
Remember me
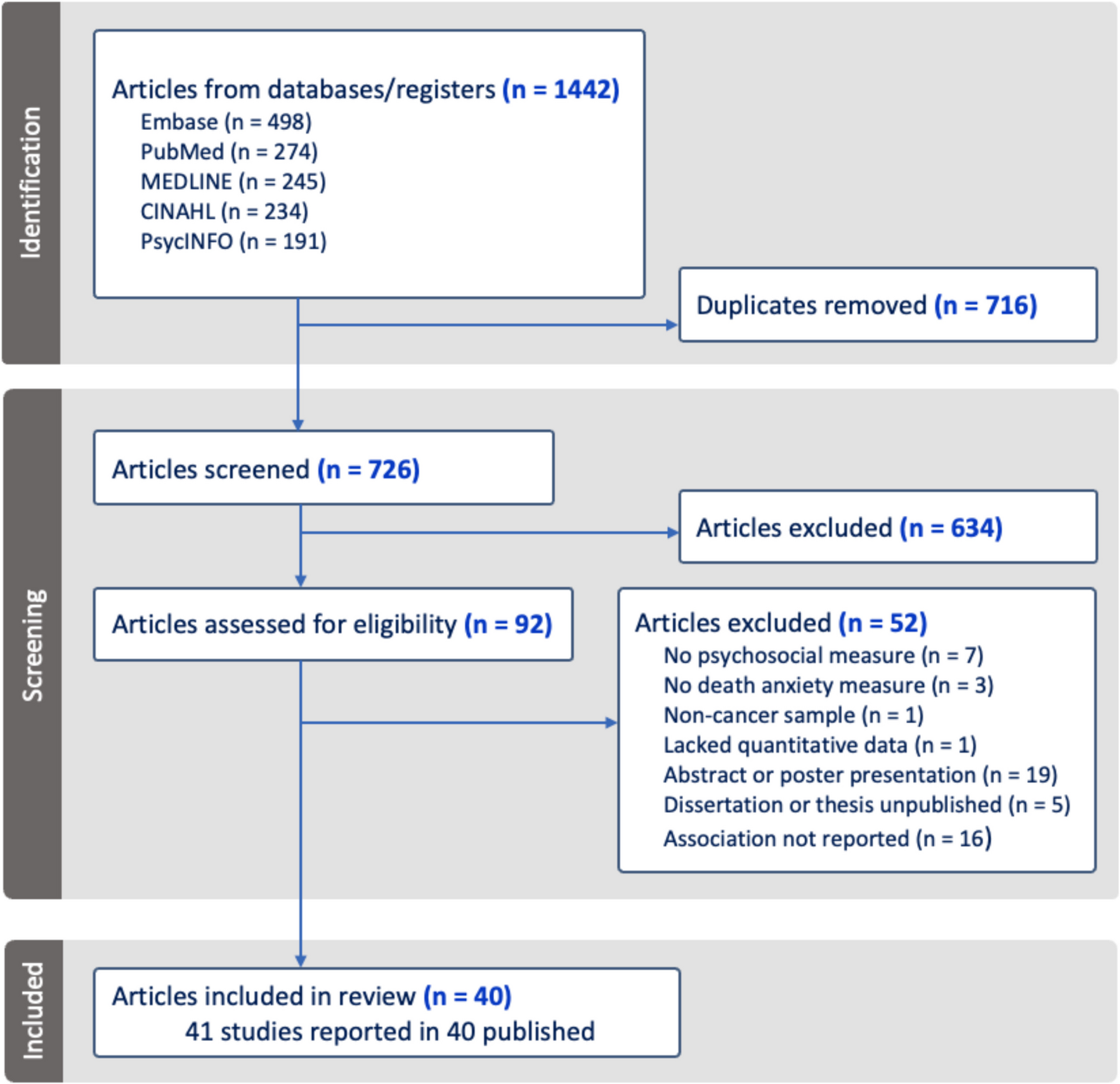
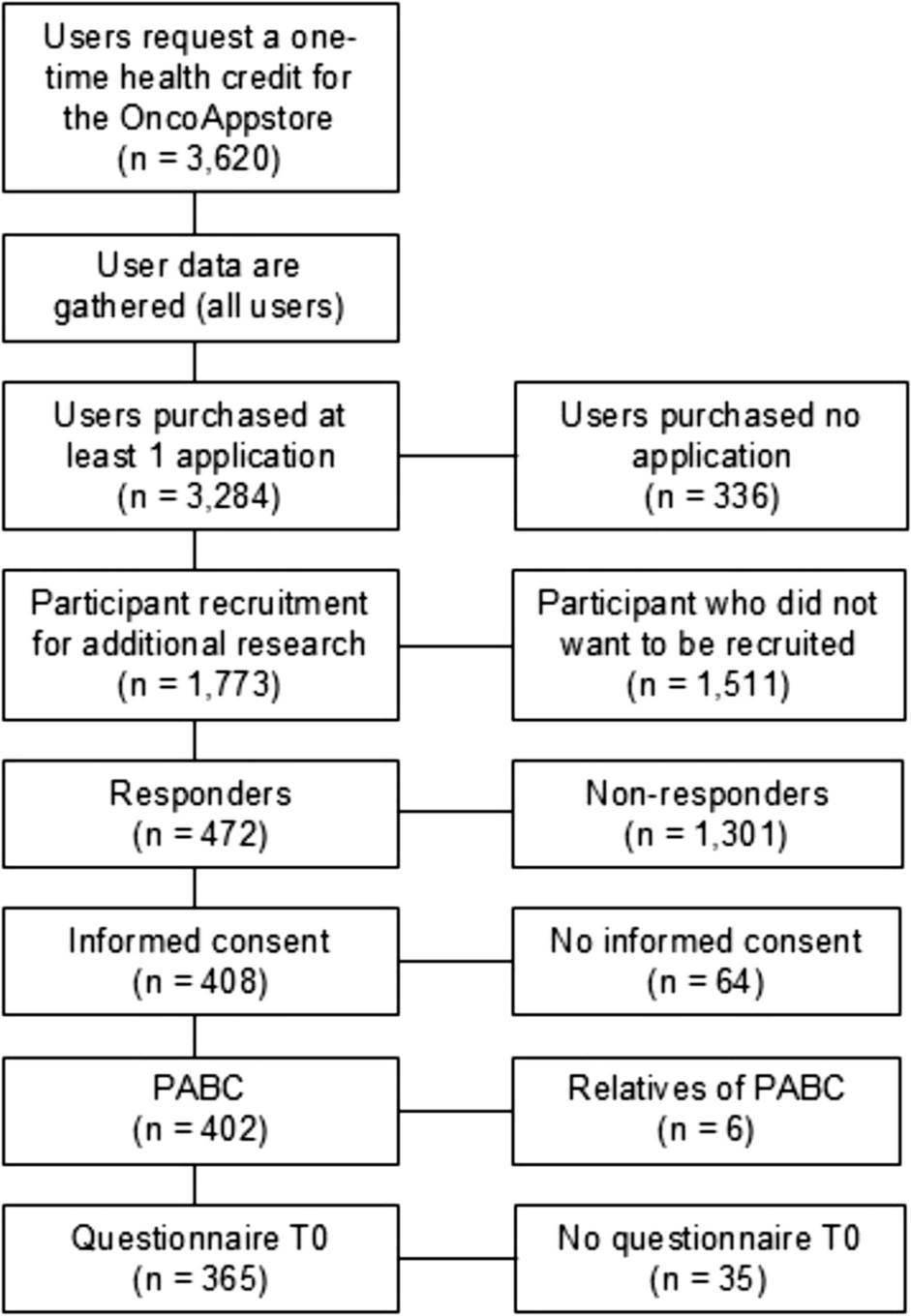
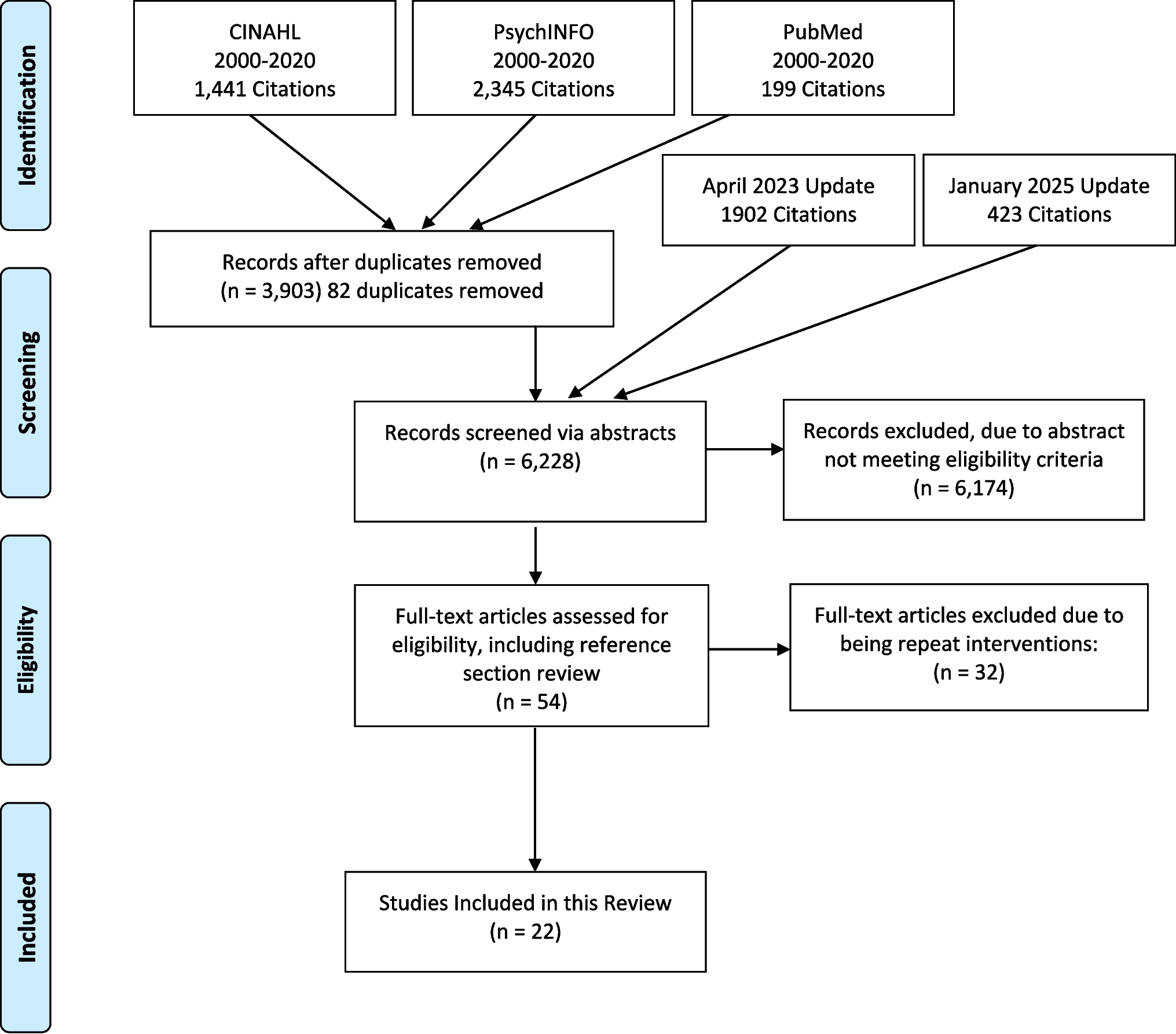
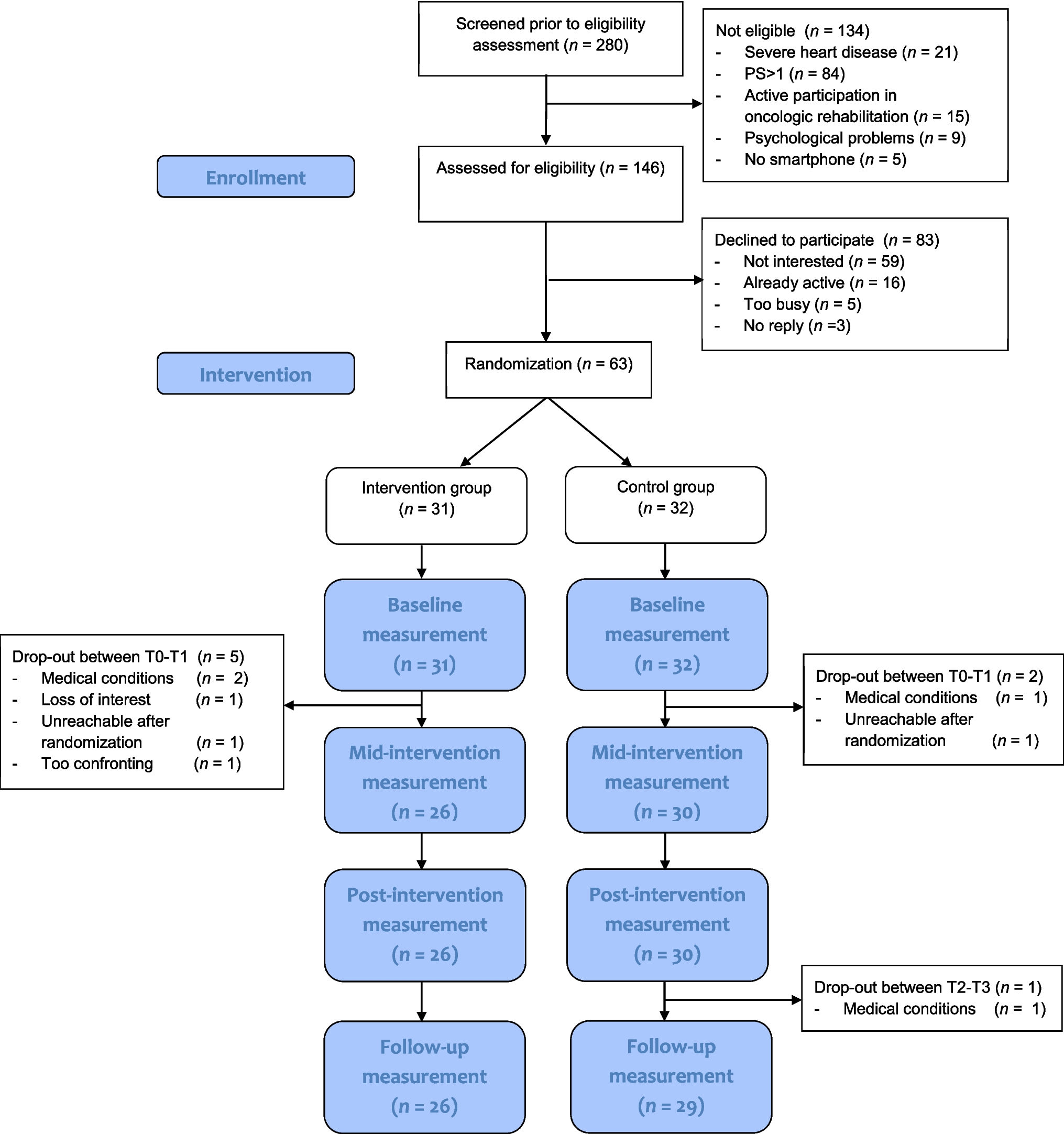
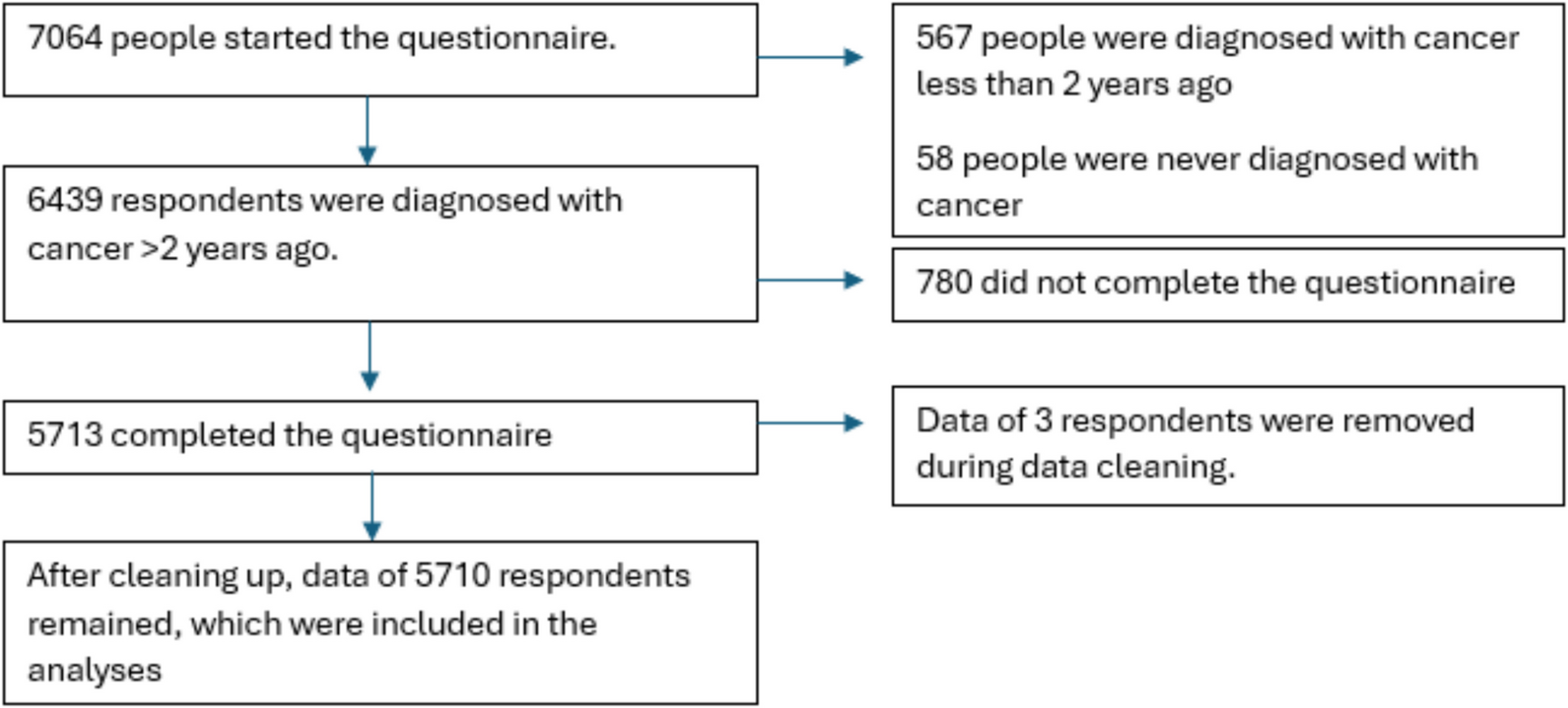

