
Remember me



The patient was a 16 year-old boy who was referred to our hospital in July 2022 because of severe heart failure.
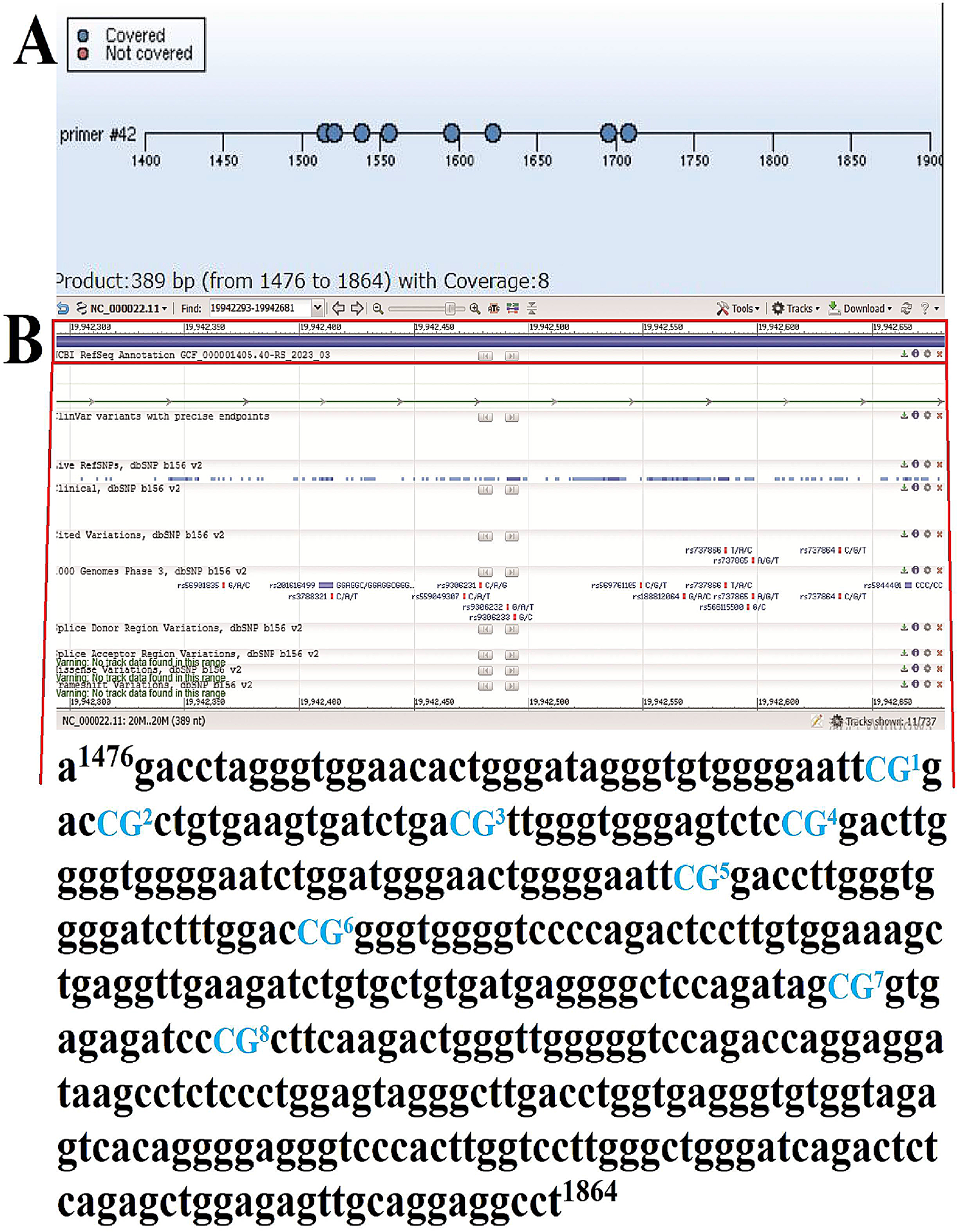
At age 13, he was diagnosed Becker muscular dystrophy carrying with the causative mutation in gene DMD (chrX:32,841,413–32,862,977, Hemizygous mutation), and gene testing showed the comorbid mutations of ABCB4(chr7:87041219, heterozygous mutation) and DSC2(chr18:28659938, heterozygous mutation). He had a history of mild breath shortness and chest distress on exertion and received treatment for cardiac dysfunction; however, heart function became worse and he was referred to our hospital for the first time. Physical examination at his first referral showed a height of 173 cm, body weight of 78 kg, blood pressure of 110/90 mmHg, heart rate of 76 beats/minute regularly, respiratory rate of 20 times/minute, body temperature of 36.5 °C, and SpO2 of 100% under room air. There was no jugular vein dilatation in the neck. His lung and cardiac auscultation sounds were normal. His abdomen was flat. There was slight edema in both instep and ankle. The patient did not show wing-like shoulder blades or lordosis. Pseudohypertrophy of the bilateral gastrocnemius muscle was observed. Gower’s sign was negative. Laboratory test showed that N-terminal prohormone of brain natriuretic pee (NT-proBNP) level was 471.55pg/ml, myohemoglobin was 272.61ng/ml, creatine kinase (CK) was 5,493 U/L, creatine kinase-MB (CK-MB) was 115 U/L, creatine kinase-MM (CK-MM) was 5,378U/L. Alanine aminotransferase (ALT) was 138 U/L, aspartate aminotransferase (AST) was 92 U/L, lactate dehydrogenase (LDH) was 393U/L. The transthoracic echocardiography showed a 19% left ventricular ejection fraction (LVEF), dilation of left atrium, left ventricle and right atrium, mild mitral valve regurgitation, severe LV systolic dysfunction, decreased whole heart diastolic function. Leg MRI revealed that muscular dystrophy changes in bilateral thighs. Medication treatments were started including sacubitril-valsartan, carvedilol, ivabradine, tolvaptan, trimetazidine and adjusted according to the heart failure treatment guidelines in the coming 3 years’ of follow-up. Follow-up echocardiographic LVEF value fluctuated at 30–35%.
