PCOS and Cardiovascular Event
Many previous studies of the effects of PCOS have not shown an increased risk of MACE in women with PCOS. In a nearly 5-year study by Morgan et al., women with PCOS did not have an increased risk of macrovascular disease or death, but were found to be at increased risk of type 2 diabetes [13]. Pierpoint et al. examined a cohort of 786 women diagnosed with PCOS followed for an average of 30 years for increased cardiovascular mortality [14]. Analysis of the calculated standardized mortality ratios (SMRs) showed that women with PCOS did not have a significantly higher than average cardiovascular mortality, although PCOS was strongly associated with diabetes, lipid disorders, and other cardiovascular risk factors. Another study comparing both cardiovascular morbidity and mortality in PCOS with the healthy population is the retrospective cohort study by Wild et al. [15]. The study used morbidity data from 319 women with PCOS and 1060 age-matched control women. Cohort all-cause and cardiovascular mortality was similar to the women in the general population. However, certain cardiovascular risk factors, including diabetes, hypertension, hypercholesterolemia, hypertriglyceridemia and increased waist:hip ratio (WHR), were higher in women with PCOS.
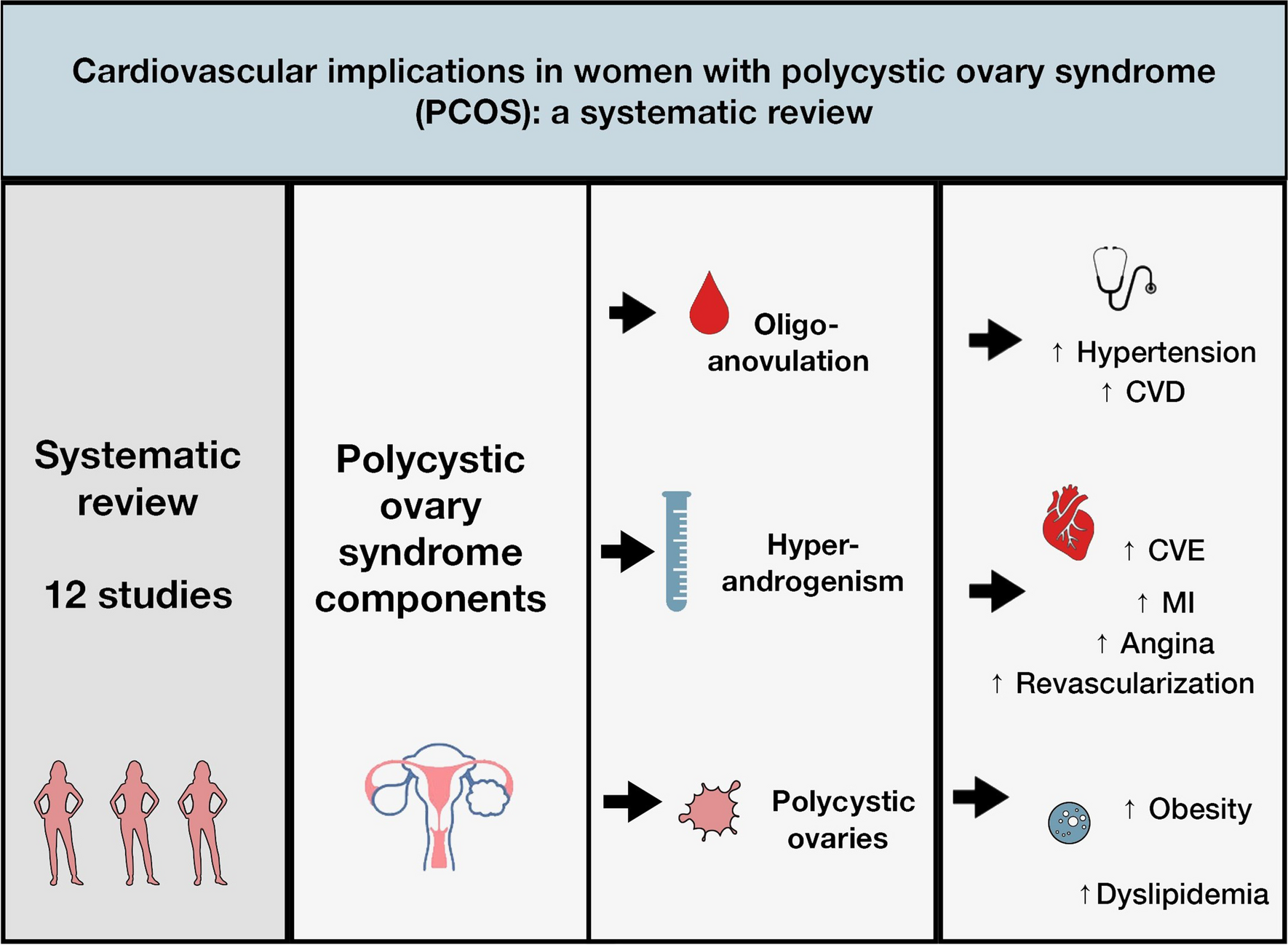
A recent retrospective study by Berni et al. compared the risk of MACE in women with PCOS with controls [16]. A total of 174,660 eligible women with PCOS were selected from the UK Clinical Practice Research Datalink Aurum and matched to controls by age, body mass index (BMI) and primary care practice. The average follow-up was 3.83 years for women with PCOS versus 3 years for the control group. The results demonstrated a grater risk of CVE in women with PCOS compared with no-PCOS woman. In this study young women with PCOS experienced higher risk of CVE, regardless of whether they were analyzed as a combined outcome or as separate outcomes of MI, angina, and revascularization. As this is the largest study to confirm an increased rate of CVD in young women with PCOS, authors highlight the crucial role of identifying PCOS as a higher-risk vascular disorder.
