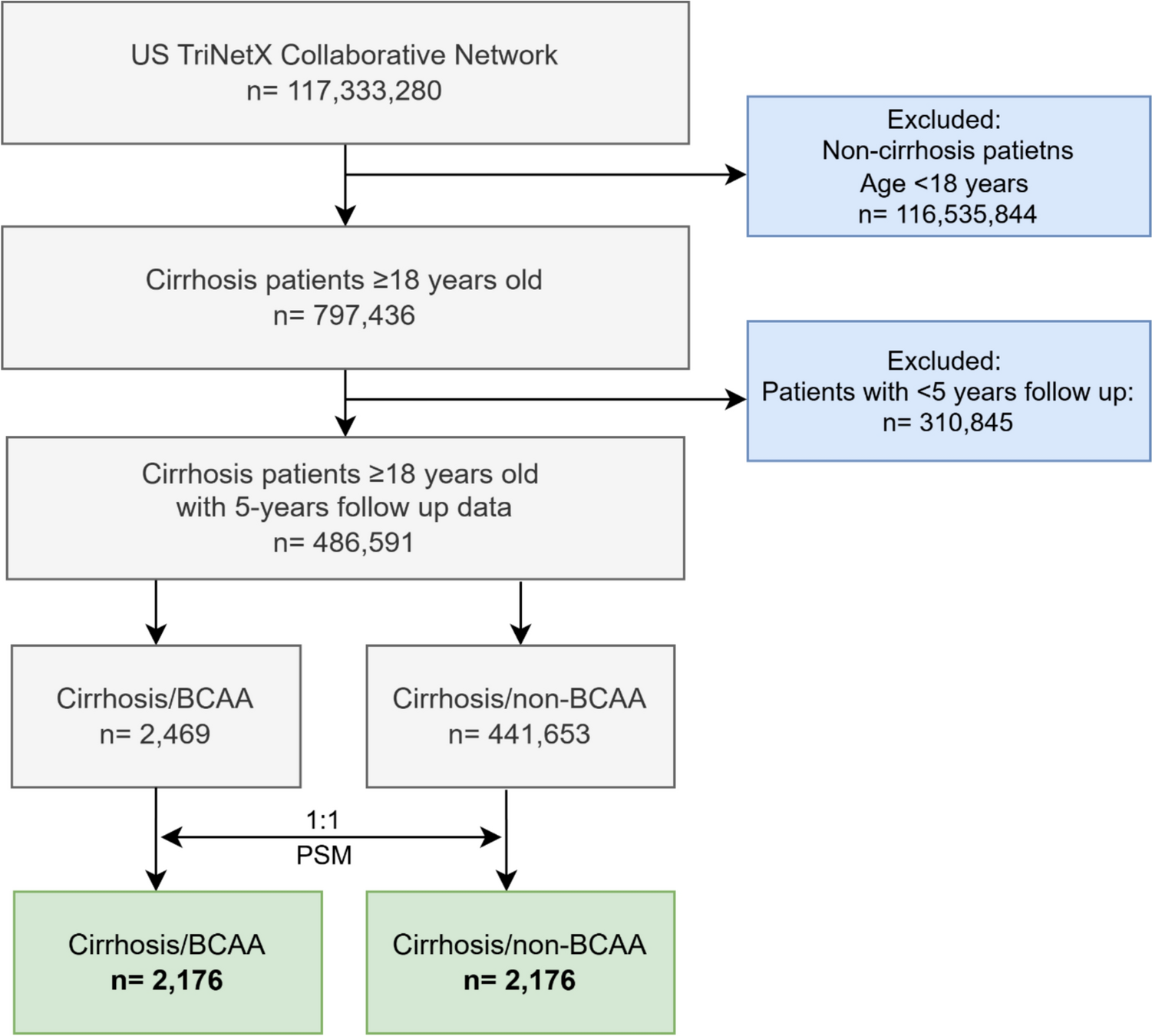
This is a retrospective study of patients undergoing WGTS for clinical evaluation for symptomatic constipation from 12/30/2018 to 10/14/2023 at Temple University Hospital. The patient’s gastroenterologist determined if a patient should undergo WGTS. Patients were excluded if they were less than 18 years old, pregnant or had prior GI surgeries.
Data Collection
The data retrieved for this study included (1) the WGTS studies and reports stored electronically in Sectra PACS. The following WGTS parameters were collected: Percent gastric retention at 0, 0.5, 1, 2, 3, 4 h, gastric emptying T-1/2, small bowel transit, geometric center of colon activity on the second, third, and fourth days of the test. (2) the questionnaires that patients filled out prior to WGTS which includes the PAGI-SYM questionnaire which quantitates symptoms and also a demographic, medical history questionnaire; and (3) EPIC, the electronic medical record (EMR) for Temple University Hospital was used to verify and obtain incomplete survey data for medical disorders, prior surgeries, other test results, and current medications. All data was entered into a password protected Excel spreadsheet. We recorded the following specific variables: age, gender, weight, height, medical disorders (including diabetes, SLE, scleroderma, Parkinson’s disease, and GERD) and prior surgeries (especially GI surgeries, and presence of jejunostomy tube, gastrostomy tube, ileostomy, colostomy, and gastric stimulator). Medication use (including use of prokinetics, opiates, anticholinergic agents, insulin, oral hypoglycemic agents) was recorded as well. For the WGTS test, patients were instructed to stop any prokinetic agents or opiate analgesics that they were taking three days prior to the test. In addition to assessing the medical records and reviewing medication dispense reports, patients completed a survey that specifically asked about their use of opiates and other medications affecting GI motility. Patients who reported using medications that affect motility were asked to confirm that they had not taken these medications within 48 h prior to the WGTS study. With the data, we calculated the frequency of different types of colon transit test patterns as defined below.
