
Remember me
The integration of PET and contrast-enhanced CT (ceCT) marks a significant advance in the diagnosis of well-differentiated NET. PET provides additional functional information to established morphological imaging, facilitating the detection of the primary tumor and small metastases, while also significantly influencing therapeutic decisions [5].
Conventional CT plays a pivotal role in the diagnosis and management of NEN due to its widespread availability, high-resolution detail, and rapid examination speed, even for multiphasic protocols. It can assess tumor extension by showing whether the tumor is locally limited or has spread to surrounding structures, such as lymph nodes, visceral organs, or bones. Particularly for surgical planning, accurate anatomical knowledge of the tumor and its metastases is essential.
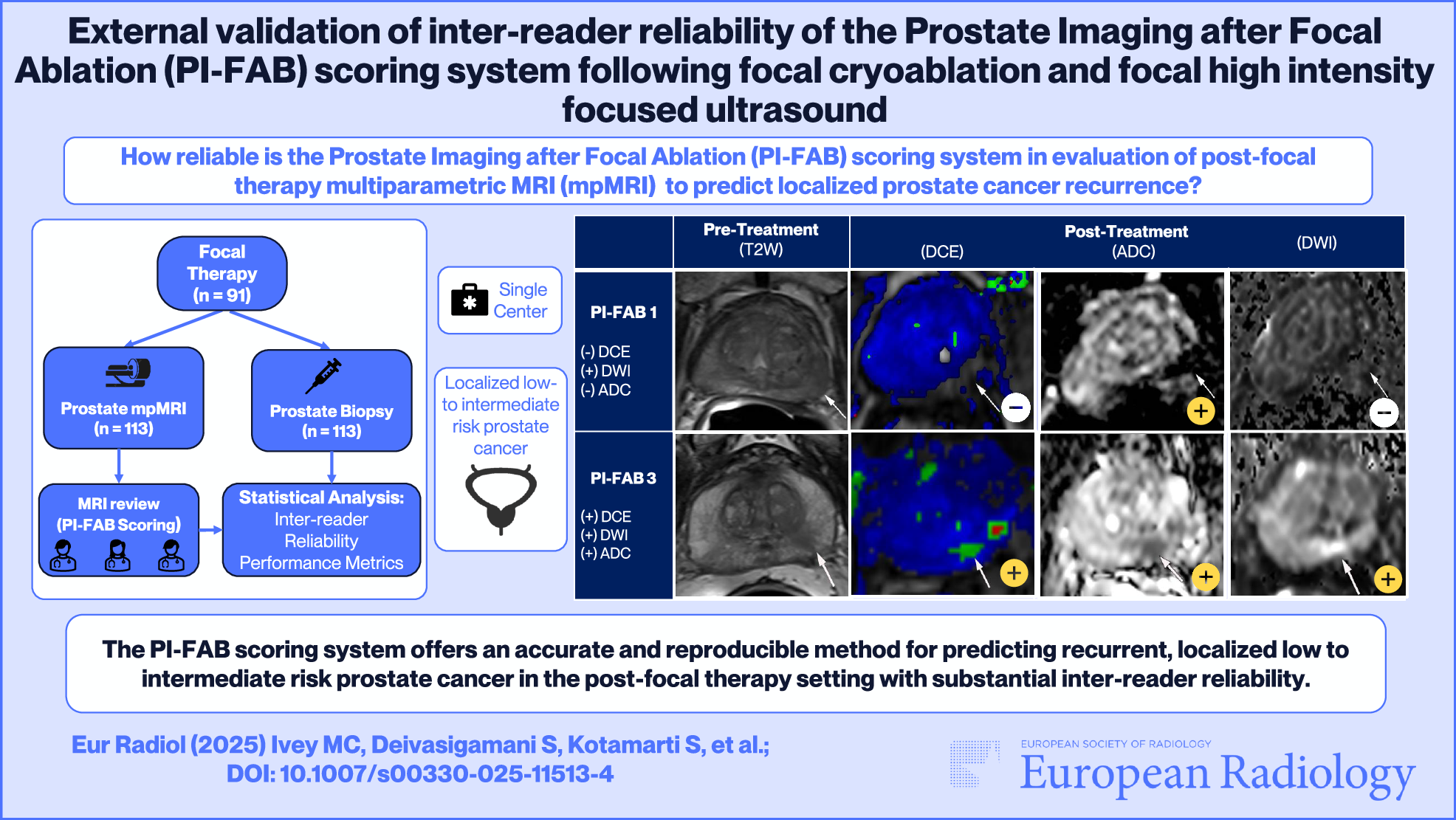
Patient preparation and a dedicated CT protocol have a major influence on the value of the examination and should therefore be carried out carefully and tailored to the respective diagnostic question. The use of an iodine-based intravenous contrast agent is important, as it significantly increases sensitivity in detecting tumors and metastases. For gastrointestinal NET, which typically shows significant arterial contrast uptake and tends to metastasize to the liver, multiphase CT scans of the upper abdomen are useful [6]. Figure 2 includes comprehensive imaging findings of a patient with a neuroendocrine tumor and disseminated liver metastases, highlighting their behavior across multiple diagnostic modalities.
Fig. 2
Patient presented with disseminated liver metastases (b) of histologically confirmed neuroendocrine tumor (G2, Ki-67 5%). Disseminated liver metastases exhibited early arterial contrast enhancement in ceCT (a) with subsequent early washout in portal venous phase (c). Liver metastases were clearly visible on magnetic resonance imaging (MRI) (including contrast-enhanced T1 sequence and diffusion-weighted imaging (DWI)-sequences) (e, f) and demonstrated intense SSR overexpression (d)
Still, conventional CT alone has lower accuracy in identifying lymph node metastases compared with SSR-PET/CT [7]. One reason for this is the size threshold used in anatomical-morphological imaging to differentiate between benign and malignant lymph nodes. Smaller tumor lesions may therefore be missed or mistakenly classified as benign. Only about 65% of lymph node metastases detectable by SSR-PET/CT through radionuclide uptake are identifiable and accurately characterized using conventional imaging techniques. Also, the average accuracy of CT in detecting the primary tumor, liver metastases, and extrahepatic metastases is only 73%, 80%, and 75%, respectively [8].
