The incidence of TF observed in this study is considerable, with one in every six female outpatients with uUTI experiencing TF to empirically prescribed oral antibiotics. To our knowledge, this study provides the most current and comprehensive estimate of the incidence of TF to empirically prescribed oral antibiotics in female outpatients with uUTI and is the first to shed light on the risk factors of TF in the US. As such, our findings advance the understanding of the risk of TF with current uUTI antibiotic treatment options and highlight the sub-populations at elevated risk for TF, among whom urinalysis may enhance treatment decision-making and mitigate the risk of antibiotic overprescribing in clinical practice.15
The incidence of TF observed in this study (16.7%) approaches the upper range of TF rates previously reported in observational studies of female patients with uUTI.9,23 Indeed, Franklin et al. (2023)11 observed TF in 12.3% of empirically treated female outpatients with uUTI in the US when using the same definition of TF as in this study. The lower incidence of TF reported by Franklin et al. may be driven by the use of administrative claims data, which provide insights into medications dispensed. As the EHR data utilized in this study accounts for antibiotic prescriptions that would not be captured in administrative claims data, it may provide a more complete estimate of the incidence of TF. EHR data provide insights into medications prescribed and therefore, prescriptions of a new or repeat antibiotic treatment are likely indicative of a lack of initial treatment response from the clinician perspective. Moreover, the incidence of TF in this study aligns with other claims-based studies of UTI. For example, Butler et al. (2021) reported a crude TF risk (defined by antibiotic prescription switch/repeat) among premenopausal women with uUTI of 13.6%.5 The incidence of TF in this study was 14.0% when defined by a new or repeat oral antibiotic prescription, consistent with Butler et al. despite their inclusion of a younger population (median age: 29–32 years) and use of administrative claims data. Therefore, the incidence of TF in this study is corroborated by prior literature, suggesting that our definition of TF is a reliable approach to estimating this outcome in EHR data, and underscores the limitations of current oral antibiotics in the management of uUTI.
One of the strongest risk factors of TF in this study was prior antibiotic prescriptions. Notably, ≥ 3 prior antibiotic prescriptions within ≤ 12 months of a uUTI imposed a 60% higher risk of empiric TF than no prior antibiotic prescriptions. Similarly, having one prior UTI within six months or two within ≤ 12 months of a uUTI imposed a 12% higher risk of TF than no prior UTIs. These findings highlight the impact of past infections, specifically those that require antibiotic prescriptions or that are UTI-related, on subsequent TF and corroborate guideline recommendations for obtaining a urine culture and susceptibility test in patients with recurrent uUTI.24,25 In other studies, prior antibiotic exposure and UTI episodes have been identified as important risk factors for AMR.26,27,28 Although prior antibiotic non-susceptibility was not identified as a risk factor of TF in this study, future research may extend our work by assessing the individual association between non-susceptibility to the empirically prescribed oral antibiotic and subsequent TF in this population. Nevertheless, our findings highlight an implicit association between AMR and TF that provides support for the consideration of local AMR prevalence8 to optimally treat uUTI.
Across oral antibiotics prescribed, the incidence of TF was varied and fosfomycin was associated with the highest risk of TF compared to NTF. In a RCT, treatment with fosfomycin was similarly observed to increase the likelihood of clinical TF by 2.35 times.14 Fosfomycin is an infrequently used uUTI treatment in the US due to efficacy concerns and high cost.29 Accordingly, few patients were prescribed fosfomycin in the present study (< 5%), which may suggest a differential risk profile with respect to TF when other first-line agents are not considered. Prescriptions of SXT and β-lactams were also identified as risk factors of TF relative to NTF. The higher risk of TF associated with β-lactams is not unexpected, given its placement as a second-line agent due to adverse outcome concerns.8,25 The higher risk of TF associated with SXT may be driven by increasing rates of non-susceptibility to SXT. Between 2011 and 2019, the prevalence of non-susceptibility to SXT among uropathogenic Escherichia coli (E. coli) in the US was consistently ≥ 25%.30 SXT is not recommended by IDSA guidelines as first-line therapy when community non-susceptibility rates are ≥ 20%.8 Thus, SXT therapy in this study may have been discordant with treatment guidelines.31 These findings suggest that the utility of some first-line therapies in the treatment of uUTI may be limited and future research investigating the impact of community non-susceptibility rates on risk of TF are warranted.