In some other prospective, population-based cohort study Ollila and colleagues evidenced a crucial elevated risk of CVE in the PCOS group [17]. The study cohort included 386 women diagnosed with PCOS according to the Rotterdam criteria and 144 women diagnosed according to the National Institute of Health (NIH) criteria, who were compared with the control group at the age of 31 years [5]. During the 22-year follow-up period, an increased incidence of CVE was observed in women in both PCOS classification groups, regardless of the diagnostic criteria used. The cumulative hazard curves in both PCOS diagnostic categories started to deviate from controls from the age of 35. Compared to controls, MI was significantly more frequent in both PCOS groups. The early increase in risk of CVE supports the need for early screening and controlling of CVD risk factors in patients with PCOS.
PCOS and Cardiovascular Risk Factors
Although obesity and hypertension are two known cardiovascular risk factors associated with PCOS, it is not entirely clear whether the risk of CVD in women with PCOS is solely led by traditional risk factors or occurs independently. There is evidence of significant associations between PCOS and CVD that are not related to obesity. Unlike other populations, East Asian women affected by PCOS typically have a low BMI and mild hirsutism. Using population-based data from the Korean National Health Insurance Service, Ryu et al. analyzed Korean women with PCOS aged 15–44 years and their matched controls to determine the association between PCOS and the incidence of CVD [18]. After reviewing data from a total of 549,534 registry participants, including 137,416 women with PCOS, the authors found that Korean women with PCOS had a higher risk of cardiocerebrovascular disease, regardless of their obesity. Followed for a median 4,5 years, the incidence rates of all CVD, ischaemic heart disease and cerebrovascular disease were statistically significantly higher in the PCOS group than in the control group. Even after adjusting for certain confounding variables such as BMI, diabetes, hypertension and dyslipidemia, the hazard ratio for composite CVD was higher in the PCOS group than in non-PCOS women. Women with PCOS had greater hazard ratios for ischaemic heart disease and cerebrovascular disease than controls. Due to the proven 1.3-times greater risk of developing CVD in women of reproductive age with PCOS compared to women without PCOS, independent of obesity, the authors emphasize the importance of implementing counseling on the long-term risk of CVD in all patients with PCOS in East Asian countries.
