
Remember me
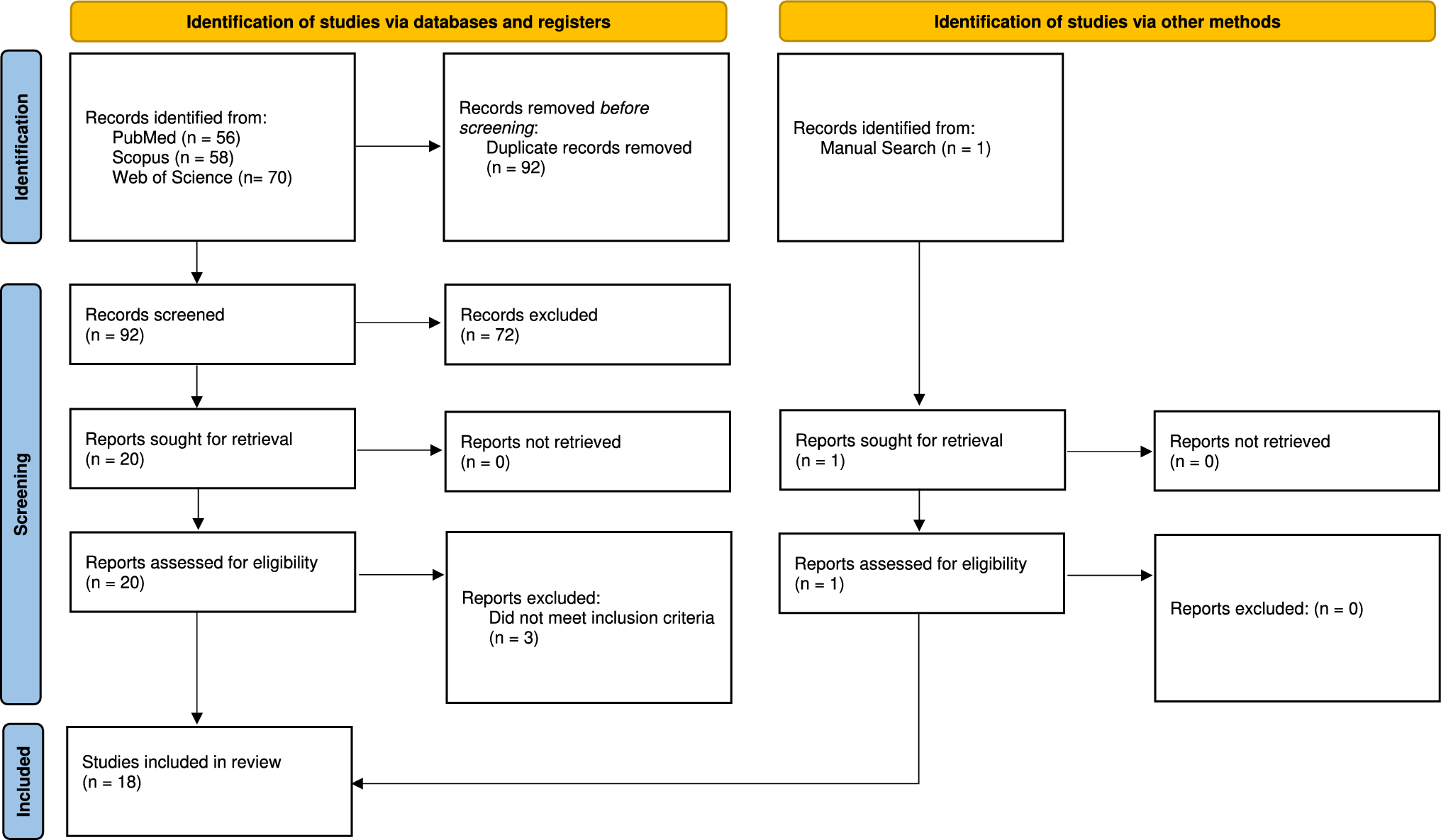
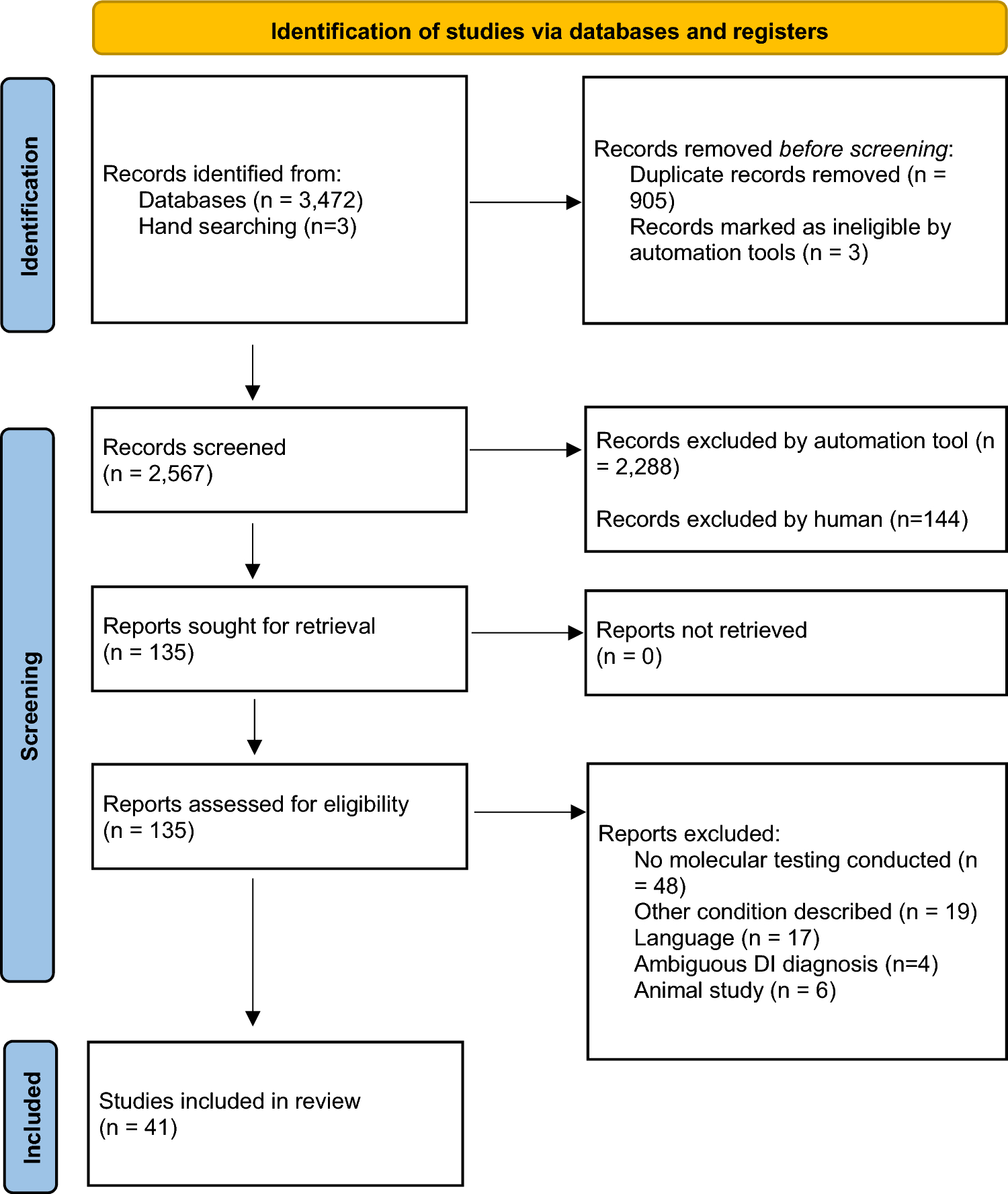
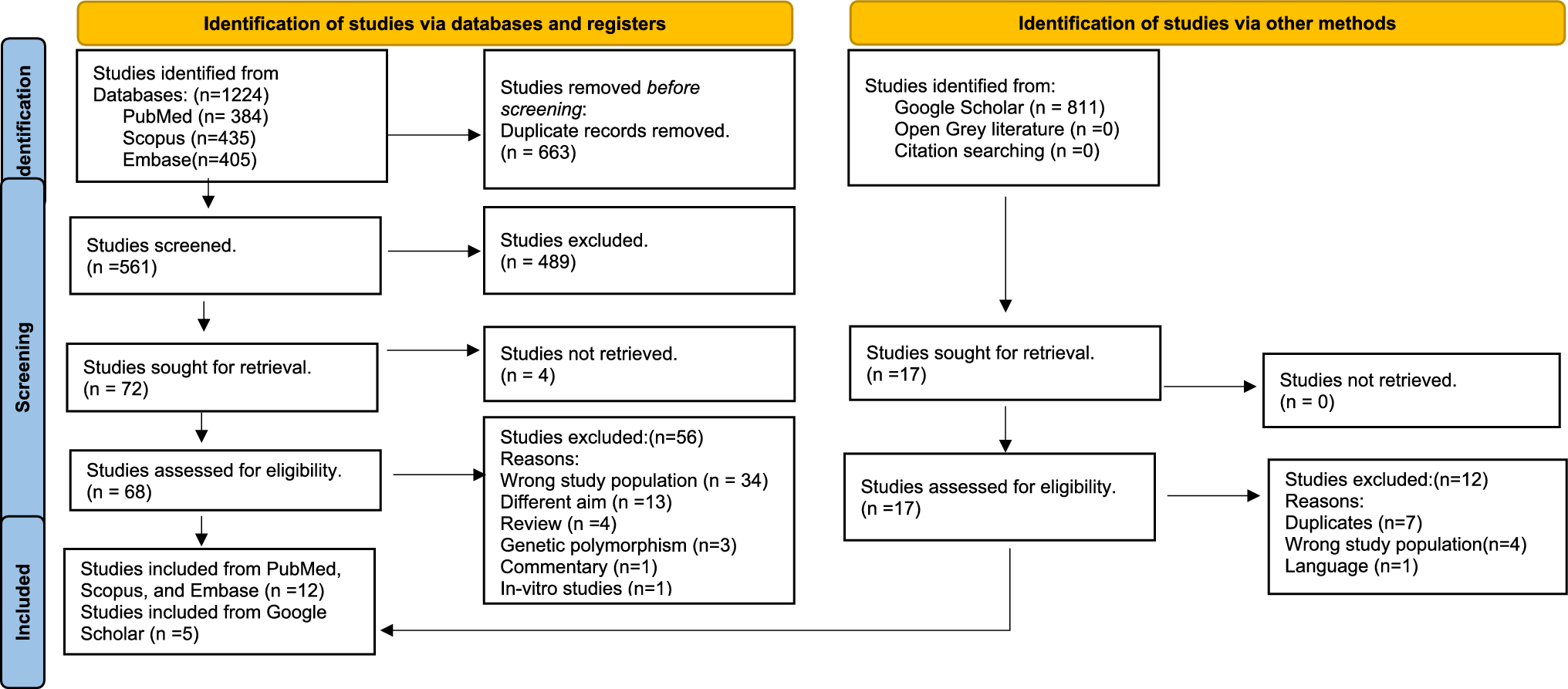

A total of 1,224 studies were initially retrieved from the three electronic databases. These were reduced to 561 after removal of 663 duplicates. Following a double title/abstract screening of 561 studies, 489 articles were excluded due to non-conformity with the eligibility criteria. The remaining 72 records were identified for full-text screening. Full texts of four articles could not be retrieved. Through a meticulous full-text screening process, a total of 68 studies were assessed. Subsequently, 56 articles were excluded due to their failure to meet the eligibility criteria. The reasons for exclusion are provided in the supplementary file (Table IV). Finally, 12 studies were identified for inclusion from PubMed, Scopus and Embase. A parallel search on Google Scholar identified 811 studies of which 17 were assessed for eligibility. Following exclusion of 12 studies, 5 were found to be eligible for inclusion in the review after full-text screening. Combined search, screening, and selection process of studies from PubMed, Scopus, Embase, and Google Scholar identified 17 primary studies for inclusion in the review as depicted in the PRISMA Flow chart (Fig. 1). No additional records were retrieved from open gray literature.
