
Remember me

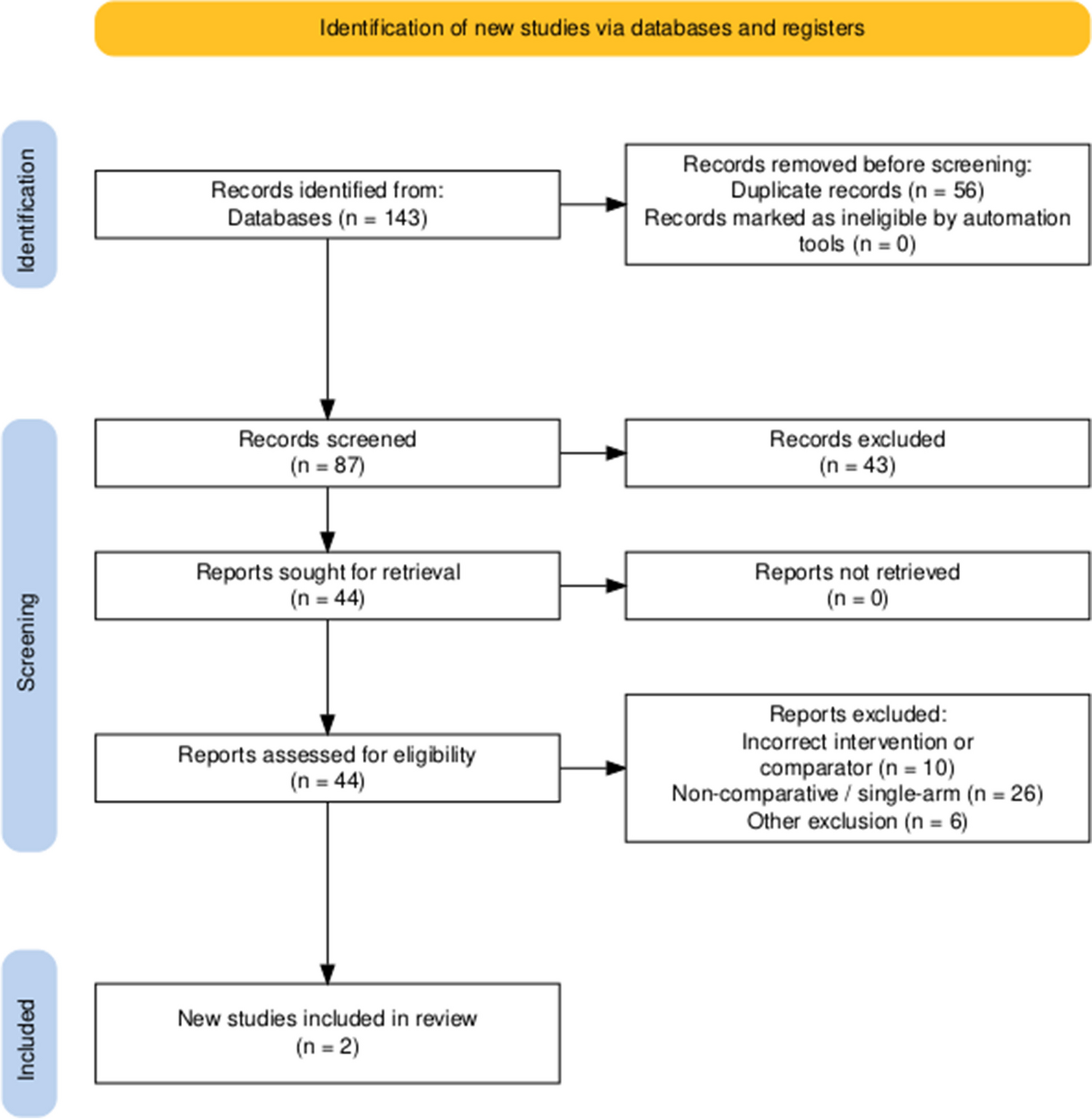

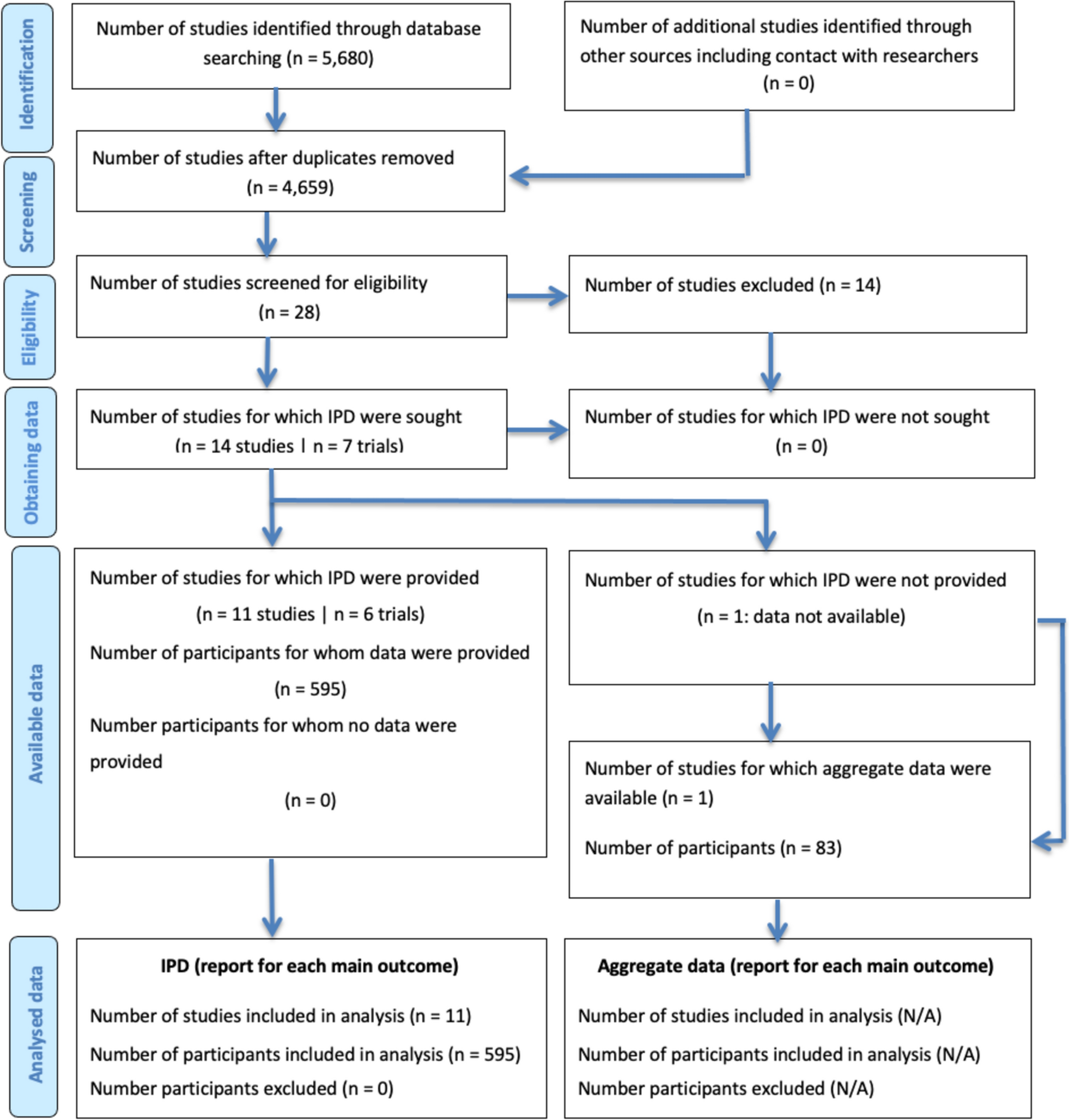

After the initial screening of 569 articles, 19 [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31] were included in this systematic review (PRIMSA flow chart, Fig. 1). The studies were published between 2005 and 2022 and were based in the USA (n = 7), Sweden (n = 3), Norway (n = 3), Germany (n = 2), Finland (n = 1), France (n = 1), Italy (n = 1), and the Netherlands (n = 1). All studies were retrospective cohort studies.
Fig. 1
Overall, 2042 patients were included in the review, with a median age of 38.2 (range, 23.1–46.4) years and a female-to-male ratio of 1.17:1. KP was performed after failed IPAA in 322 (15.8%) patients. The number of patients operated on per study year ranged from 0.96 to 22.7, with a mean of 5.2 patients per year (Table 1). In 16 studies, the indication for a KP was IBD, whereas in 10 studies it was FAP, and in seven studies, functional disorders including colonic inertia and Hirschsprung’s disease were the indications for KP (Table 2).
Table 1 Characteristics of patients and studiesTable 2 Indications for Kock pouchTotal and individual complicationsThe weighted mean prevalence of total complications was 60.4% (95% CI: 46.1–74.7%, I2 = 98%; Fig. 2). The weighted mean prevalence of nipple valve complications was 40.5% (95% CI: 24.7–56.2%, I2 = 97%), difficult intubation 13.1% (9.7–16.5%, I2 = 43.8%), pouch leak/fistula 16.8% (95% CI: 10.9–22.7%, I2 = 93.7%), pouchitis 13% (95% CI: 6.6–19.4%, I2 = 93.8%), abscess 11.9% (95% CI: 0.2–23.6%, I2 = 81.1%), hernia 8.6% (95% CI: 4.3–13%, I2 = 88.1%), and short-bowel syndrome 2.5% (95% CI: 0.3–4.7%, I2 = 0; Fig. 3). The total and individual complications reported in each study are summarized in Table 3.
