
Remember me




In light of surgeons’ pursuit of less invasive treatment modalities, with the aim of improving clinical outcomes, minimally invasive surgery has gained traction over the past decades. However, for liver surgery, the uptake of the minimally invasive approach has been rather slow, due to concerns about hemorrhage control, oncological safety, and the long learning curve of minimally invasive liver surgery (MILS).1 Despite these initial challenges, pioneering surgeons working in highly specialized centers have refined their MILS techniques and reported favorable outcomes in selected patients.2,3
After these early experiences, international guidelines and a plethora of observational and randomized studies have appraised the efficacy of MILS.1,4–9 Hence, the minimally invasive approach has become the reference approach for many liver surgical procedures in expert centers.1,10 Originally, MILS was mainly performed using the laparoscopic approach, but more recently the robotic approach has been increasingly adopted.11,12 In theory, robotic liver surgery (RLS) should offer at least comparable benefits over open surgery as laparoscopic liver surgery (LLS), and recent studies have supported this hypothesis.13,14 Nevertheless, evidence supporting the implementation of RLS is still relatively scarce, and its associated costs are generally higher than those of laparoscopic surgery.11 In fact, clear advantages of RLS over LLS have rarely been demonstrated, despite the technical advantages that the robot offers, such as integrated 3-dimensional systems, improved stability, and dexterity.15–17
Therefore, the exact role of the robotic approach in liver surgery remains to be defined. The aim of this study is thus to compare the perioperative outcomes of RLS and LLS in various settings. The composite outcome measure “textbook outcome” was used as the primary outcome measure, as composite outcome measures may offer a more accurate reflection of overall surgical quality.18,19
METHODS Study DesignTo perform this international multicenter retrospective cohort study, the prospectively maintained databases of 34 hepatobiliary referral centers from 15 countries were bundled and retrospectively assessed. Consecutive patients (≥18 years) who underwent an elective robotic or laparoscopic liver resection from January 2009 to December 2021 were included. Patients who underwent hand-assisted procedures, preoperative portal vein embolization, portal vein ligation or associating liver partition and portal vein ligation for staged hepatectomy, major concurrent procedures (eg, vascular or biliary reconstructions, colorectal, diaphragmatic, or pancreatic resections) and patients who did not undergo a formal liver resection (eg, cyst fenestration) were excluded. The included patients were stratified according to the allocated surgical approach (robotic or laparoscopic). Thereafter, subgroups were created according to the type of procedure that was performed: (1) minor resections in the anterolateral segments (segments 2, 3, 4b, 5, and 6), (2) posterosuperior segments (segments 1, 4a, 7, 8), and (3) major resections (3 or more contiguous Couinaud segments). The characteristics and perioperative outcomes of RLS and LLS in the overall cohort and subgroups were compared before and after propensity score matching (PSM), which was applied to mitigate the influence of selection bias.20,21 A standardized survey was conducted among the participating robotic surgeons to clarify whether they regularly use the Cavitron Ultrasonic Surgical Aspirator (CUSA, Integra LifeSciences Corporation), operated by the bedside surgeon. The survey question was formulated as follows, specified for laparoscopic and robotic surgery separately: “How do you perform liver parenchymal transection in your center? Do you use Energy devices, CUSA, or both?” The medical ethical committee of Brescia approved this study and waived the need to obtain informed consent due to its retrospective nature and the use of pseudonymized data. (judgment’s reference number: NP 5403) This report was written following the guidelines outlined in the “Strengthening The Reporting of Observational Studies in Epidemiology” statement.22