On the first day of this referral, the patient suffered deteriorating chest distress, palpitation, and shortness of breath at rest indicating progressive heart failure. He was referred to our hospital at 9:00 p.m. On physical examination, blood pressure of 106/63mmHg, heart rate of 120 beats/minute irregularly, respiratory rate of 20 times/minute, body temperature of 37℃, and SpO2 of 97% on room air. A chest examination revealed moist crackles in both lungs. His heart sounds were intact but irregular, and no heart murmur was observed. His muscle strength was 5/5. Laboratory tests showed the following results: white blood cell count, 10.56 × 109/L with neutrophils 60.5%; hemoglobin, 144 g/L; platelet count, 177 × 109/L. Coagulation function was sightly abnormal, as follows: Prothrombin time (PT), 14.8 s; activated partial thromboplastin time (APTT), 27.1 s; D-Dimer, 0.27 mg/L. Biochemical examination showed potassium of 3.9 mmol/L, creatinine of 67µmol/L. His total bilirubin level was normal, but his liver enzyme levels were slightly elevated, as follows: ALT, 109 U/L; AST, 87 U/L; LDH, 376U/L. NT-proBNP was markedly elevated to 9,171pg/ml. cTnT level was 0.107ng/ml. The electrolyte levels were normal. Electrocardiogram showed atrial fibrillation with rapid ventricular rate and intraventricular heart block.
At 10:00 p.m. on the first day, chest distress was aggravating. 150 mg of amiodarone through intravenous injection failed cardioversion. Ventricular rate was 120 bpm. Then, 450 mg of amiodarone was used for rate and rhythm control through continuous intravenous dripping (6ug/Kg/min). At the same time, we provide continuous infusion of recombinant human brain natriuretic peptide to improve clinical heart function. ECG monitor showed atrial fibrillation with ventricular rate of 90 bpm.