In a subsequent study, Joham et al. utilized data of 9508 women aged 21 to 42 years from the Australian Longitudinal Study on Women’s Health (ALSWH) to assess the occurrence of hypertension in women with and without PCOS over a 15-year follow-up period [19]. Hypertension was found to be significantly more common in young Australian women with PCOS than in women without PCOS, with the risk of hypertension being 37% higher in women with PCOS after adjustment for several variables including BMI, family history of hypertension, occupation and type 2 diabetes. When obese women with PCOS were compared with lean women with PCOS, the difference in the incidence rate of hypertension was 4 times greater in the obese subgroup. Knowledge of the increased risk of hypertension in women with PCOS regardless of BMI, which is aggravated further by obesity, indicates the need of screening these women from early adulthood for prevention, early detection and the possibility of treatment.
To better understand how PCOS and selected risk factors such as BMI, multiple pregnancy or gestational diabetes mellitus (GDM) influence the incidence of hypertensive disorders in pregnancy (HDP) in general, Khomami et al. conducted a study also based on data from the Australian Longitudinal Study of Women's Health (ALSWH) [20]. Of the 14,247 registry participants, 5838 women who reported both PCOS and HDP in at least one pregnancy were included in the study. Whereas the univariate model associated PCOS with a greater incidence of HDP, this significance disappeared when risk factors were adjusted. Nevertheless, PCOS lasted substantially associated with an increased risk of HDP only in non-obese women in the multivariate subgroup analysis. Furthermore, in contrast to previous literature, the study showed that PCOS predicted a lower risk of HDP in pregnancies with positive GDM. The authors emphasize the need for continued research, screening, and treatment of HDP among both PCOS and non-PCOS women with similar risk profiles.
PCOS, Inflammation and Cardiac Remodelling
The results of a cross-sectional study by Rashid et al. suggest a possible role of inflammation as a mediator in cardiac dysfunction in women with PCOS [21]. The authors quantified echocardiographic values of left ventricular mass (LVM) and left ventricular mass index (LVMI) and evaluated their correlation with measured markers of inflammation, insulin resistance (IR), and androgen levels by 260 women with PCOS diagnosed according to the Rotterdam criteria and 250 healthy women matched for age and BMI. In contrast to the control group, women with PCOS were characterised by a reduced number of menstrual cycles yearly and substantially greater Ferriman-Gallwey scores, plasma insulin, homeostasis model assessment of IR (HOMA-IR) [22], total testosterone, plasma glucose and inflammatory markers, such as high-sensitivity C-reactive protein in serum, tumor necrosis factor-α and interleukin-6. In normotensive, non-obese women with PCOS LVMI was greater than in healthy controls, which was positively associated with proinflammatory markers and IR, but not with hyperandrogenism in multivariate analysis.