Definitions and OutcomesData were collated from electronic health records. Baseline characteristics comprised patient demographics, American Society of Anesthesiologists score, presence of cirrhosis and if present Child-Pugh scale, treatment with neoadjuvant chemotherapy, history of extrahepatic or hepatic abdominal surgery, disease characteristics (type, number of lesions, size of the largest lesion, and uni or bilobar distribution) and the extent and type of resection performed. The extent of liver resections was defined according to the Brisbane 2000 terminology.23 In addition, the “New World Terminology” equivalents, as described by Nagino et al,24 were added between brackets to non–self-explanatory definitions of resections (ie, right hepatectomy, right posterior sectionectomy, etc). No standardized terminology is available for the term “segmentectomy,” but this was considered the resection of the majority of a Couinaud segment. A bisegmentectomy and trisegmentectomy were considered the resection of the majority of 2 or 3 contiguous segments, respectively. A resection of 3 or more contiguous segments was defined as major. Minor resections in the anterolateral or posterosuperior segments were separately reported and analyzed, due to the increased technical difficulty of minimally invasive resections in the posterosuperior segments.5,25 The Institut Mutualiste Montsouris difficulty score was assigned to each laparoscopic and robotic resection, defined according to Kawaguchi et al,26 as follows: grade 1 includes wedge resection and left lateral sectionectomy, grade 2 includes anterolateral segmentectomy and left hepatectomy (H234), and grade 3 includes posterosuperior segmentectomy, right posterior sectionectomy (H67), right hepatectomy (H5678), central hepatectomy (H458), and extended left/right hepatectomy (H23458, H45678, respectively). The intraoperative outcomes included operative time in minutes, estimated blood loss in milliliters, usage and duration of the Pringle maneuver, perioperative packed red blood cell transfusion, intraoperative unfavorable incidents, and conversion to an open procedure. The postoperative outcomes consisted of length of stay, morbidity, and readmissions at 30 days and 90 day or in-hospital mortality. The Oslo classification was used to define and grade intraoperative unfavorable incidents. Postoperative morbidity was defined and graded using the Clavien-Dindo classification and reported as overall and severe (Clavien-Dindo: ≥ 3a).27,28 Posthepatectomy bile leak and liver failure were defined and graded according to their respective International Study Group of Liver Surgery classifications.29,30 Whether or not a patient achieved a textbook outcome was derived from the available perioperative outcome data. The validated survey-based definition of textbook outcome in liver surgery (TOLS) was used.31 Thus, TOLS was defined as the absence of intraoperative incidents of grade 2 or higher, postoperative bile leak grade B or C, severe morbidity, readmission, and 90-day or in-hospital mortality with the presence of an R0 resection margin in case of malignancy. The absence of a prolonged length of stay was added to define textbook outcome + (TOLS+), using the previously reported cut-offs of >4 days for minor and >7 days for major resections.31
Statistical AnalysesSeveral variables contained missing data in a missing at-random pattern (Supplemental Digital Content Fig. 1, https://links.lww.com/SLA/F45). Therefore, a single imputation was applied. Outcome data were not imputed. Categorical data were reported as counts and percentages and compared between the robotic and laparoscopic groups using χ2 or Fisher exact test, when appropriate. Normally distributed continuous data were reported as the mean with its standard deviation (SD) and compared using an unpaired T test. Non-normally distributed continuous data were reported as the median with its range and compared using the Mann-Whitney U test. The distribution was evaluated by visual inspection of histograms and Q-Q plots. Subsequently, PSM was applied in a 1:1 ratio without replacement on the overall cohort and the predefined procedure subgroups, using a caliper width of 0.2.32 Propensity scores were calculated using multivariable logistic regression models.33 Factors that could influence the allocation to robotic or laparoscopic surgery were entered as covariates in this model: age, sex, American Society of Anesthesiologists classification, presence of cirrhosis and grade (Child-Pugh Scale), history of previous hepatic surgery, type of resection, and type and extent of disease (pathologic diagnosis, number of lesions, size of the largest lesions, and uni or bilobar distribution). A sensitivity analysis was conducted, wherein this process was repeated on the subgroup of patients that underwent surgery from January 2015 onwards, to correct for possible influences of the learning curve and improvements in perioperative care. After matching, a balance was assessed using standardized differences. A SD ≤0.1 is considered optimal balance.34 Categorical data were compared using the McNemar test. Ordinal and continuous data were compared using the Wilcoxon signed-rank test. All analyses were performed according to the intention-to-treat principle. A 2-sided P value < 0.05 was considered statistically significant. Data were analyzed using IBM SPSS Statistics version 29.0 (IBM) and R for Mac OS X version 4.2.1 (R Foundation for Statistical Computing).