WGTS Imaging Protocol and Image Analysis
Patients underwent WGTS utilizing the currently established standard egg sandwich meal radiolabeled with Tc-99m SC (short half-life for radioactive decay and short imaging time) and water radiolabeled with 111In-DTPA (longer half-life for radioactive decay and more prolonged imaging up to 72 h) as part of a standard solid–liquid gastric emptying meal [1]. Gastric emptying was assessed for the first 4 h of the study. Small bowel transit analysis utilized the liquid water phase for the next two hours. Small bowel transit was considered delayed if less than 40% of the meal accumulated in the TI/CAC area at 6 h [1]. Colon transit images were acquired at 24, 48, and 72 h after meal ingestion using the In-111 which was administered in water. To calculate the colonic geometric center, the colon was divided into 7 anatomic regions, each of which has a numeric value: cecum–ascending colon (1), hepatic flexure (2), transverse colon (3), splenic flexure (4), descending colon (5), rectosigmoid colon (6), and, by calculation, excreted stool (7). The geometric center is the weighted average of the counts in each region. The normal mean values (± SD) for geometric center are 4.6 ± 1.5 at 24 h, 6.1 ± 1.0 at 48 h, and 6.6 ± 0.19 at 72 h which were determined from 28 normal volunteers (18 men and 10 women, mean age 26.2 yr (range 18–45 yr) [1, 3].
Colonic inertia (CI) is defined by failure of the radiotracer to progress beyond the splenic flexure, with a geometric center of less than 4.1 at 48, and 72 h. Generalized slow colonic transit (GSCT) is defined as diffuse retention of radiotracer throughout all colonic segments, with a geometric center of less than 4.1 (proximal to the splenic flexure) at 48 h and between 4.1 and 6.2 at 72 h. Functional rectosigmoid obstruction (FRSO) is defined as initially sufficient colonic transit into the rectosigmoid colon followed by localized retention [1]. FRSO has a geometric center of more than 4.1 at 48 h and less than 6.2 at 72 h [1, 8].
Upper GI Tract Abnormalities
We determined how often patients with each colonic transit pattern in our study had upper GI tract abnormalities of delayed GE and delayed SBT. As described by Dinning et al., the following definitions were used: Delayed gastric emptying of solids: > 60% retention Tc-99m at 2 h and/or > 10% retention at 4 h [1]. Rapid gastric emptying of solids: < 30% retention at 1 h [1]. Normal gastric emptying of solids: < 60% retention at 2 h and < 10% retention at 4 h [1]. Delayed gastric emptying of liquids: > 50% retention of In-111 at 1 h [1]. Delayed small bowel transit: < 40% collection of In-111 in terminal ileum/cecum area at 6 h [1]. Normal small bowel transit: ≥ 40% collection of In-111 in terminal ileum/cecum area including activity having passed into the colon [1]. Using the PAGI-SYM and other survey data we compared how patients with different colonic transit patterns, symptom profiles and demographics varied.
Additional Colonic Transit Parameters
We also calculated two additional colonic transit parameters. First, the percent total In-111 colon retention was determined for 24, 48, 72 h as previously performed by Ziessman et al. and Antoniou [9, 10]. We then correlated these values with the geometric center at 24, 48, 72 h within each colonic transit pattern. Second, the percent change in the colonic geometric center over time (i.e. GC day 2—GC day 1, GC day 3—GC day 2 and GC day 3—GC day 1). This assessment of the progression of the colonic geometric center over time has been suggested to identify additional patients with slow transit constipation (Khoshbin [11]). The mean of each of these values was determined for each colonic transit pattern and correlated with the geometric center at 24, 48, 72 h within each colonic transit pattern. This measurement of colonic transit propagation (CTP) is an assessment of transit time as it shows the difference of location radioactive tracer at each of the different imaging time points.
Statistical Analysis
Data were collected and entered into a Microsoft excel spreadsheet, along with results of the PAGI-SYM. Numeric data are expressed as mean ± standard deviation (SD). Data are correlated using Pearson correlations, as weak (0.00–0.30), moderate (0.31–0.50), and strong (0.51–1.0) correlations, with significance defined at < 0.05. Data analysis were performed in a commercially available software package (Microsoft Excel, USA). After these relationships were determined, we determined significance as a p value less than 0.05 using statistical testing such as ANOVA and Chi square testing.




Comments (0)