
Remember me

The trial was designed as a double-blinded study, involving both assessors and patients, and was conducted as a randomized control clinical study with two parallel simultaneous groups, each with an equal allocation ratio. The trail protocol was officially reported on ClinicalTrials.gov under the ID number NCT04720638. The trial took place at the Conservative Dentistry outpatient clinic of the Faculty of Dentistry at Cairo University, Egypt, spanning from March 2021 to December 2022. The reporting of this trial followed the guidelines established by the Consolidated Standards of Reporting Trials (CONSORT). Furthermore, this trial received approval from the Ethics Committee of the Faculty of Dentistry at Cairo University, with an ID number of (13/11/20). All participants were instructed about the trial's objectives and procedures, and their participation was confirmed through informed consent, which they provided by signing the forms.
Eligibility criteriaPatients included in this study were 18–55 years old with good oral hygiene and presenting with at least one upper or lower vital posterior tooth with compound proximal carious cavity. The selected tooth should be in favorable occlusion and normal contact with the adjacent teeth. The exclusion criteria were patients with compromised medical health, pregnant women, known allergy to any material used in the trial, signs and symptoms of irreversible pulpitis or necrosis or any other pulp pathologies and previous restoration or severe periodontal problems in the selected tooth.
Sample size calculationBased on the findings from a prior clinical trail [23], a power analysis was devised to facilitate the application of a two-sided statistical test aimed at assessing the null hypothesis. By setting the Alpha (α) level at 0.05 (5%) and the beta (β) level at 0.20 (20%), thus ensuring a statistical power of 80%, and by determining an effect size (W) of 0.400, the projected sample size (n) was computed to encompass a total of 60 cases. In anticipation of potential dropouts, this number was subsequently increased by 15%, resulting in a final total of 70 cases, which corresponds to 35 cases per group. The calculations for sample size were conducted utilizing G*Power version 3.1.9.4 (citation may be needed https://link.springer.com/article/https://doi.org/10.3758/BF03193146), a widely recognized software tool for statistical analysis.
Randomization and concealment of allocationThe process of randomization was executed utilizing a straightforward approach overseen by a contributor who maintained no further involvement in subsequent trial phases. A total of seventy random numbers were generated employing the Random Sequence Generator (https://www.random.org/). This list of random numbers was then sealed securely within an opaque envelope. Access to this list was restricted exclusively to the operator, who could only open the envelope at the precise moment of applying the composite filling material, subsequent to the completion of the adhesive protocol. Both the two assessors responsible for evaluating trial outcomes and the patients remained unaware of the specific restorative material employed, ensuring a double-blind setup. Blinding of the operator was not applicable due to variances in the techniques of application required for the different materials.
Interventions: restorative treatmentA single trained operator performed all the restorations. All patients received local anesthesia (Artinibsa 4% 1:100.000, Inibsa Dental, Spain). Multiple teeth isolation was done using a rubber dam (Sanctuary® powder free latex dental dam, Malaysia). Preparation of all cavities was applied using # 245 and # 1, 2 round carbide burs with an air/water-cooled high speed handpiece with the aid of a sharp excavator in accordance with the cavity preparation principles for adhesive composite restorations and the recent clinical recommendations for caries excavation.
