
Remember me

This was a single-center cross-sectional study conducted at the Third Affiliated Hospital of Sun Yat-sen University from December 2020 to December 2021. Consecutive hospitalized patients in the Department of Endocrinology or Cardiovascular Medicine who underwent abdominal color doppler ultrasound, echocardiography and 12-lead Holter system were enrolled. Participants younger than 18 years old (n = 14); those with overt central nervous system disease and secondary peripheral nerve damage (n = 53); Individuals who began taking medications affecting autonomic nerve activity and heart rate over the past week (n = 58); Individuals who have severe hepatic and renal dysfunction (n = 36); endocrine diseases such as hyperthyroidism, hypothyroidism and electrolyte disturbance (n = 34); individuals with overt heart failure with a New York Heart Association (NYHA) functional classification of III and IV, left ventricular ejection fraction (LVEF) less than 50%, history of primary cardiomyopathy, severe valvulopathy, myocarditis and chronic atrial fibrillation (n = 289); those with uncontrolled hypertension (systolic blood pressure ≥ 150 mmHg, diastolic blood pressure ≥ 95mmHg) with stable antihypertensive drugs for at least 4 weeks (n = 78); patients with cancer (n = 31); individuals with drug abuse (n = 19); those with inadequate information (n = 66); and pregnant women (n = 7) were excluded. Finally, a total of 380 participants was enrolled for analysis, including 249 type 2 diabetic patients diagnosed according to the 1999 criteria of the World Health Organization [12], and 131 non-diabetic patients as the control group. Ethics approval was obtained from the Third Affiliated Hospital of Sun Yat-sen University network ethics committee, in accordance with the ethical guidelines of the 1975 Declaration of Helsinki [13]. Informed consent was obtained from all participants. Power analyses based on our sample size were carried out using the Monte Carlo Methods [14].
Measurement of adipose tissuesMediators were adipose tissues at four locations, including subcutaneous adipose tissue (SAT), extraperitoneal adipose tissue (EPAT), intraperitoneal adipose tissue (IPAT) and epicardial adipose tissue (EAT), which utilized for analysis to explore the effects of various adipose tissues on HRV. The thicknesses of these adipose tissues were measured using abdominal color Doppler ultrasound or echocardiography. To assess SAT, the abdominal wall fat thickness was measured 1 cm above the umbilicus in a longitudinal section along the line between the xiphoid process and umbilicus. EPAT was evaluated by measuring the distance between the left extrahepatic peritoneum and the abdominal white line under the xiphoid process. The thickness of IPAT was determined by measuring the distance between the posterior wall of the abdominal aorta and the peritoneum, also 1 cm above the umbilicus, in a cross-cut section between the xiphoid process and umbilicus. To measure the thickness of EAT, two-dimensional transthoracic echocardiography was performed on each subject to capture images in standard parasternal and minor axis views. Perpendicular to the aortic annulus for the parasternal long-axis view, perpendicular to the interventricular septum at the mid-chordal and the tip of the papillary muscle level for the parasternal short-axis view was used to assess the maximum thickness of EAT at the end-systole. The thickness of EAT was defined based on the average of three cardiac cycles for each echocardiographic view.
Measurement of heart rate variabilityThe primary outcome of our study was HRV measured using a 12-lead Holter system (Marquette, USA) over a 24-hour period. Participants were instructed to follow their normal daily activities, avoiding caffeine, alcohol, cigarette and heavy activity during the recording time. Both frequency-domain and time-domain indices were adopted to assess HRV. Frequency-domain indices included the low frequency (LF) band power, high frequency (HF) band power and ratio of LF and HF (LF/HF). LF and LF/HF reflect sympathetic activity whereas the HF and time-domain HRV indices reflect parasympathetic activity and the whole autonomic function. Time-domain HRV measures included standard deviation (SD) of all normal to normal intervals (SDNN, ms), SD deviation of the average sequential 5-minute normal to normal interval means (SDANN, ms), the mean value of the SD of all the normal to normal intervals in every 5-minute interval within 24 h (SDNN index), the root mean square of successive differences (rMSSD, ms) and the number of pairs of adjacent normal to normal intervals differing by > 50 ms in the entire recording divided by the total number of NN intervals (pNN50, %).
Measurements of covariatesFactors known to be associated with diabetes, adipose metabolic and HRV were included in the analyses as covariates, including age, gender, body mass index (BMI), systolic blood pressure (SBP), triglyceride (TG), total cholesterol (TC), lifestyle (smoking and alcohol consumption), self-reported comorbidity (hypertension, coronary artery disease), duration of diabetes and medical history. Other laboratories examination including high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting plasma glucose (FPG), hemoglobin, uric acid (UA), estimated glomerular filtration rate (eGFR) and glycated hemoglobin (HbA1c) were analyzed for both T2DM and non-diabetic group by Hitachi 7180 chemical analyzer. Triglyceride-glucose (TyG) index was calculated as (fasting TG × fasting plasma glucose/2).
Statistical analysisDescriptive statistics were presented as mean ± SD for continuous variables or as numbers and percentages for categorical variables to compare baseline characteristics between participants with T2DM and those without diabetes.
First, the baseline data, HRV indices and thickness of adipose tissues were compared between T2DM and non-diabetes groups. Categorical variables were compared using χ2 test, while continuous data were assessed using the parametric t test or non-parametric Mann–Whitney U test.