Although an unenhanced low-dose scan may suffice for anatomical orientation and attenuation correction in PET/CT, a contrast-enhanced scan is recommended for a comprehensive evaluation of mediastinal and abdominal structures. The use of positive oral (iodine-containing) contrast agents is not recommended in CT scans to avoid missing small tumors within the intestinal and gastric walls [9].
SSR-PET/CTIn clinical practice, a range of radiopharmaceuticals is available for SSR-directed imaging, each demonstrating a high affinity particularly for SSR subtype 2. The most frequently utilized SSA, including DOTA-TATE, DOTA-TOC, and DOTA-NOC, vary in their affinity for different SSR subtypes. However, linked with the radionuclide [68Ga], they are regarded as equally effective in terms of diagnostic accuracy for imaging NET [10].
SSR-PET/CT with [68Ga]-DOTA-conjugated SSA has been approved by the Food and Drug Administration and European Medicines Agency for imaging of well-differentiated NET and is now considered the ENETS-recommended reference standard for this purpose [8]. While the synthesis of [68Ga]-DOTA-conjugated peptides for NET imaging is well-established, reliable, and features relatively simple radiochemistry, challenges such as small-scale production and the short 68-min half-life of [68Ga] persist. However, the recent development and clinical application of a new SSR-ligand, [18F]-SiFAlin-TATE, offers significant improvements in acquiring SSR-PET/CT images for patients with NET. The cyclotron-produced radionuclide [18F] has a half-life of 110 min, providing an optimal window for synthesis, transport, and in-vivo distribution, while minimizing radiation exposure to the patient [8]. Furthermore, [18F]-labeled tracers emit positrons with lower energy, leading to higher-resolution images. For [18F]-SiFAlin-TATE, significantly higher tumor uptake was described in almost all tumor lesions in common metastatic sites of NET, including the liver, lymph nodes, and bone, but not in lung lesions [11]. The development of cyclotron-derived, [18F]-labeled compounds for NET imaging might solve the disadvantages of a cost-intensive Germanium-68 [68Ge]-/[68Ga]-generator, low activity amounts after single elution, and the shorter half-life of [68Ga]-labeled compounds [12].