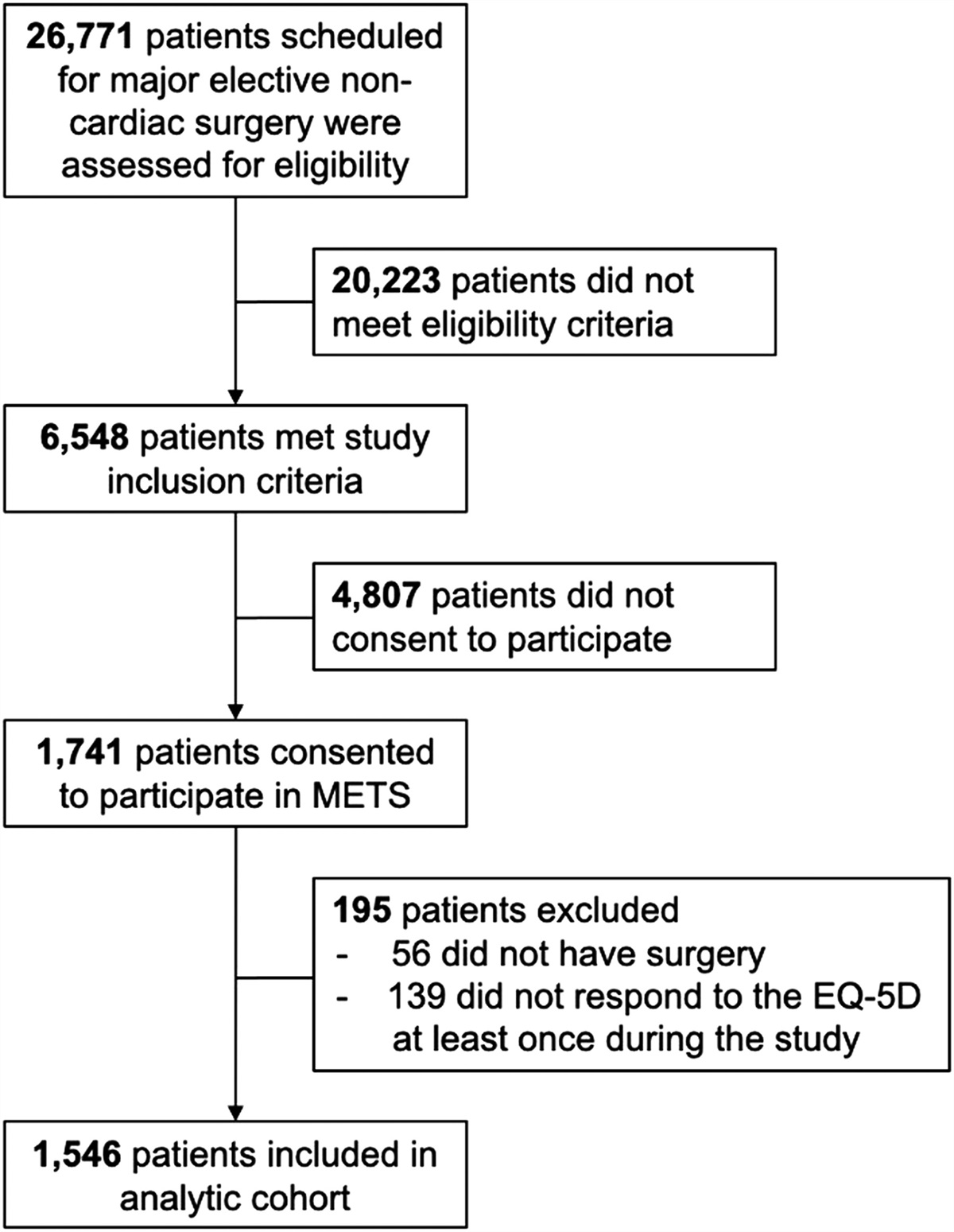
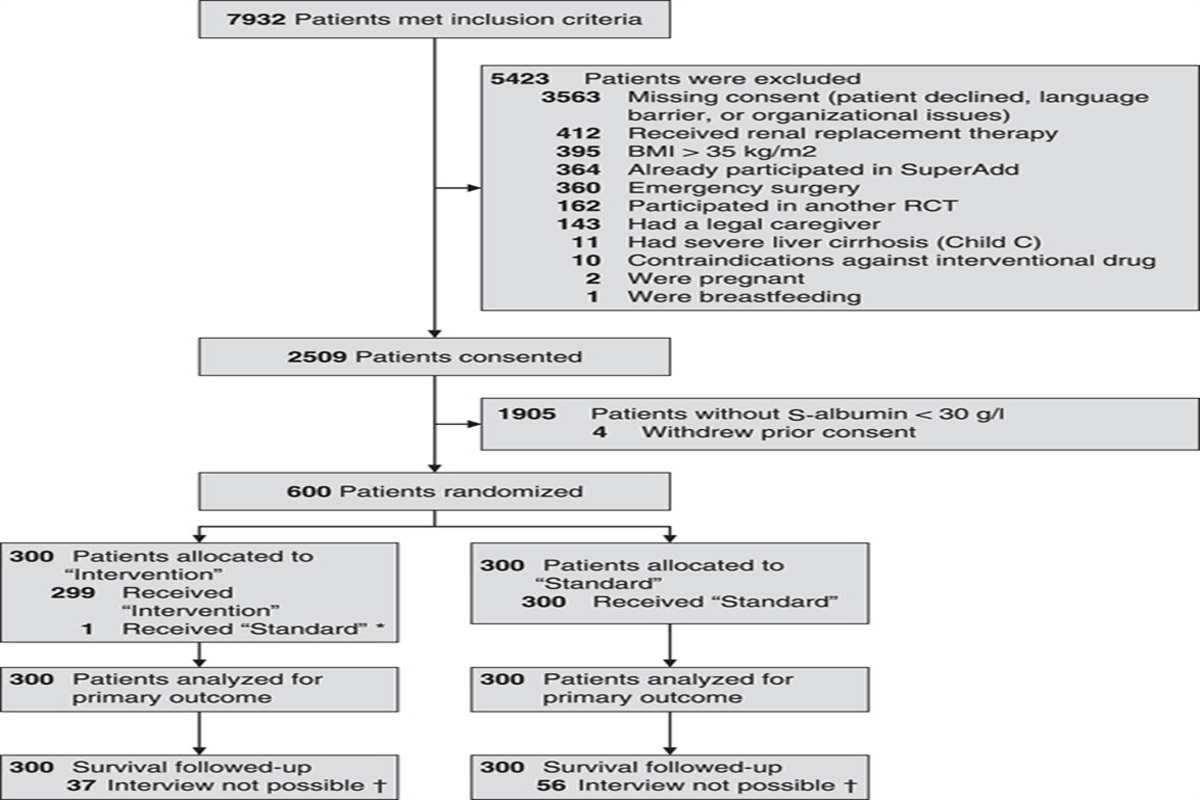
RESULTSOverall, 10.075 patients were included (Fig. 1). Of these patients, 1.507 underwent RLS and 8.568 LLS. Of the participating centers, 23 centers performed both RLS and LLS, 9 centers only LLS, and 2 centers only RLS. The subgroups comprised 5.464 patients for minor resections in the anterolateral segments, 2.862 patients for minor resections in the posterosuperior segments, and 1.749 patients for major resections.
 FIGURE 1:
FIGURE 1: Study flowchart. AL, indicate anterolateral; ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; PS, posterosuperior; PVE, portal vein embolization; PVL, portal vein ligation.
Patient Characteristics and Perioperative Outcomes in the Overall Cohort, Before Propensity Score MatchingBaseline characteristics of patients allocated to RLS and LLS revealed that the RLS group was associated with slightly younger age (Median 62 vs 64.6 years, P < 0.001) and a higher prevalence of liver cirrhosis (25% vs 20.4%, P < 0.001). In terms of lesion characteristics, the RLS group was associated with more singular lesions , and larger lesion size (median 36 vs 30 mm, P < 0.001). Furthermore, while a greater proportion of patients in the RLS group was affected by hepatocellular carcinoma (34.3% vs 