
Remember me







Patients presenting at Saint Joseph University of Beirut dental clinics with a distal-shortened mandible or distal intercalary space of two to three missing premolars or molars (class I, II or VI according to Kennedy’s classification on edentulous spaces) and requiring implant-supported reconstructions were selected to participate in this study.
For each case two implants were placed with a fully guided procedure followed by the insertion of two to three splinted temporary resin crowns that were virtually designed and prepared. Temporary crowns were loaded either immediately or conventionally (after 2 months) depending on primary stability.
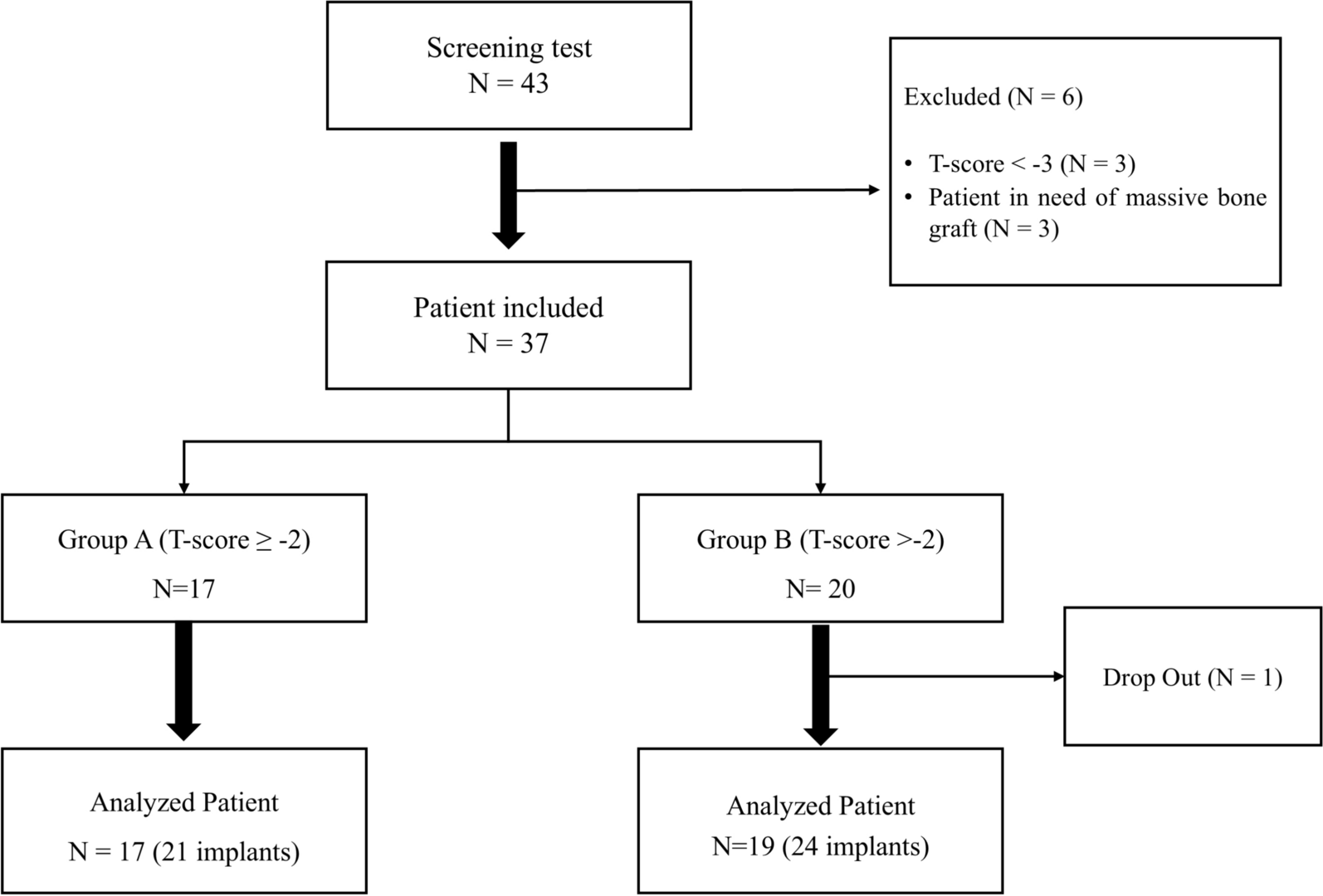
Thirteen patients were included in this study with twenty-five implants eligible for accuracy evaluation. Deviation of final implant position compared to virtually planned implant position was assessed after superimposing the two scanned 3D images.
