatively suboptimal continence. The wide heterogeneity in the number of piles treated in published studies renders specification impossible. There is a strong consensus amongst members of the RDG to address only pathologic piles to prevent overtreatment.
R4:Only pathologic hemorrhoids should be treated.
Strong consensus: 88.24%
Q5.Can external hemorrhoids and skin tags be managed at the same time with LHP?
Skin tags were removed in 28% of the German cohort by Weyand et al. [40]. Similarly, skin tags were excised in 53.3% of cases in the study by Jain et al. [31] and in 40% of cases in the Swiss study by Faes et al. [33]. While this practice appears to be in accordance with patient expectation, there is no evidence in the current literature to recommend the management of external hemorrhoids and skin tags as part of the standard LHP procedure. The RDG cautions toward the use of the laser for the shrinkage of external hemorrhoids because of a hypothetical risk of fistula formation. Moreover, additional procedures may increase the risk of complication and postoperative pain.
R5:Management of external hemorrhoids and skin tags may be considered in individual cases (patient’s expectation) but should not represent an elementary aspect of the standard LHP procedure.
Strong consensus: 92.65%
Can LHP be routinely combined with other proctological procedures?
There is hardly any data in the current literature looking into the combination of LHP with other procedures. In the retrospective study by Weyand et al. four fistulectomies, seven polypectomies, and 21 fissurectomies were performed during LHP [40]. As stated above (comments to Q5), the most relevant advantage of LHP, i.e., less pain, may be jeopardized by additional procedures around the anoderm. Also, the theoretical risk of morbidity increases with additional procedures. Nonetheless, addressing other pathologies at the same time with LHP may be reasonable in some cases. The coexistence of both symptomatic piles and a chronic anal fissure in a patient presenting with pain, for example, warrants a simultaneous management of both pathologies. Similarly, polypectomy can be safely performed during LHP. The decision for additional procedures during LHP may be reached in individual cases as a shared decision between surgeon and patient after considering the patient’s expectations and surgeon’s expertise.
R6:Additional proctological procedures can be combined with LHP in individual cases but cannot be considered as routine.
Strong consensus: 95.59%
What are common contraindications for LHP?
So far, contraindications for LHP have not been widely reported in the literature. However, active inflammatory processes like abscesses, proctitis, and undrained fistula may increase the risk of complication following LHP [41]. Therefore, surgery should be rescheduled in such cases. Uncontrollable hemorrhagic conditions with high risk of bleed may constitute relative contraindications.
R7:Acute inflammation such as abscess, proctitis, and fistula represent absolute contraindications for LHP.
Consensus: 83.82%
What is the role of LHP in managing recurrent hemorrhoids?
The risk of recurrence may be seen as the Achilles tendon of LHP. In an RCT by Naderan et al. investigating LHP vs. hemorrhoidectomy for grade 2 and 3 symptomatic hemorrhoids, the rate of recurrence was 6.7% vs. 10% after 12 months for the LHP vs. hemorrhoidectomy, respectively [21]. In a retrospective study by Gambardella et al., the rates of recurrence following LHP were 1.3% after 6 months, 9.4% after 12 months, and 21.6% after 24 months [42]. In another retrospective study by Ram et al. from Israel 10.5% of the cohort of 162 patients undergoing LHP had undergone previous intervention for hemorrhoids [43]. In a recently published paper by Dursun et al., the risk of recurrence was 50% in 12 patients with grade 4 hemorrhoids compared to 17.6% in 91 patients with grade 2 and 3 hemorrhoids [41]. While the small number of cases undergoing LHP for grade 4 hemorrhoids in this study appears to be in line with the current literature, the high rate of recurrence for this group may be easily explained via the sample size. Moreover, it was not stated whether mucopexy was added to LHP for patients with grade 4 hemorrhoids in this study. Nonetheless, these results argue for a grade-dependent risk of recurrence. In the study be Faes et al., 49 of 50 patients treated with LHP reported that they would recommend LHP to other patients and relatives. After 5-years follow-up, 64% would still recommend LHP [33]. Because LHP is an organ-preserving procedure, the risk of recurrence would most probably remain an issue that needs to be discussed with the patient. The expert opinion is that LHP could still be a good option following recurrence.
R8:LHP could still be a good option following recurrence and should be discussed with the patient on an individual basis.
Strong consensus: 88.24%
What is the optimal bowel preparation prior to LHP?