CONSORT diagram of the recruitment process
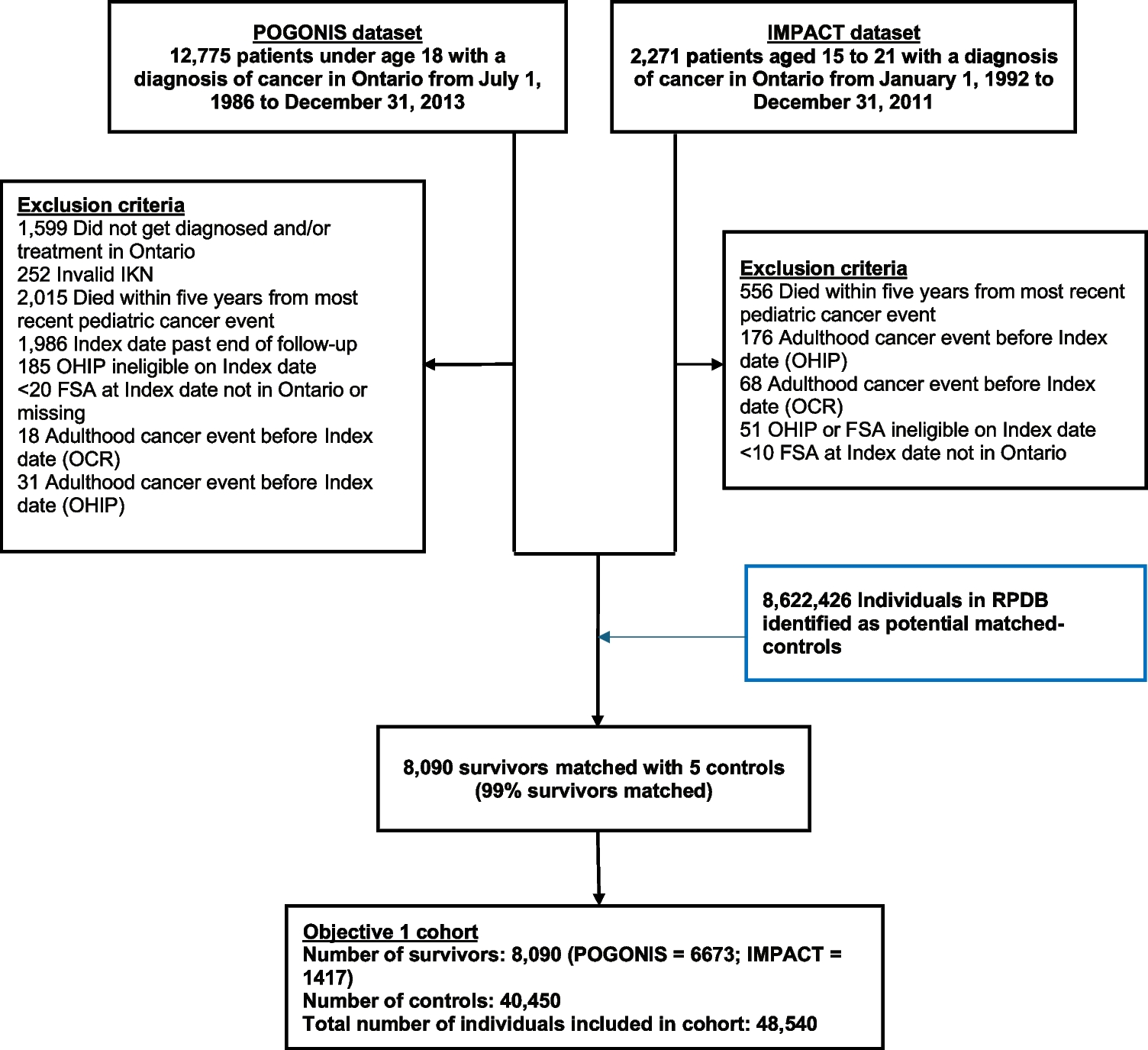
A total of 5894 potential participants (1946 cancer cases and 3948 controls) were initially invited by mail. One hundred sixty were excluded as ineligible and 3513 declined (2806 passively declined and 707 actively declined). A total of 2221 (38.7%) participants returned completed surveys. However, 146 did not sign the consent form and were excluded from the final sample to ensure compliance with the General Data Protection Regulation. This resulted in a final sample of 2075 respondents (36.2% return rate). Return rates for cancer groups were breast (45.6%), colorectal (42.7%), ovarian (45.3%) and 31.9% for the matched control group.
We compared the 2075 participants to 3507 decliners (3513 minus 6 opt-outs) across age, sex and social deprivation index scores. There were no differences by age or sex, but both the cancer survivors and matched controls had higher levels of participation in the least socially deprived groups compared to the most deprived groups (p < 0.001).