Inclusion criteriaAge over 18 years old.
Acceptable oral hygiene with no signs of active periodontal disease or local infection.
ASA 1 and 2.
Non or Light smoking (< 10 cigarettes per day).
Acceptable intermaxillary space (44 mm minimum).
Minimal crestal width of 5.5 mm.
Minimal residual bone height of 10 mm above the alveolar nerve canal.
Exclusion criteriaHead and neck irradiation.
Bone grafted sites.
Severe bruxism.
CBCT with exaggerated artifacts.
Limited intermaxillary space.
An Institutional Review Board (IRB) approval was given by the Committee for the Protection of Human Subjects (CPHS) of the Saint Joseph University of Beirut-Lebanon, and an informed consent was signed by all patients.
Pre-operative planningA pre-operative CBCT was taken with an open mouth of 2 cm to prevent any overlap or artifact from the opposite arch. DICOM files (Digital Imaging and Communications in Medicine) derived from the CBCT were imported into Implant Studio (3Shape® Copenhagen, Denmark) planning software.
An optical surface scan was performed using TRIOS (3Shape® Copenhagen, Denmark) optical scan. The resulting 3oxz file (optical 3D image) was exported to the Implant Studio software as well (stage 1 A and 1B Fig. 1).
Fig. 1
The 4 stages of the digital workflow leading to deviation assessment. Stage 1 and 2 are pre-implant placement; Stage 3 and 4 are post-implant placement. 1 A- DICOM/DCM File exported from CBCT to the planning software for super-imposition; 1B- 3OXZ file exported from the intra-oral scanner to Implant Studio software for superimposition and implant planning; 2- STL file used to print the surgical guide and 3OXZ file used to design and mill the crowns in the dental Lab; 3- Implant scanning and 3OXZ file export to Trios Dental System for flag matching with the scan-body; 4-The Information of the planned implant (4 A) and the placed implant (4B) with coordinates embedded are exported as DCM files to the deviation test tool. (3OXZ: 3Shape Order Exchange Zip File; DICOM/DCM: Digital Imaging and Communications in Medicine; STL: Standard Tessellation Language)
The two 3D images were subsequently superimposed and implant placement was planned in a prosthetically-driven manner. A 2 mm security distance from the alveolar nerve, that was set by the 6th ITI consensus conference in 2018 (6), was respected in this study.
In case of distal edentulous space, a lateral fixation pin was planned to strengthen the guide, prevent its distal bending, and achieve multiple tissue support (mucosal, dental and pin support). After implant planning and guide design (see stage 2 Fig. 1), an STL file (Stereo Lithography interface format) was obtained for guide printing, a 3oxz file for temporary resin crowns fabrication, and a DICOM file for future superimposition with the final implants position (stage 4 A Fig. 1).
Surgical guide and crown manufacturingSTL files were used to print the resin surgical guide with a 3D printer - Envisiontec (Envisiontec Vida HD, Envisiontec Inc, USA). Lateral windows for seating check, additional bars for reinforcement and metal rods inserted into the resin for higher rigidity were designed (Fig. 2).
Fig. 2
Surgical guide with reinforcement bars, fixation pin for distal edentulous spaces, lateral windows for posterior sites and occlusal windows for seating control
For immediate loading protocols, virtual splinted crowns were designed using a Dental System DS Software (3Shape, Copenhagen, Denmark) and produced by a milling machine (Amann Girrbach AG, Koblach, Austria).
To basically evaluate the accuracy of CAD/CAM processes, a mandibular cast was printed with replicas of planned implants inserted into this model, and three tests were effectuated (Fig. 3). Firstly, the surgical guide fit was checked by seating the later over the printed model and appraising its stability. Secondly, implant placement procedure was tested performing a simulation and evaluating if the laser mark of implant holder corresponds to the planned level of offset. Thirdly, the crown fit was assessed on the corresponding screw-retained Variobase abutments from Straumann. These tests proved the accuracy of pre-operative steps related to the digital workflow. Thus, CAD/CAM protocol was free from any source of distortion.