Baseline SSR imaging with PET/CT is recommended by the ENETS guidelines for every NET G1 or G2 [13]. For G1-NET or G2-NET, SSR-PET/CT is recommended, except in specific cases such as gastric NET type I or G1 rectal NET with a diameter of less than 1 cm and no adverse features. In these instances, alternative diagnostic approaches (CT, MRI, ultrasound) may be more appropriate due to the typically indolent nature of these tumors and their lower probability of developing metastases. SSR imaging should be considered for re-staging after potentially curative surgery in patients with a clinically significant risk of residual or metastatic disease, even if SSR imaging was not performed before surgery. Similarly, SSR imaging is deemed necessary for re-staging after non-curative surgery in all patients, complementing conventional imaging methods [14]. When clinical or laboratory indicators suggest progression, the recommended imaging approach for SSR-positive NET involves combining SSR imaging with CT and/or MRI. If SSR imaging detects a new lesion on a PET scan while the anatomical-morphological CT scan shows stable disease, the disease may be indeed advancing. Some organs, such as the thyroid and adrenal gland, or inflammatory conditions, can accumulate SSR radiotracers due to their slight expression of SSR. This underscores the need for careful evaluation when interpreting scan results, especially because the CT component of SSR-PET/CT can significantly aid in diagnostic guidance [15].
In the evaluation of SSR-PET/CT scans, the description of malignant NET lesions, and their increased receptor density is traditionally documented in a descriptive manner. This assessment primarily relies on comparing the SSR-uptake of the NET manifestations to that of the liver, known as the Krenning score [16]. Recently, a new standardized reporting system, SSTR-RADS 1.0 has been introduced. This system is modeled after the established and widely used “Reporting and Data System” (RADS) frameworks that are widespread in other imaging modalities and tumor entities. SSTR-RADS 1.0 is specifically designed to standardize the interpretation of SSR-PET/CT scans and to aid in the decision whether or not NET patients are suitable for PRRT [17], a receptor-targeted radiotherapy for NET, aimed with high affinity and specificity at SSR and involves the systemic administration of a radioactively labeled peptide. DOTA-TATE combined with therapeutic beta-emitting radionuclides like [177Lu] or Yttrium-90 ([90Y]) enables effective treatment. PRRT is used in the management of inoperable or metastasized, well-differentiated NET and is particularly useful for patients with tumor progression under biotherapy with SSA. SSA play a pivotal role in managing NET, particularly in alleviating symptoms associated with carcinoid syndrome and tumor growth. However, for cases unsuitable for chemotherapy due to their slow growth behavior, such as NET G1 and G2, and when curative tumor resection or other local ablative methods are not feasible, PRRT emerges as a promising therapeutic option [18]. As de-differentiated, SSR-negative lesions cannot be targeted by PRRT, an additional [18F]FDG-PET/CT may be beneficial for patients with NET G2 or G3. This helps identify discordant FDG-positive, SSR-negative lesions, which are known prognostic markers for poor outcome after PRRT [19].