Location of care, including healthcare setting and geographic region, was significantly associated with a higher risk of TF in uUTI. An index uUTI diagnosis in the ED increased the risk of TF by nearly 50% versus a diagnosis in the office/clinic. Previous research suggests that inappropriate antibiotic prescribing may contribute to higher risk of TF in the ED than in the office/clinic.32 The challenges of managing UTIs in EDs, including limited medical history, limited longitudinal follow-up, and lack of culture and susceptibility results, may further contribute to increased TF.33 Residence in the South (versus MidWest) was associated with higher risk of TF, which may be driven by higher rates of antibiotic prescribing and inferior antibiotic stewardship practices in the South than other US regions.34 Poor empiric treatment practices are associated with clinical failure, including increased risk of AMR and the need for alternative antibiotics.35 A retrospective US study of E. coli isolates from female outpatients with uUTI observed that AMR rates are highest in Southern US regions.30 The South has also been associated with the highest risk of non-susceptibility to NTF, SXT and fluoroquinolones, when controlling for confounding factors.28 Careful consideration of the location of care in empiric treatment decision-making, together with effective antibiotic therapies, may help to reduce inappropriate prescribing in this population.
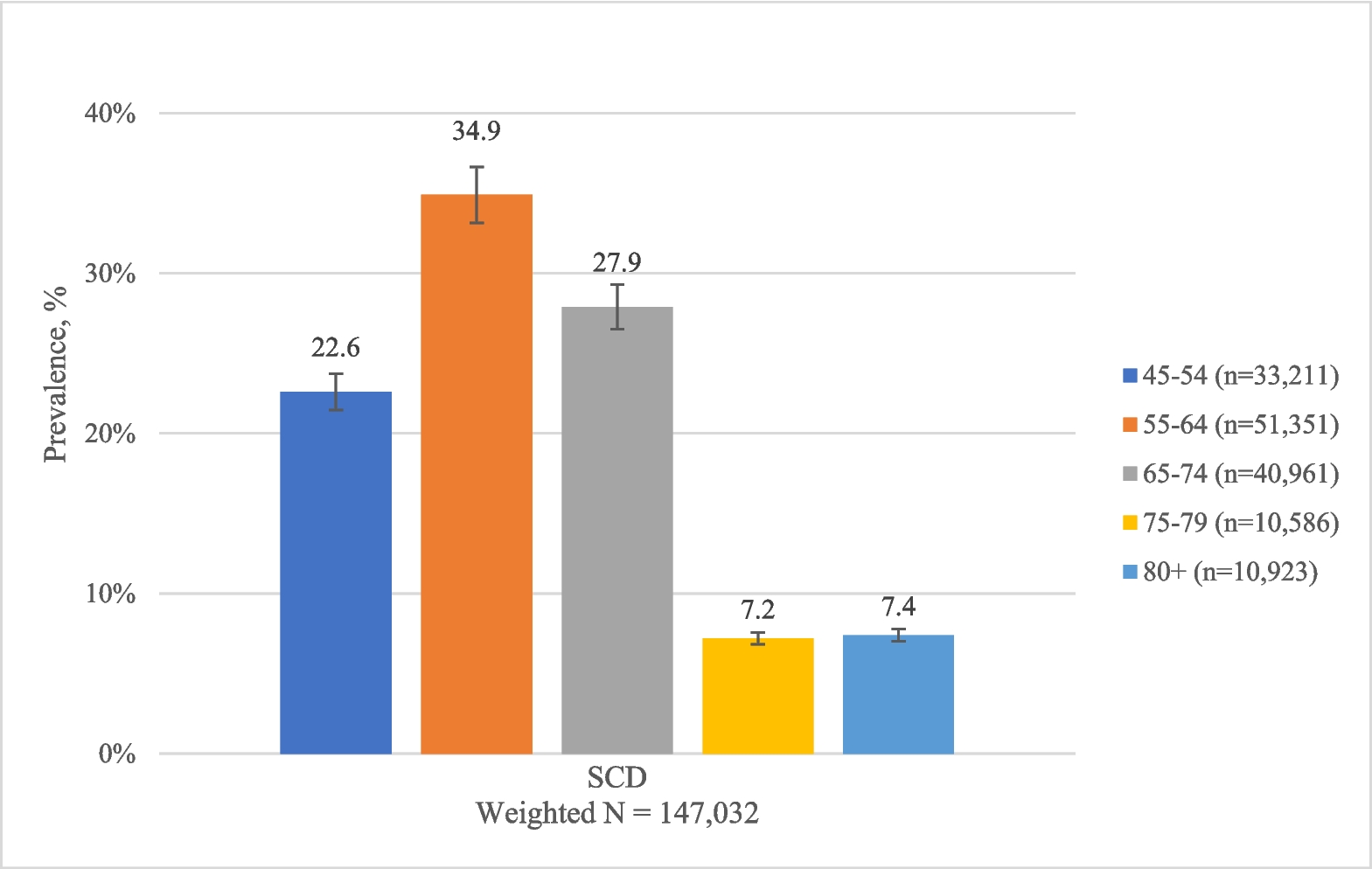
UTIs are one of the most commonly diagnosed infections in older women, due in part to their compromised immune response, vaginal atrophy, hormonal changes and multiple comorbidities.36,37 UTIs are the most common indication for antibiotic prescriptions in this population, with 40–75% of antibiotic use considered inappropriate.37 Older age was significantly associated with a higher risk of TF in this study, with a 27% and 35% higher risk in female outpatients aged 65–74 years and ≥ 75 years, respectively, than those aged 12–17 years. In prior literature, the estimated probability of TF in UTI increased by 2% for each decade after 60 years of age.6,37 As older patients with uUTI are at higher risk of TF to empirically prescribed oral antibiotics, it is imperative that effective agents are initiated early in the elderly population.
