This study of VHA data over a 15-year period demonstrates that most patients with rapid PSADT underwent secondary treatment within 1 year after BCR, and over 2 years for patients with less rapid PSADT. Intriguingly, outcomes among patients with rapid PSADT compared favorably to prior studies of all BCR patients treated with ADT delayed until metastasis [3]. Further study will determine whether this reflects the benefits of early aggressive treatment of high-risk BCR or improved outcomes over time.
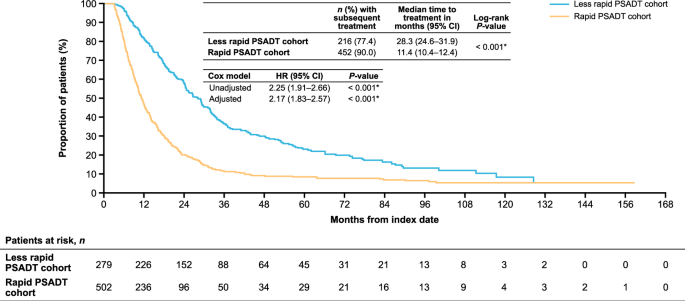
Natural history studies of patients with ADT delayed until metastasis show the important prognostic value of PSADT [3, 4]. Importantly, patients with rapid PSADT had worse time to metastasis, MFS, and OS compared with patients who had less rapid PSADT. Our results mirror these findings but extend the results to those who largely received early aggressive secondary treatment for BCR. Our exploratory analyses found that patients with PSADT ≤3 months and PSADT >3 to ≤9 months had worse MFS and patients with PSADT ≤3 months had worse OS than patients with PSADT >12 to ≤15 months. These results further support the prognostic role of PSADT, regardless of whether patients receive early or delayed ADT.
The median time to metastasis for patients with rapid PSADT was 102 months (8.5 years). Similarly, there were 8 years until metastatic spread in patients with BCR in the Johns Hopkins analyses, none of whom received secondary hormonal therapy prior to metastasis [3]. Importantly, the Johns Hopkins analysis included all BCR patients, not just those who were high-risk. For those with PSADT <10 months in the Johns Hopkins data, median time to metastatic disease was around 5 years [3]. As >80% of our cohort underwent prior surgery, it is noteworthy that we defined BCR as a PSA value of ≥1 ng/mL, which potentially excludes patients for whom salvage therapy is a treatment option. This cutoff is higher than that used in prior Johns Hopkins data, where BCR was defined as a PSA value of ≥0.2 ng/mL [3]. As such, despite being further along in their BCR journey, our patients had better outcomes. One possible explanation is that early secondary treatment of high-risk BCR improves outcomes. Alternatively, as new therapies are introduced and stage migration continues, overall outcomes in prostate cancer are improving [14]. Given the retrospective nature of our study, we cannot imply cause and effect, and comparison across studies is challenging. More studies are needed to understand the reasons for better outcomes in more contemporary patients treated with aggressive, early, secondary therapy.
While comparing time to metastatic disease is important, it is possible that many of the metastases that developed in our study were castration-resistant at the time of metastases versus the Johns Hopkins analysis where they were castration-sensitive. Therefore, it is important to also compare OS. The median OS in patients with rapid PSADT in our study (120.5 months [10.0 years]) aligned with previous results in patients with a PSADT of 3 to 8.9 months from longer term follow-up from Johns Hopkins [4]. However, our cohort was older than the Johns Hopkins cohort (median age 66.4 and 61.5 years, respectively; see Supplementary Fig. S4 for general male-specific mortality by age) and the Johns Hopkins PSADT 3 to 8.9 month group did not include patients with PSADT <3 months, unlike our PSADT ≤9 month group which included these very high-risk patients. In contrast, patients with less rapid PSADT in our series had a median OS of 140.5 months (11.7 years), whereas median OS was not reached at 15 years in the Johns Hopkins data for patients with a PSADT of 9 to 14.9 months. Notably, the risk of prostate cancer death in patients with slower PSADT is much lower than those with more rapid PSADT and, therefore, it is likely that many deaths in our study were not related to prostate cancer. As such, the worse outcomes in our patients with less rapid PSADT suggest that our cohort had poorer overall health versus the Johns Hopkins cohort. When taken together with the older age, inclusion of a very high-risk group (PSADT < 3 months), and higher PSA levels at BCR within our cohort, this further emphasizes the potential clinical significance of the similar median OS between patients with rapid PSADT in our study and historical Johns Hopkins data [4]. Again, whether this reflects the benefit of early ADT in patients with high-risk nmCSPC and BCR or temporal changes in the natural history over time requires investigation in prospective randomized trials.
Several studies investigated the clinical benefit of adding chemotherapy or NHT to ADT in patients with high-risk BCR. TAX3503 did not demonstrate a meaningful benefit of adding docetaxel to ADT in patients with high-risk BCR [15]. One possible interpretation of our data is that early ADT is beneficial; if true, it is possible that intensified ADT may provide further benefit. Indeed, EMBARK demonstrated that enzalutamide, with or without ADT, improved MFS and the time to first use of new antineoplastic therapy compared with placebo plus ADT in patients with high-risk nmCSPC and BCR (PSADT ≤9 months) following definitive therapy (RP or radiotherapy) [13]. Additionally, ADT plus apalutamide, with or without abiraterone, prolonged biochemical progression-free survival in patients with high-risk BCR following RP in AFT-19 [16]. Follow-up is ongoing to determine longer-term outcomes, including OS in EMBARK, and MFS and time to castration resistance in AFT-19.
Our findings may not be generalizable to populations other than patients from the VHA and are limited by possible incorrect diagnosis coding. Furthermore, care occurring outside the VHA may not have been captured, which could have led to misclassifications of disease states or treatments. Additionally, a prescription may not signify that the medication was taken as prescribed. As we excluded patients with ADT at any point prior to index to ensure that PSADT calculations were free from any lingering effects of ADT, patients who received standard-of-care ADT plus radiotherapy were not included. As such, RP patients are likely over-represented in our cohort, though this permits closer comparisons to prior Johns Hopkins studies that included only RP patients. Our definition of BCR was more restrictive than the Johns Hopkins studies, which defined BCR as a PSA value of ≥0.2 ng/mL. Finally, our OS estimates also reflect the availability of life-prolonging therapies for metastatic disease that were not available during the historical Johns Hopkins analyses.
In summary, patients with nmCSPC, BCR, and rapid PSADT following definitive therapy in the VHA had shorter time to first systemic antineoplastic therapy and worse outcomes for time to metastasis, MFS, and OS, than patients with less rapid PSADT. Patients with rapid PSADT from the VHA, who were heavily treated with secondary treatment, older, had potentially poorer health, and had higher PSA levels at BCR than patients from the historical Johns Hopkins data, had similar outcomes to patients who did not receive aggressive secondary treatment. This suggests either a potential benefit of aggressive, early treatment of patients with rapid PSADT after BCR and/or temporal improvements in outcomes over time. Further study exploring the relationship between short PSADT and lineage plasticity may be warranted.


Comments (0)