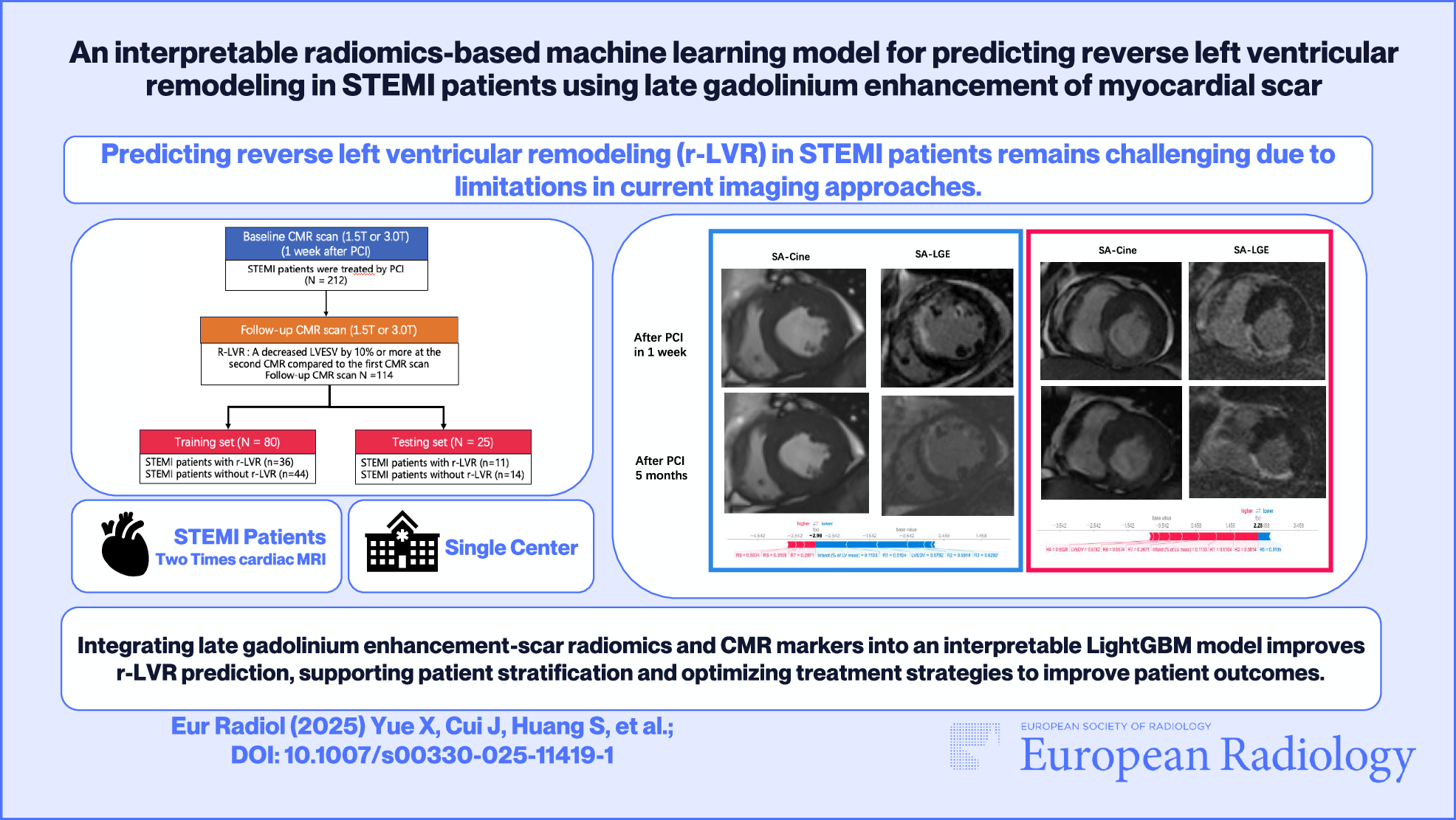
The NETTER-1 study has shown good tolerability and efficacy of [177Lu]Lu-DOTA-TATE compared to high-dose SSA (“Octreotide”) in patients with progressing, metastasizing midgut NET. Patients with strong SSR expression and stable disease but who have therapy-resistant clinical symptoms are suitable for PRRT [14]. Figure 3 provides a detailed comparison of imaging data from [18F]-SiFAlin-TATE PET/CT and MRI scans following second-line PRRT treatment with [177Lu]Lu-DOTA-TATE. The figure compares various imaging modalities, demonstrating a reduction in lesion size and SSR expression, along with changes in diffusion characteristics, indicative of a positive therapeutic response.