Findings from this study should be interpreted considering some limitations. Neither the study population nor the definition of TF used in this study required a urinalysis- or culture-proven UTI. This approach may have resulted in the inclusion of misdiagnosed patients in the study and overestimation of TF. However, as urine cultures are not systematically collected in real-world clinical practice, nor specifically recommended for the management of non-recurrent uUTI8 our findings may be more generalizable to the broader empirically treated uUTI population. A patient may have received an oral/IV antibiotic for a non-uUTI related condition, which may overestimate TF. Nevertheless, findings from the sensitivity analysis suggest that the incidence of TF was consistent when accounting for other infections and possible prophylactic use due to surgeries/procedures. Despite exclusionary efforts, patients with cUTI may be present in the study population due to misclassification. While EHR data provide insights into medications prescribed, they do not indicate if the antibiotic prescription was dispensed and consumed by the patient as prescribed. This limitation may lead to overestimation of TF if patients were noncompliant with their initial empirically prescribed oral antibiotic treatment. Nonetheless, despite this known limitation of EHR data in retrospective, observational studies, the incidence of TF reported in this study largely aligns with published evidence from claims-based studies. Lastly, the requirement of ≥ 12 months of Optum EHR activity post-index may have introduced survival bias. However, given that uUTIs are not associated with high mortality rates,38 minimal bias is expected to be introduced by this criterion.
Despite these limitations, key strengths of this study include its reporting of the most current estimate of TF to empirically prescribed oral antibiotics in a large patient population. Moreover, this study is the first to identify risk factors for TF in empirically prescribed female outpatients with uUTI in the US. The dataset utilized was an ideal data source given the large and rich clinical data from which candidate risk factors for TF were derived. The list of candidate risk factors identified in this study were further informed by input from a urology expert.



Comments (0)