Demographic and clinical dataTable 2 shows the sex, age, IMD and comorbidity characteristics of the overall cancer survivor and the matched control groups, in addition to each subgroup (breast, ovarian and colorectal cancer survivors and their individual control groups). As expected, due to the matching process, the groups were similar in sex, age and IMD profiles and also reported a similar number of comorbidities.
Table 2 Proportions of sex, age ranges, IMD and no of comorbidities across the cancer survivor and matched control groupsQLACSGeneric summary scoresT-test comparisons of the QLACS generic summary scores demonstrated that the total cohort of cancer survivors scored higher (M = 74, SD = 28.5) than the matched controls (M = 70.6, SD = 37.5), indicating worse QoL (p = 0.007), although the effect size was modest (ω2 = 0.121).
Comparisons between individual cancer survivor groups and matched controls identified that although all cancer survivor groups had higher (worse) scores, none of these was statistically significant.
Domain scores (Table 3)Table 3 QLACS individual domain scores split by cancer survivors and matched controlsComparisons between all cancer survivors and matched controls across all QLACS domains, excluding the cancer-specific domains (e.g. distress about recurrence and benefits of cancer), showed that cancer survivors scored higher (worse) across energy/fatigue (p = 0.002), financial problems (p < 0.001), distress about family cancer (p < 0.001), concerns about appearance (p < 0.001), sexual interest/function (p < 0.001) and social avoidance (p = 0.004). There were no significant differences across the other domains.
In comparing individual cancer groups to their matched controls (Supplementary file/Table 4), we found statistically significant differences between the breast survivors and matched controls across energy/fatigue (p = 0.004), financial problems (p < 0.001), distress about family cancer (p < 0.001), concerns about appearance (p < 0.001), sexual interest/function (p = 0.002) and social avoidance (p = 0.004). There were significant differences between the colorectal group and matched controls across financial problems (p < 0.001), distress about family cancer (p < 0.001) and concerns about appearance (p < 0.001). There was a significant difference between ovarian survivors and matched controls on financial problems (p = 0.001). There were no statistically significant differences between groups on any of the other domains of QLACS.
Cancer-specific summary scoreThe three cancer survivor groups were compared on the cancer-specific summary score of the QLACS using a Kruskal–Wallis test. Statistically significant differences were identified (p < 0.001), with the breast group scoring highest (indicating worse QoL), followed by the ovarian group and then the colorectal. Subsequent pairwise analysis using Mann Whitney U revealed the differences were between the breast and colorectal groups (p < 0.001) only.
EORTC symptom subscales (Table 3)Comparisons of the symptom subscale scores of the cancer survivors with their matched controls using Mann Whitney U tests found no significant differences across groups on muscular pain, urinary frequency, urinary incontinence, GI symptoms or constipation. The cancer survivor group reported significantly worse (higher) scores than the matched controls on tingling and numbness (p = 0.001), urinary symptoms (p < 0.001), diarrhoea (p < 0.001) and abdominal/GI symptoms (p < 0.001).
Comparison of the individual cancer groups (breast, colorectal and ovarian) and their specific matched control groups identified worse tingling and numbness (p = 0.009) amongst the breast cancer cohort versus their matched controls, but no differences on any other symptoms. The colorectal survivors scored worse than their matched control counterparts on urinary symptoms (p < 0.001), diarrhoea (p < 0.001) and abdominal/GI symptoms (p < 0.001). There were no significant differences on any of the symptom subscales between the ovarian cancer survivors and their matched controls. The full scores are outlined in the Supplementary file/Table 4.
EQ-5D-3L (Fig. 2)Fig. 2
Comparison of cancer survivors and matched controls on EQ-5D-3L domains
Utility scores and VASNo statistically significant differences between the cancer survivor and control cohorts were found for the EQ-5D-3L utility scores or VAS scores.
Domain scoresChi-square analyses assessed differences in the proportion of cancer survivors and matched controls reporting any level of problem across the domains of the EQ-5D-3L and showed no statistically significant differences between groups on mobility, pain or self-care. However, a higher proportion of participants in the cancer survivor group reported problems with usual activities (30.2% vs 23.2%, X2 = 12.69, p < 0.001) and anxiety/depression (32.4% vs 26.2%, X2 = 9.29, p = 0.002) than those in the matched control group.