Fig. 3
Histologically confirmed NET of the pancreas with multiple liver metastases (G2, Ki67% 10–20%) depicted in [18F]-SiFAlin-TATE PET/CT and MRI scan. After chemotherapy with Streptozotocin and 5-Fluorouracil, SSR-PET/CT showed tumor progression, multidisciplinary team recommended second-line PRRT with [177Lu]Lu-DOTA-TATE. Comparison of Maximum Intensity Projection (MIP, a1–a3), contrast-enhanced CT (ceCT, b1–b3), SSR-PET/CT (c1–c3), contrast-enhanced MRI (d1, d3) with diffusion-weighted imaging (DWI, e1, e3) sequences show a size reduction of the lesions in ceCT and MRI, reduced SSR expression and reduced diffusion restriction as signs of a therapeutic response
[18F]FDG-PET/CTImaging with the glucose analog [18F]FDG is particularly useful in aggressive NEN, such as well-differentiated NET G3 or poorly differentiated NEC, characterized by a high Ki-67 index and typically lower tumor SSR expression. However, [18F]FDG-PET/CT can also be useful in NET G1 or G2 to provide prognostic information as high uptake correlates with an increased risk of early progression, while low uptake characterizes rather indolent tumors [19]. Furthermore, [18F]FDG-PET/CT can contribute to biopsy planning in cases of unclear disease courses and the characterization of tumor heterogeneity.
Tumor heterogeneity in NEN complicates treatment by creating variability in how different tumor regions respond to therapy. Different parts of the same tumor may show varying levels of receptor expression or metabolic activity, leading to uneven responses to targeted PRRT or chemotherapy. This inconsistency can lead to partial treatment success—some areas of the tumor may shrink or stabilize, while others continue to grow or