In cases of reduced mouth opening, a lateral window was created in the sleeve and guide to prevent any pressure during drilling procedures.
Fig. 3
Simulation proving the accuracy of the pre-operative steps related to the digital workflow: a- Printed cast with preparation for implant digital analog. b- Control of the surgical guide seating. c- Simulation of free-hand implant insertion by checking the laser-mark of the implant holder. d- Positioning the screw-retained splinted crowns to validate the accuracy of their seating once again
Guided implant surgery protocolOnly one experienced and skilled investigator was in charge to perform all the surgeries in respect with the consistency of the protocol.
After local anesthesia, the surgical guide was seated, 1.25 mm fixation pins (Straumann) were placed, stability of the surgical guide was checked, and special attention for rocking or loose fit of the guide was accorded. Surgical guides were tooth-mucosa supported and were stabilized with fixation pins (Fig. 4). Depending on the thickness of the tissue and the amount of keratinized tissue around the implantation area, the investigators decided to either choose a flapless or open-flap procedure.
Fig. 4
Design of the surgical guide with fixation pin and fitting of the printed guide intra-orally during surgery
The followed drilling protocol was according to the implant studio planning, using adequate guided surgical cassette, drills with stoppers, and metallic drill handles. After implant site preparation, implants were inserted in a fully guided manner through the sleeve using a guided surgery implant holder with corresponding off-set laser marks. Bone level (BL) and bone level tapered (BLT) Roxolid implants (Straumann AG, Basel, Switzerland) with a diameter of either 3.3–4.1 mm and length of 8–10 mm were chosen.
After the surgery, patients were asked to take the following medications for seven days: Diclofenac as NSAID twice daily, Paracetamol 1 g if needed and mouthwash with Chlorhexidine Digluconate 0.12% three times per day.
Measured parameters1. Primary stability assessment_ At the last rotation during implant insertion, a customized adaptor for the digital ratchet of the insertion torque (IT) device (DTA, by studio AIP Srl, Italy) was used as an implant holder and the values were recorded with a transducer connected to a computer via Bluetooth wireless. A graph displayed the variation of IT with each rotation on DT1 2.2 software, and the highest value was considered the maximum insertion torque in Ncm.
_ Implant stability quotient ISQ was also recorded following the resonance frequency analysis RFA using the Osstell AB ISQ device (Ostell ISQ; Integration Diagnostics AB, Göteborg, Sweden).
The ISQ records were only scored to follow with time the evolution of the implant stability, since it is considered as an assessment which can provide prospective monitoring and shows fluctuations in stiffness of the implant interface as bone matures from primary to secondary contact [15].
In the current study the ISQ was only a variable used to monitor the behavior of the secondary stability after immediate loading.
_ When primary stability of the two implants reached 30 Ncm and above, an immediate loading protocol was applied by inserting two splinted, prefabricated and milled screw-retained crowns on top of Variobase abutments for bridge (Straumann AG, Basel, Switzerland). (Fig. 5)
Fig. 5
Planning and clinical view of an Immediate loading of implants with high primary stability over a screw retained bridge and a surface scan with digital scan bodies of the placed implants
2. Assessment of the deviationsA preliminary clinical visual check of the distortions was observed at the moment of insertion of the pre-milled splinted crowns. For adjustment of misfitted temporary restorations due to inaccuracy of implant placement, a relining or reparation with resin material was performed to ensure a passive fit (Fig. 6).