Fig. 1
PRISMA flow diagram of the processes leading to 17 studies included for review (Page et al. 2021)
Primary characteristics of individual studiesOf the 17 primary studies included in this systematic review, 14 studies (82.35%) employed an analytical cross-sectional study design. Other study designs included 2 case–control studies (11.76%) and one prospective cohort study (5.88%). The included studies were published between 2011 and 2022. The main characteristics of the included studies in the qualitative synthesis are summarized in Table 1. A total of 1,330 subjects were recruited of which 537 were males, and 559 were females. Five studies did not report male-to-female distribution (Damle and Doifode 2011; Ranadheer et al. 2011; Priya et al. 2013; Picco et al. 2017; Vasudevan et al. 2022). Most studies were conducted in India (n = 6) (Damle and Doifode 2011; Ranadheer et al. 2011; Priya et al. 2013; Pyati et al. 2018; Ahmad et al. 2021; Vasudevan et al. 2022), followed by China (n = 3) (Yang et al. 2015; Wang et al. 2018; Chen et al. 2020), Brazil (n = 1) (Picco et al. 2017), Colombia (n = 1) (Angarita-Díaz et al. 2021), Egypt (n = 1) (WM and Youssef 2016), Indonesia (n = 1) (Soesilawati et al. 2019) Romania (n = 1) (Monea, Vlad and Stoica 2018), Saudi Arabia (n = 1) (Murugeshappa et al. 2018), Serbia (n = 1) (Stojković et al. 2020), and Thailand (n = 1) (Angwaravong et al. 2015).
Table 1 Primary characteristics of the included studiesThe included studies investigated a variety of salivary proteins for their potential association with dental caries in children during mixed dentition (6–13 years). Most of the studies used DMFT/deft caries index (n = 13) (Damle and Doifode 2011; Ranadheer et al. 2011; Priya et al. 2013; Yang et al. 2015; Picco et al. 2017; Murugeshappa et al. 2018; Pyati et al. 2018; Wang et al. 2018; Soesilawati et al. 2019; Chen et al. 2020; Stojković et al. 2020; Ahmad et al. 2021; Vasudevan et al. 2022), except for 3 studies that employed the ICDAS (n = 1)(Angarita-Díaz et al. 2021), visual detection method (n = 1) (Monea, Vlad and Stoica 2018), and modified WHO diagnostic criteria (n = 1) (Angwaravong et al. 2015). Although most studies used DMFT/deft caries index, the cut-off values of caries-free/caries-prone patients varied among studies. There were 612 individuals with dental caries and 505 subjects in the control group across all the studies. Five studies considered (DMFT/deft ≥ 5) as caries-active group (Priya et al. 2013; Murugeshappa et al. 2018; Pyati et al. 2018; Ahmad et al. 2021; Vasudevan et al. 2022), two studies considered (DMFT/deft ≥ 3) as caries-active group (Ranadheer et al. 2011; Soesilawati et al. 2019), one study considered (dmfs > 8) as caries-active group (Chen et al. 2020), whereas one study considered (dfs ≥ 10) as caries-active group (Damle and Doifode 2011). Two studies considered (DMFT/dmft = 5–10 & 5–15) as high dental caries group, and (DMFT/dmft = 1–4) as low dental caries group (Yang et al. 2015; Wang et al. 2018), while two studies did not report the DMFT/deft scores (WM and Youssef 2016; Picco et al. 2017). On the other hand, studies considered DMFT /or deft = 0 as caries-free group (n = 12) (Damle and Doifode 2011; Ranadheer et al. 2011; Priya et al. 2013; Angwaravong et al. 2015; Yang et al. 2015; Murugeshappa et al. 2018; Pyati et al. 2018; Wang et al. 2018; Chen et al. 2020; Stojković et al. 2020; Ahmad et al. 2021; Vasudevan et al. 2022). Only one study considered deft < 3 as low-caries group (Soesilawati et al. 2019).