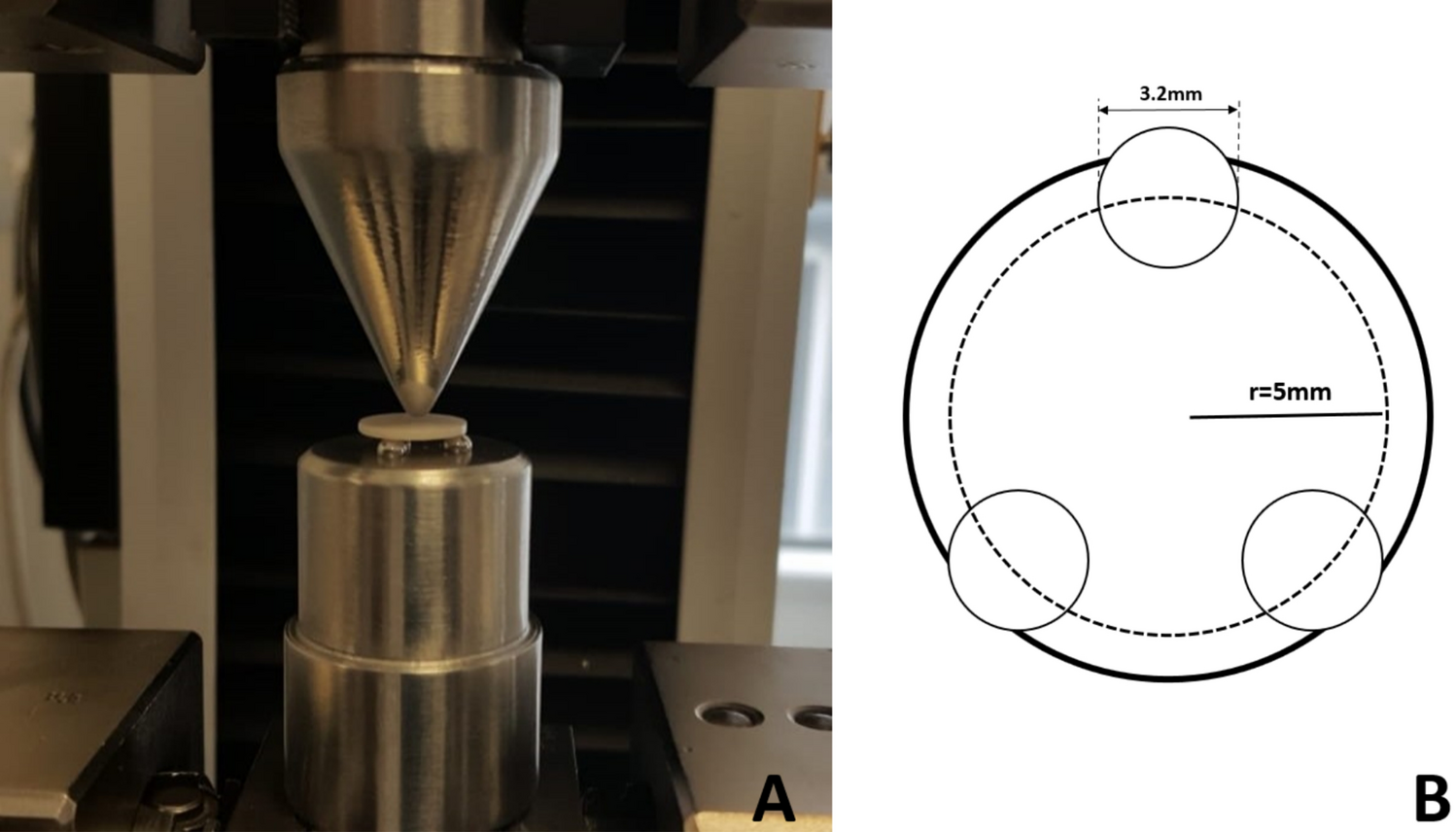
For the restorative procedures, first, the lost proximal wall was replaced using an appropriate pre-contoured sectional matrix complemented by the corresponding separating ring (TOR VM, Russia) and an appropriately dimensioned wooden wedge (Fig. 1). The prepared cavity was cleansed by applying a thorough water rinse then application of the bonding protocol. All teeth in both groups received the same adhesive protocol. A selective enamel etching approach was made by applying 37% phosphoric acid gel (Scotchbond, 3M ESPE, USA) for a duration of 15 s. Subsequently, the tooth underwent a 15 s rinsing procedure with water and was gently dried using brief air blasts and cotton pellet blotting. A one-step self-etch bonding agent application (G-ænial Bond, GC) involved a thorough and careful process where a disposable microbrush was used to gently spread the bonding agent over the surfaces of the prepared cavity. Following this application, it was left for a period of 10 s before being exposed to the highest air pressure for 5 s. Subsequently, the light-curing procedure was performed utilizing an LED light-curing unit with an intensity surpassing 700 mW/cm2 (LED.F, Woodpecker, China) for a total time span of 10 s.
Fig. 1
(A) Preoperative view; (B) after removal of the old restoration; (C) interproximal walls were built by flowable SFRC; (D) post-operative view
In the intervention group, flowable SFRC (everX Flow) was injected as dentin replacement including the proximal wall (Fig. 1) leaving about 1–2 mm of space for an occlusal surface layer of the conventional PFC. SFRC was subjected to light curing for 20 s. A capping or surface layer of the conventional micro-hybrid PFC (G-ænial Posterior, GC) was applied and underwent light curing for a period of 20 s as well.
While for the control group, the cavities were completely filled with conventional PFC, using an oblique 2 mm incremental layering technique, and each increment subjected to light curing separately for 20 s.
After checking centric and eccentric occlusion by an articulating paper, restoration finishing was done, using fine grit bud-shaped diamond stones (Microdont, Brazil) then polishing by rubber points and bristle brushes with ultrafine Microdont diamond paste (Microdont). All the used materials and their specification are mentioned in Table 1.
Table 1 Material descriptions and specificationsClinical evaluationRestoration evaluation was performed by two blinded outcome investigators using modified USPHS criteria (Table 2). The examiners were trained on the modified USPHS criteria before starting the trial and calibrated to at least a kappa value of 90% per each criteria for inter- and intra-examiner agreement. The assessments of the restorations were conducted at baseline, 6-month, 12-month, and 18-month intervals. Any discrepancies in the scores were resolved through discussion.
Table 2 Modified USPHS criteriaStatistical analysisNumerical (age) data were expressed as mean values along with standard deviations (SD) and assessed for normality through the Shapiro–Wilk test, which confirmed their adherence to a normal distribution. Subsequently, independent t tests were employed for comparisons. Categorical and ordinal data were presented as percentages and frequencies. Chi-square tests were utilized for the analysis of categorical (gender and treated teeth) data, such as gender and treated teeth. For ordinal data, specifically USPHS scores, intergroup comparisons were conducted using the Mann–Whitney U test, while intragroup comparisons employed the Friedman’s test, followed by the Nemenyi post hoc test. A significance threshold of p < 0.05 was applied to all tests. The statistical analysis was executed using R statistical analysis software, version 4.1.3.
Comments (0)