This retrospective cohort study was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee and followed the Declaration of Helsinki.
The data source was described previously [3]. Briefly, we used the Clinical Data Analysis and Reporting System (CDARS), a population-based health records database of all patients who attend public hospitals/clinics in Hong Kong. CDARS is linked to the governmental death registry. Both have been used extensively in research [4].
Patients aged ≥18 years old with prostate cancer who received enzalutamide or abiraterone atop androgen deprivation therapy (gonadotrophin-releasing hormone agonists and antagonists, and bilateral orchidectomy) in Hong Kong between 1/12/1999 and 31/3/2021 were included. The following patients were excluded: (a) received both drugs simultaneously/separately, (b) with abiraterone initiated without glucocorticoids, (c) with prior stroke, myocardial infarction (MI), or heart failure (HF), (d) with enzalutamide initiated with any glucocorticoid, and (e) with abiraterone initiated with any glucocorticoid regimen that is not prednisolone/prednisone 5 mg daily, 5 mg twice daily, nor 10 mg daily. Exclusion criteria (d) and (e) were added to the ones used in our prior study [3] as these prescriptions were not standard for enzalutamide/abiraterone regimens and were likely for other indications.
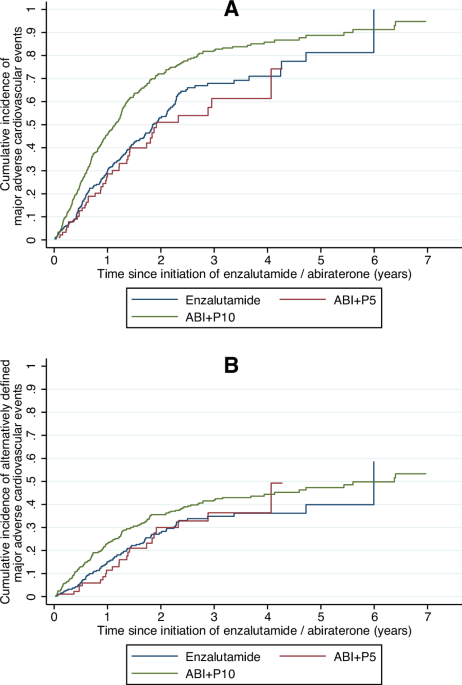
Patients were followed up from enzalutamide/abiraterone initiation (“index”) until 30/9/2021 or death, whichever earlier. Per our prior study [3], the primary outcome was MACE, a composite of all-cause mortality, MI, HF, and stroke. As some studies suggested efficacy differences between enzalutamide and abiraterone [5], we included an alternatively defined MACE (MACEalternative) as a secondary outcome, defined as a composite of non-PCa-related mortality, MI, HF, and stroke. Outcome and covariate ascertainment have been described in our prior study [3].
The exposure groups (regimen at the start of follow-up) were enzalutamide, abiraterone with 5 mg daily total of prednisolone/prednisone (ABI + P5), and abiraterone with 10 mg daily total of prednisolone/prednisone (ABI + P10).
The association between exposure and the risk of MACE was modeled using multivariable Cox regression, while that for the cumulative incidence of MACEalternative was modelled using multivariable Fine-Gray competing risk regression with PCa-related mortality as the competing event. All regressions were adjusted for pre-specified covariates as listed in Supplementary Table 1. Cumulative glucocorticoid dose at index (CGD) was analyzed as log-transformed prednisolone-equivalent dose (as ln(1 + [cumulative glucocorticoid dose]) to allow transformation of zeros) [6].
In a post-hoc sensitivity analysis, only enzalutamide was compared against ABI + P10, as these groups were more similar in PCa treatment-related covariates (e.g. pre-index ADT duration).
Two-sided p < 0.05 were considered statistically significant. All analyses were performed using Stata v16.1 (StataCorp LLC, United States).


Comments (0)