The colorectal cancer group reported significantly more problems with usual activities than their matched controls (32.1% vs 21.7%, p < 0.001). There were no other significant differences between the individual cancer groups and matched controls on any of the EQ-5D-3L domains. The comparisons are illustrated in the Supplementary file/Fig. 3.
Cancer survivor identity (Supplementary file/Fig. 4)There was a significant difference (X2 = 50.84, p < 0.001) between the cancer survivor group and the matched controls on the cancer survivor identity question (how they chose to describe someone who has had cancer). A higher number of participants in the cancer survivor group selected the option ‘A person who has had cancer’ than in the matched control group (55.9% versus 46.1%). A higher number of participants in the matched control group selected ‘A victim of cancer’ than in the cancer survivor group (8.2% versus 1.5%).
Differences between the breast cancer survivors and matched controls (X2 = 32.131, p < 0.001) and the colorectal survivors and matched controls (X2 = 27.882, p < 0.001) were significant, but not between the ovarian cancer group and matched controls. Responses across all subgroups had a similar pattern with cancer survivors being more likely to describe themselves as ‘A person who has had cancer’ and less likely to describe themselves as ‘A victim of cancer’.
Healthcare usage and personal financesCancer Care Co-ordination Questionnaire (CCCQ)Comparing the cancer survivors and matched controls on the navigation subscale of the CCCQ found no significant differences between any of the cancer survivor groups and their matched controls.
Healthcare usageIn terms of services used in the past 3 months, there were no statistically significant differences in the proportion of cancer survivors and matched controls who reported seeing their GP or ‘other’ healthcare providers, seeing a healthcare professional for emotional issues or problems with alcohol or drugs or accessing hospice care. A higher proportion of matched control participants reported seeing a physiotherapist (12.0% vs 8.3%, p = 0.009). No statistically significant differences between individual cancer survivor groups were observed when compared to matched controls.
Cancer survivors reported different patterns of hospital-based healthcare, being more likely than matched controls to require hospital care in the past 3 months (51.1% vs 44.1%) and more likely to access most of their care outside LTHT (p < 0.001). Differences between the breast survivors and matched controls were statistically significant in this regard (p < 0.001), as were differences between the ovarian survivors and matched controls (p = 0.003), with similar patterns observed. There were no differences between the colorectal survivors and matched controls.
A significantly higher proportion of cancer survivors reported accessing some type of voluntary or charity services (6.5% vs 3.8%, p < 0.001). However, the descriptions of services accessed were very heterogeneous and not always related to cancer.
Providing and receiving careThe matched control group was significantly more likely than the cancer survivor group to report providing care for someone else in the past 3 months (36.4% vs 29.9%, p = 0.002). These differences were significant between the breast survivor and control groups (p < 0.001) and the colorectal survivor and control groups (p = 0.004). However, there were no significant differences between the ovarian survivors and the control group.
Cancer survivors were more likely than their matched controls to report receiving care from someone else in the past 3 months (25.1% vs 18.9%, p < 0.001). These differences were significant between the colorectal survivors and their control group (p < 0.001) but not between the breast and ovarian survivors and their control groups.
There were no significant differences reported in the mean hours of care support received, the proportion of carers taking time off work and the mean number of hours that carers took off work.
Employment and income (Supplementary file/Table 5)Statistical comparisons of employment status were not possible due to the small sample size, since the majority of participants in both groups were retired (61.4% of cancer survivors and 64.0% of matched controls). Reported income losses over the past 3 months were similar across both groups.
Medication, travel and other costsCancer survivors were less likely than matched controls to pay for their prescription medications (7.6% vs 17.9%, p < 0.001). However, there were no significant differences between the groups on costs of health and social care-related travel and parking or time spent travelling. The matched control group reported a higher expenditure on ‘other’ health and related costs than the cancer survivor group (£65 vs £37, p = 0.002). However, the description and amount of costs were very heterogeneous and included some descriptions that were not specifically cancer related (e.g. dentistry or house renovations).
Comments (0)