Next, Spearman rank correlation tests were used to examine the relationships between the thickness of various adipose tissue and parameters of HRV. Univariate linear regression was performed to assess the unadjusted relationships between various adipose tissue and HRV. Two multivariate linear regression models were performed to adjust for confounding factors. Model 1 was adjusted for age and gender. Model 2 was additionally adjusted for HbA1c, FPG, BMI, TG, TC, smoke, alcohol, hypoglycemic therapy (OAD, Insulin, OAD + insulin), medications (ACEI/ARB, statin, antiplatelet), hypertension, CAD, and diabetic peripheral neuropathy, as well as the duration of diabetes mellitus.
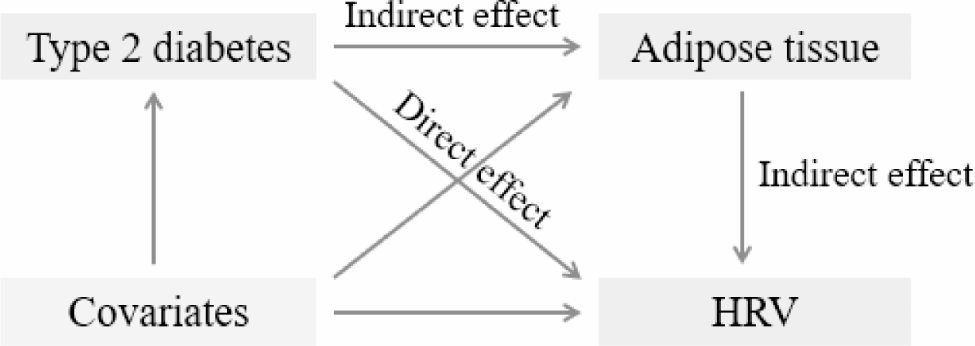
Then, adipose tissues which simultaneously associated with both T2DM and the HRV indices in linear regression model 2 were included in mediation analysis. The shortlisted adipose tissues in mediation analyses recognized as mediators, with T2DM as the independent variable and HRV indices as the dependent variable. Age, gender, HbA1c, FPG, BMI, TG, TC, smoke, alcohol, hypoglycemic therapy (OAD, Insulin, OAD + insulin), medications (ACEI/ARB, statin, antiplatelet), hypertension, CAD, duration of diabetes mellitus were treated as covariates in each model. Figure 1 was employed to enhance the visualization of our statistical approach. A parameter regression approach was used to estimate the total effect, the indirect effect and direct effect of T2DM on HRV. The direct effect is the effect of T2DM (exposure) on HRV (outcome) after adjusting for adipose tissue (mediator). The proportion of mediation represents the fraction of the association of T2DM explained by its association with changes in adipose tissue thickness. A significant disparity in these models would imply that adipose tissue introduces supplementary variability in HRV beyond the impact of T2DM alone. To quantify the magnitude of mediation, the study estimated the proportion of the association mediated by adipose tissue (indirect effect/[direct effect + indirect effect] if the indirect effect is significant.
Fig. 1
Mediating pathway of the association of type 2 diabetes mellitus (T2DM) with heart rate variability (HRV)
In addition, we constructed a latent variable, HRV burden, to further evaluate overall HRV. Latent variables are variables that cannot be observed directly and need to be measured indirectly by a set of observed variables. Confirmatory factor analysis (also known as a measurement model), which enables exploration of whether a hypothesized latent factor model fits the collected data, was used to evaluate the reliability and validity of latent structure mode (which hence for HRV burden in our research) [15]. Structural validity is mainly used to test the fitness of the overall model, assessing the agreement between the model parameters derived from our data and the parameter values of the theoretical model. Reliability represents the internal stability and aggregation of the model, with high reliability means that the measurement variables under the same potential variable are highly correlated. The latent variable was then incorporated into another series of multiple regressions, modeled within structural equation modeling framework adjusted for covariates to estimate the mediation effect of T2DM on HRV burden via adipose tissues.
Planned additional sensitivity analysis were performed to examine the robustness of study results. First, gender-stratified mediation was estimated. Second, to account for protopathic bias, the analyses excluded all participants diagnosed with T2DM in the 12 months prior to adipose tissues measurement. Third, to mitigate the influence of cardiovascular disease on adipose tissues, individuals diagnosed with coronary artery disease and hypertension were also excluded.
The significance of mediation effect was assessed by computation of bootstrap confidence intervals (CIs). Bootstrapping entailed multiple rounds of sampling from the dataset to gauge the indirect effect in each resampled dataset. Through 5000 iterations of this procedure, an empirical approximation of the sampling distribution for the quantified indirect effect of the independent variable on the dependent variable, mediated by each potential mediator, was established and then utilized to generate CIs for the indirect effect. All reported β’s presented are standardized regression coefficients and were thus directly comparable. All P values were 2-tailed, and values less than 0.05 were considered statistically significant. Analyses were performed using SPSS version 24.0 software for Windows (SPPS Inc, Chicago, IL, USA) and Lavaan packages in R software (version 4.3.0). This mediation analysis was reported in accordance with the Guidelines for Reporting Mediation Analyses in Randomized Trials and Observational Studies (AGReMA) statement [16].
Comments (0)