spread. Additionally, heterogeneity can lead to rapid development of resistance to therapies, as more aggressive tumor clones that are less responsive to standard treatments may emerge. This aspect necessitates frequent reassessment of the disease and may require a combination of therapeutic strategies to manage the disease effectively over time [20].
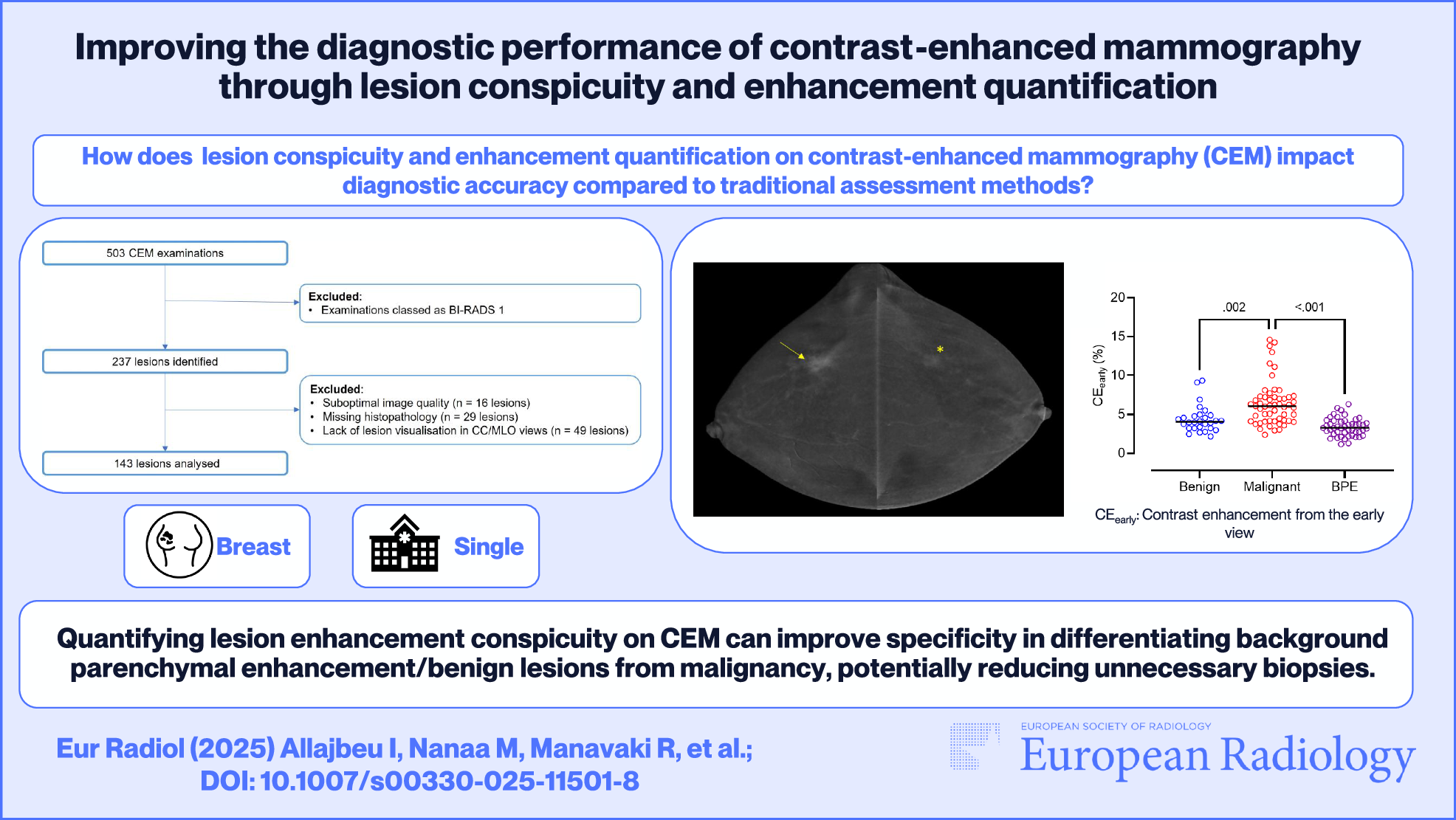
[18F]FDG-PET/CT is also indicated in NET cases where there are suspicious findings on conventional imaging (CT or MRI), but no SSR expression is observed during staging, or in patients with rapid progression of disease despite earlier low-grade disease on pathology. Due to the high risk of metastatic disease, [18F]FDG-PET/CT is recommended by the ENETS guidelines for NEC of the gastrointestinal tract before (curative) surgery and adjuvant chemotherapy. Carboplatin combined with etoposide is recommended as the first-line treatment. Should additional treatment be necessary, irinotecan paired with fluoropyrimidines has the best evidence as a second-line treatment [21]. Figure 4 includes comparisons of [18F]-SiFAlin-TATE PET/CT and [18F]FDG-PET/CT imaging results, illustrating specific uptake patterns and metabolic activity in the pancreas and liver.
Fig. 4
NET of the pancreas, with histological tumor grade G2 and G3. [18F]SiTATE PET/CT imaging (top row, a–c) revealed intense uptake in the body and tail of the pancreas and SSR-expressing liver metastases in segments II/III. FDG imaging (bottom row, d–f) indicated less extensive metabolic activity in the pancreatic tail, aligning with the histologically confirmed de-differentiated components. The liver metastases exhibited no increased metabolic activity
Comments (0)