Due to the paucity of data on the effect of PCOS on left ventricular (LV) geometry, De Jong et al. performed a study to determine whether PCOS contributes to the risk of developing left ventricular hypertrophy (LVH) in obese but normotensive women [23]. In their retrospective cross-sectional study, they analyzed collected echocardiographic parameters as well as clinical and metabolic data in 24 obese women with PCOS and 29 obese control women, all of whom were matched for age, BMI, and were normotensive. Exclusion factors, in addition to BMI < 30 kg/m2, were type 2 diabetes, hypertension or use of antihypertensive drugs, and prior heart or systemic disease. When comparing both groups, obese women with PCOS had increased LVM, regardless of whether they were corrected for BSA or height. Comparative analysis of LV geometric patterns showed a lower incidence of normal LV geometry in the PCOS group, with a slightly higher prevalence of eccentric hypertrophy and concentric remodeling compared with the control group and identified the presence of concentric LVH (25%), which was not observed at all in the obese control group. Both study groups had similar rates of normal diastolic function (around 70%), as well as similar rates of grade 1 diastolic dysfunction (DD) and grades 2 and 3 DD. However, concentric hypertrophy was not associated with DD, which may indicate compensatory changes in structure of the LV in women with PCOS, that were not seen in obese only women. The mechanisms responsible for the pathogenesis of concentric hypertrophy in women with PCOS remain elusive because of the complexity of PCOS, which often includes concomitant conditions such as hyperlipidemia, hypertension, insulin resistance, and hyperandrogenism. In this study, the PCOS group, despite having normal fasting glucose, lipid profiles (possibly in part due to metformin use), and blood pressure values, still showed a pattern of LV remodeling that was not observed in the obese group, suggesting that normalization of some of the associated metabolic abnormalities in PCOS may not be sufficient to reduce the increased cardiovascular risk. Additionally, the absence of fasting plasma insulin and androgen levels in the study participants further complicated the evaluation of the relationship between insulin resistance and androgen levels with LV remodeling in PCOS patients, further challenging the investigators.
Given the higher risk of developing CVD even in young patients with PCOS, it is important to identify subclinical left ventricular dysfunction (LVD) as early as possible in asymptomatic patients with preserved left ventricular ejection fraction. Echocardiography with Tissue Doppler Imaging (TDI), Myocardial Performance Index (MPI), Isovolumetric Relaxation Time (IVRT) or Global LV Longitudinal Strain (GLS) can be used for this purpose.
To ascertain whether a presystolic wave (PSW) and subclinical LVD measured by MPI in PCOS patients are related, Saylik and colleagues carried out a prospective study [24]. PSW as a late diastolic flow was obtained by Doppler in the LV outflow tract (LVOT). This paper demonstrated that PSW independently predicts subclinical LVD in PCOS patients and can be used for its early detection. A group of 106 patients diagnosed with PCOS were splited into two groups according to the presence of PSW. Thus, 58 patients, with a mean age of 23 years, had PSW and increased values of specific clinical parameters such as WHR, fasting insulin and HOMA-IR compared to the remaining 48 patients in whom PSW was not detected (average age of 25 years old). The group with the presence of PSW was distinguished by significantly increased MPI velocities as well as more often occurrence of subclinical LVD than in the group without PSW. There was a clear correlation between PSW and MPI velocities. The attendance PSW, HOMA-IR, and WHR > 85 predicted subclinical LVD in univariate logistic regression analysis, whereas only positive-PSW did so in multivariable logistic regression analysis.
One of the parameters of Doppler echocardiographic imaging is pulmonary artery stiffness (PAS), used to assess pulmonary artery mechanics and early detection of pulmonary hypertension. Another parameter in the assessment of pulmonary artery compliance is the right ventricular-pulmonary artery (RV-PA) coupling. Its abnormality indicates reduced PA compliance and significantly translates into the development of pulmonary artery hypertension (PAH). In a retrospective cohort study led by Abacioglu et al., both PAS and RV-PA coupling were assessed for the first time in patients with PCOS [25]. PAS was calculated as the ratio of maximal frequency shift of pulmonary flow (MFS) to the pulmonary acceleration time (AT), whereas the RV-PA coupling as a ratio of tricuspid annular plane systolic excursion (TAPSE) to the pulmonary artery systolic pressure (SPAP). A total of 104 women, 44 diagnosed with PCOS, were included in the study, all matched for age and BMI. The group of patients with PCOS was characterized by significantly elevated PAS values in comparison with women in the control group. These scores also showed a positive correlation with HOMA-IR. In addition, 34% of those enrolled were found to have abnormal RV-PA coupling. The risk of CVD is increased in patients with PCOS, and although most studies focus on left ventricular and coronary artery pathology, right ventricular dysfunction and pulmonary hypertension should not be overlooked, which can also affect mortality and limit quality of life.




Comments (0)