Fig. 6
Temporary restoration cut with a disc to repair it for a passive fit
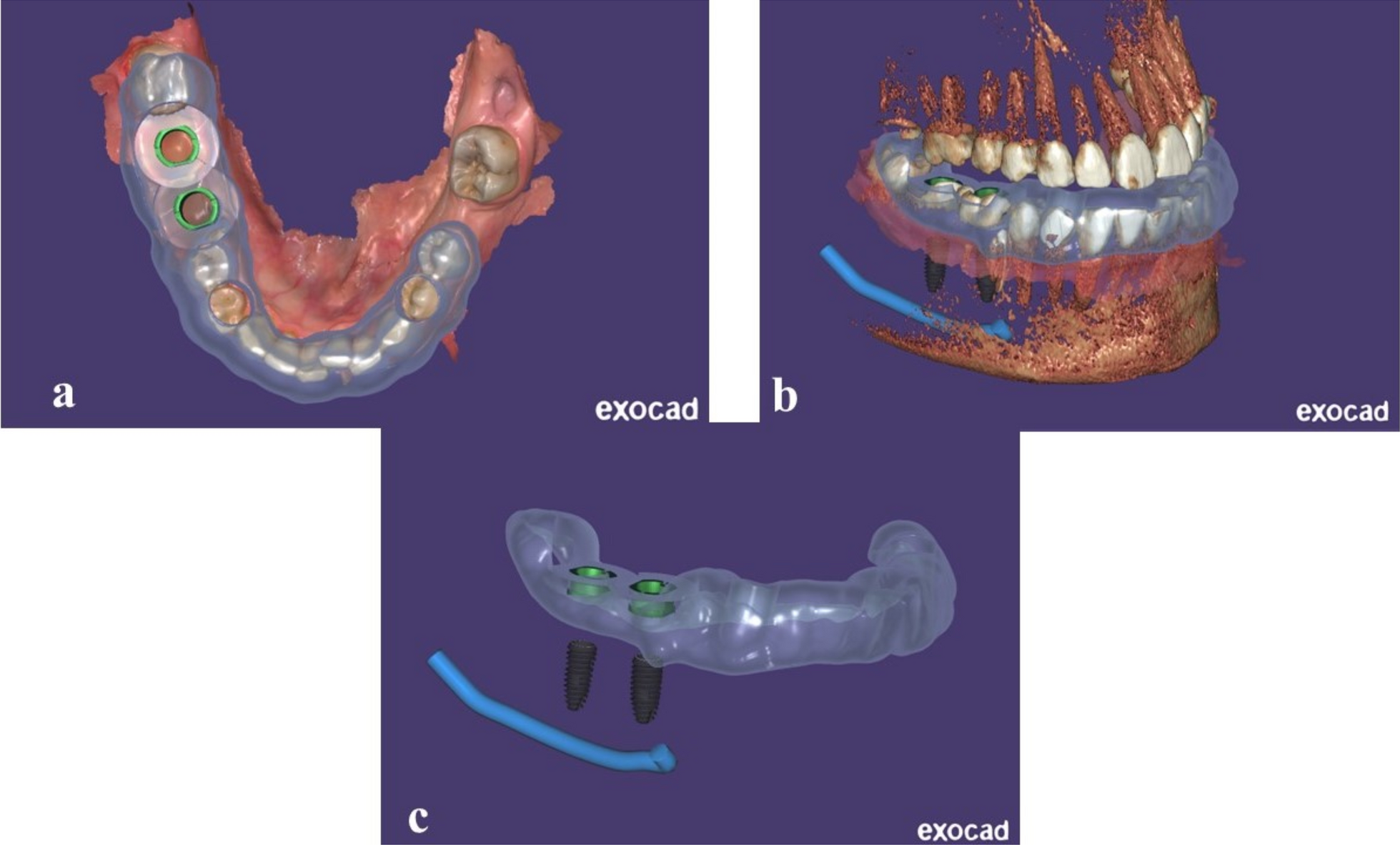
The real assessment of the deviations was performed only at eight weeks after implant placement. Intra-oral surface scans of the final implants’ positions were registered using a digital scan body. Resulting 3oxz output files were exported to the Dental system DS software of 3Shape to generate a DCM file of the placed implant. Afterwards, the deviations between virtual implant VI and placed implant PI positions were calculated with a “comparison tool” developed by 3Shape company for research purposes (Fig. 7; stage 4 Fig. 1).
Fig. 7
3D Viewer software was used to assess the amount of deviation: the 3 coordinate arrows of the Virtual (VI) and the placed (PI) implants were superimposed. Also, the accuracy of the mesial implant (neighboring to natural tooth) was compared to the distal implant
Four different measures were provided to calculate the amount of distortion in millimeter (mm) or in degree: Origo Displacement OD (mm), Horizontal Displacement HD (mm), Error Depth ED (mm) and Error Angle EA (degree) (Fig. 8).
Fig. 8
Deviation parameters obtained with the implant position comparison tool from 3Shape
Comments (0)