All included studies collected unstimulated saliva, except for three studies that evaluated stimulated saliva (Picco et al. 2017; Soesilawati et al. 2019; Vasudevan et al. 2022). Most studies performed saliva collection in the morning; however, six studies did not report at what time of day the saliva sample collections were carried out (Damle and Doifode 2011; Ranadheer et al. 2011; Priya et al. 2013; WM and Youssef 2016; Picco et al. 2017; Murugeshappa et al. 2018). Of the 17 studies, only two studies evaluated differentially expressed salivary proteins between caries-free and caries affected individuals (Wang et al. 2018; Chen et al. 2020) while the remaining 15 studies compared salivary levels of specific proteins among caries-free and caries-active groups.
In regard to the methods for protein analysis, enzyme-linked immunosorbent assay (ELISA) was used for quantification of salivary proteins in most studies (Ranadheer et al. 2011; Priya et al. 2013; Angwaravong et al. 2015; Yang et al. 2015; WM and Youssef 2016; Picco et al. 2017; Murugeshappa et al. 2018; Soesilawati et al. 2019; Stojković et al. 2020; Angarita-Díaz et al. 2021; Vasudevan et al. 2022). Total protein content of saliva was investigated by Biuret method (WM and Youssef 2016; Pyati et al. 2018), and Bradford analysis (Murugeshappa et al. 2018; Chen et al. 2020). Other methods used were spectrophotometer (Monea, Vlad and Stoica 2018), radial immunodiffusion (Damle and Doifode 2011), and two-site sandwich enzyme immunoassay (Ahmad et al. 2021). Two studies carried out a comprehensive analysis of salivary proteome with a focus on evaluating differentially expressed proteins reported in caries-free and caries-active children (Wang et al. 2018; Chen et al. 2020) Chen et al (2020) used SDS-PAGE electrophoresis, and iTRAQ-coupled LC–MS/MS for salivary protein quantification (Chen et al. 2020), while Wang et al (2018) also used iTRAQ-based mass spectrometry for quantitative proteomic analysis (Wang et al. 2018).
Association between salivary proteins and dental cariesThe findings of the included studies based on differences in salivary protein levels between caries-active and caries-free groups are depicted in Table 2. The key findings related to different salivary proteins are summarized below.
Table 2 Association of salivary proteins with dental caries in children with mixed dentition in the included studiesTotal protein contentThe association of total protein content with dental caries was investigated by four studies. The total protein content was reported to be positively associated with caries in three studies (Murugeshappa et al. 2018; Pyati et al. 2018; Vasudevan et al. 2022). However, the differences in total salivary protein content between caries-active and caries-free groups were not statistically significant in one study (Vasudevan et al. 2022). One study reported that the total protein content was similar between the two groups (WM and Youssef 2016).
Salivary glycoproteinsSalivary immunoglobulin A (IgA) was the most commonly investigated glycoprotein in the included studies (n = 7). The mean salivary IgA levels were reported to be higher in caries-free group which attributed to their protective role against dental caries (Damle and Doifode 2011; Murugeshappa et al. 2018; Ahmad et al. 2021; Angarita-Díaz et al. 2021). Similarly, salivary IgA levels were reported to be higher in subjects with low-caries activity (Soesilawati et al. 2019). However, salivary IgA levels were observed to be higher in caries-active group in two studies (Ranadheer et al. 2011; Priya et al. 2013).
Increased levels of MUC5B in subjects with low-caries activity and a negative correlation were shown between MUC5B and the number of decayed tee
Comments (0)