Fig. 2
Forest plot depicting the weighted mean prevalence of total complications after Kock pouch
Fig. 3
Forest plot depicting the weighted mean prevalence of nipple valve complications, difficult intubation, pouchitis, and leak or fistula after Kock pouch
Table 3 Complications after Kock pouchSubgroup analysesThe pooled complication prevalence in the studies published after 2010 was slightly lower than that in the studies published before 2010 [58.1% (95% CI: 45.1–71.1%) versus 59.9% (95% CI: 41–78.7%)]. Studies with follow-up > 10 years (n = 12) had a pooled complication prevalence of 54.6% (95% CI: 43–66.2%) compared with 71% (95% CI: 55–87%) in studies with follow-up < 10 years. Studies conducted in the USA had a mean complication prevalence of 89.9% (95% CI: 81.1–98.5%), higher than that in studies conducted in European countries [52.2% (95% CI: 41.5–62.9%)]. After exclusion of the two largest studies [14, 27], the weighted mean rate of total complications was 60.8% (95% CI: 45.9–75.7%). The pooled prevalence of complications in studies with > 5 patients per year was 59.6% (95% CI: 29.6–89.6%). Studies (n = 6) that mainly included patients with IBD had a pooled complications prevalence of 48.5% (95% CI: 35.4–61.6%), whereas the pooled complication prevalence in the studies that included patients with slow-transit constipation, inertia, or other motility disorders was higher, at 73.8% (9%CI: 49.1–98.5). A leave-one-out meta-analysis did not reveal a significant change in the pooled prevalence of complications on the exclusion of each study (Supplementary Fig. 1).
Meta-regression analysisFactors associated with higher complications were increased BMI (SE: 0.992, p < 0.001), previous IPAA (SE: 0.008, p = 0.002), and country of the study (SE: − 0.334, p = 0.002). Age (SE: − 0.004, p = 0.656), male sex (SE: − 0.0001, p = 0.528), and study year (SE: − 0.043, p = 0.722) were not significantly associated with complications after KP creation.
Pouch revision and failureThe median follow-up period was 12.7 (range, 3.7–31) years. The weighted mean prevalence of pouch revision was 46.6% (95% CI: 38.5–54.7%, I2 = 80.8%), and of pouch failure was 12.9% (95% CI: 9.3–16.4%, I2 = 80.7%; Fig. 4). A summary of failure and revision prevalence in each study is shown in Table 4.
Fig. 4
Forest plot depicting the weighted mean prevalence of Kock pouch revision and failure
Table 4 Revision and failure of Kock pouchSubgroup analysesThe weighted mean pouch failure prevalence in the studies published after 2010 (13.2%; 95% CI: 8.2–18.1%) was higher than that in the studies published before 2010 (10.4%; 95% CI: 6.2–14.6%). Studies with a follow-up of > 10 years (n = 12) had a mean failure rate of 14.4% (95% CI: 10.6–18.2%) compared with 5.9% (95% CI: 2.8–9%) in studies with a follow-up of < 10 years. Studies conducted in the USA had a mean failure prevalence of 12.6% (95% CI: 6.2–18.9%), comparable to studies conducted in Europe (11.1%; 95% CI: 7.5–14.7%). After exclusion of the two largest studies [14, 27], the weighted mean prevalence of pouch failure was 11.6% (95% CI: 7.8–15.4%) and of pouch revision was 46.7% (95% CI: 39.9–53.5%). The pooled prevalence of failure and revision in studies that included > 5 patients per year was 11.5% (95% CI: 7.3–15.7%) and 48% (95% CI: 29.7–66.3%), respectively. A leave-one-out meta-analysis did not reveal a significant change in the pooled prevalence of failure and revision on the exclusion of each study (Supplementary Fig. 1).
A summary of the pooled prevalence of pouch complications and failure in the sensitivity analyses is shown in Fig. 5.
Fig. 5
Pooled prevalence of pouch complications and failure in the sensitivity analyses
Meta-regression analysisNone of the examined variables were associated with pouch failure [age (SE: − 0.006, p = 0.222), male sex (SE: − 0.0001, p = 0.778), previous IPAA (SE: − 0.0001, p = 0.710), study year (SE: 0.020, p = 0.567), country of the study (SE: − 0.082, p = 0.114), complications (SE: − 0.001, p = 0.971), nipple valve complications (SE: 0.001, p = 0.473), pouchitis (SE: − 0.006, p = 0.164), and pouch leak/fistula (SE: − 0.0001, = 0.795)].
Risk of bias and certainty of evidenceA total of 12 studies had some concern of bias, and 7 were at high risk of bias (Appendix Table 1). There was no evidence of publication bias for complications, pouch revision, and failure as shown by the insignificant p-values of the Egger’s regression test (p = 0.381, p = 0.571, and p = 0.388, respectively; Supplementary Fig. 2). Based on the GRADE assessment, the main outcomes of this review had very low certainty of evidence because of the high risk of bias, inconsistency, and imprecision as shown in Appendix Table 2.
Comments (0)