At 1:00 pm on the second day, the patient became pale, sweating and orthopnea. The patients’ blood pressure dropped to 75/50 mmHg, heart rate was 74 bpm. Therefore, amiodarone and recombinant human brain natriuretic peptide was discontinued and intravenous infusion of dopamine and dobutamine was administrated. All oral medications were stopped at the same time. ECG showed a normal sinus rhythm of 84 bpm and second-degree type II atrioventricular block. Emergency bedside echocardiography showed that dilatation of whole heart with reduced systolic function of left and right ventricle (LVEF 25%), mild pulmonary artery hypertension, infinitesimal pericardial effusion. Physical examination showed blood pressure of 89/60mmHg, heart rate of 74 bpm regularly and SpO2 of 99% under 3 L/minute oxygen. Skin mottling was visible on both lower limbs. The urine volume on the second day was 1,000 ml.
On the third day, abdominal ultrasound revealed gallstones and cholecystitis. Meropenem (0.5 g q12h ivgtt) was used empirically to control infection. The urine volume decreased to 400 ml.
On the 4th day, the patient complained of relief of chest distress. Laboratory tests showed the following results: ALT, 7,391 U/L; AST, 5,671 U/L; LDH, 8,089U/L; CK, 2,875pg/ml, CK-MM, 28,522U/L; CK-MB, 229U/L; urea nitrogen, 29.8mmol/L; uric acid, 859µmol/L; creatinine, 305 µmol/L; eGRF, < 30 ml/min/1.73m2; platelet,104 × 109/L; PTs, 29.3 s; APTT, 29.9 s; Fibrinogen, 163 mg/dl; D-Dimer > 40 mg/L. He was referred to ICU for further treatment.
We provided bedside continuous renal replacement therapy. Administrations of isoglycyrrhizinate, reduced glutathione and polyene phosphatidylcholine were given to protect liver function. Dopamine and dobutamine (1.3ug/kg/min) was administrated to sustain blood pressure and strengthen heart contraction. Laboratory examinations were conducted to monitor patient’s related indexes. Coagulation function: PTs was 22 s. D-Dimer was higher than 40 mg/L. Liver function were as follows: total bilirubin level of 75.5µmol/L, ALT of 5,060 U/L, AST of 1,952 U/L, LDH of 8,089U/L. Renal function: blood urea nitrogen of 23.8mmol/L, uric acid of 604 µmol/L, creatinine of 322 µmol/L, and eGRF 23 ml/min/1.73m2. NT-proBNP was 5701 pg/ml, CK was 11476U/L, CK-MM 11308U/L, CK-MB 168U/L. ECG showed a normal sinus rhythm of 62 bpm, intraventricular heart block, left atrial hypertrophy and left axis deviation.
At 10:00 pm on the 5th day, dopamine was discontinued. Blood pressure fluctuated 90–112/50-70mmHg. We administrated oral sacubitril-valsartan 25 mg bid and trimetazidine 35 mg bid on July 10th. Ivabradine (5 mg bid p.o.) and tolvaptan (10 m qd p.o.) were administrated on the 10th day due to stable hemodynamics, improved renal function and increased daily urine volume. Dobutamine was stopped on the 11th day. Low molecular weight heparin was started on the 12th day.
On the 15th day, reexamination of laboratory examinations suggested significant amelioration of liver function. Alanine aminotransferase was down to 255 U/L, aspartate aminotransferase to 35U/L. The daily amount of transfusion was 2,106 ml with daily urinary output of 1,125 ml. Therefore, polyene phosphatidylcholine was stopped. Hemodialysis catheters were removed. A timeline with relevant data from the episode of care was showed in Figs. 1 and 2.
Fig. 1
The timeline with episodes of care and medical treatment for the patient
Fig. 2
The timeline with dynamic alterations of ALT, AST, LDH and CK
Comments (0)