There is a high degree of heterogeneity on bowel prepping prior to LHP in the literature. An enema given prior to surgery has been reported in many studies and seems to represent the most favored method of bowel prepping in this setting [39, 44, 45]. In an RCT from Vilnius by Poskus et al., lactulose was given 1 day prior to LHP for bowel prepping [22]. So far, there is no standardized technique for bowel prepping prior to LHP. The timing of bowel prepping should be well chosen, e.g., enema 2 h prior to LHP [39, 46, 47] or the day before surgery [22]. The rationale behind this timing is to reduce the risk of spillage of feces during and immediately after LHP as a means of reducing the risk of infection of the punction sites. For patients needing colonoscopy prior to surgery, LHP can be performed after colonoscopy without further prepping. Expert opinion is to omit bowel prepping for standard LHP or use an enema 2 h prior to surgery for more extensive procedures requiring HAL or mucopexy in combination with LHP.
R9:Bowel prepping may be omitted prior to standard LHP.
If needed, a simple enema may be given about 2 h prior to surgery.
Strong consensus: 92.65%
Q10.What is the role of perioperative antibiotic prophylaxis for LHP?
The need for single-shot antibiotic prophylaxis specifically for LHP has not been systematically investigated. Therefore, the published data largely represents institutional standards rather than following established protocols. Despite this limitation, most published papers reporting on perioperative antibiotics used a combination of a second- or third-generation cephalosporine and metronidazole [21, 22, 24, 42]. The use of a single antibiotic for this purpose has also been reported in recent literature, e.g., Brusciano et al. used 2 g ceftriaxone i.v. [32], while the Canteralla et al. used 1.2 g of Augmentin as prophylactic antibiotic [48]. Interestingly, perioperative antibiotic prophylaxis was either not given or not reported in a huge proportion of available papers on LHP. Therefore, there is no solid data to back the routine use of prophylactic antibiotics in patients undergoing LHP. The indication for prophylactic antibiotics therefore should be made on an individual basis.
R10:Routine single-shot antibiotics can be omitted during LHP. Antibiotic prophylaxis should be considered in individual cases on the basis of patient’s risk factors.
Strong consensus: 92.65%
Q11.What is the optimal wavelength for LHP?
Two wavelengths, 980 nm and 1470 nm, have been widely used to deliver the laser energy within the pile to induce shrinkage of the hemorrhoidal tissue [49,50,51]. High-quality evidence on the efficacy of the 980-nm wavelength is available from RCTs, mainly from the Asian Pacific region [21, 24, 35, 44]. Equally, high-quality evidence for the 1470-nm wavelength is available from published RCTs and prospective studies [22, 23, 32, 34, 36]. So far, there is no comparative study investigating both wavelengths for this indication.
R11:Both 980 nm and 1470 nm wavelengths can be safely used for LHP.
Strong consensus: 97.06%
Q12.What is the optimal laser setting with regards to laser power in watts for LHP?
While the optimal wavelengths for LHP are clear, the only other undisputable technical aspect about the setting of the laser applicator is the pulse mode of energy application. Wide heterogeneity can be seen in the duration of application (pulse duration) and the amount of energy per pulse. In a retrospective investigation from Iran by Jahanshani et al., a pulse mode of 3 s duration with a power of 15 W was the reported setting using the 980-nm wavelength [52]. A similar setting was chosen by Naderan et al. in their RCT, but for the fact that the pulse duration was set at 1.2 s [21]. The same wavelength and the pulse mode with 13 W for 1.2 s was the preferred setting for Mert [39]. The wide spectrum of possible laser generator settings is further demonstrated in the report by Mohammed et al. using 5 W for 3 s in the pulse mode [53].
A similar scenario is easily identified for the 1470-nm wavelength. Gambardella et al., for example, used the pulse mode with 8 W for 3 s in their retrospective cohort [42]. This setting was used in the RCT by Poskus et al. [22] as well as in the observational study from the Netherlands by Boerhave et al. [54]. In a Turkish prospective investigation, the pulse mode was set at 10 W for 5 s [55]. Lower [56] and higher [31] performance/energy settings have been reported for the 1470-nm wavelength in the current literature (Table 2).
Table 2 Recommended laser settings R12:For laser machines employing 980 nm wavelength, a setting of 12–15 W per pulse (1.2 s) can be recommended.
For laser machines employing 1470 nm wavelength, a setting of
Comments (0)