25.8%, P < 0.001) or benign liver disease (27% vs 17.7%, P < 0.001), the proportion of patients with colorectal liver metastases was significantly lower (21.6% vs 40.1%, P < 0.001; Supplemental Digital Content Table 1, https://links.lww.com/SLA/F45). The RLS group demonstrated lower rates of previous hepatic surgery (5.7% vs 9.3%, P < 0.001) and treatment with neoadjuvant chemotherapy (16.7% vs 26.7%, P < 0.001). Concerning the performed procedures, the proportion of major resections was higher in the RLS group (21.9% vs 16.6%, P < 0.001), whereas the proportion of patients who underwent concurrent thermal ablations was lower (2.2% vs 5%, P < 0.001). Compared with LLS, the RLS group generally consisted of patients that underwent resections with higher Institut Mutualiste Montsouris difficulty scores (grade 1: 72.4% vs 62.3%, grade 2: 15.2% vs 23.3%, grade 3: 12.4% vs 14.4%, P < 0.001).
Intraoperatively, RLS was associated with a longer operative time [median: 190 (IQR: 139–272) vs 190 minutes (123–270), P = 0.013], a shorter Pringle duration when applied (median: 30 vs 40 minutes, P < 0.001), less blood loss (median: 100 vs 200 mL, P < 0.001), transfusions (4.9% vs 6.2%, P = 0.046), grade 2 intraoperative incidents (2.4% vs 4.4%, P < 0.001), and conversions (2.7% vs 7.1%, P < 0.001; Table 1). During the postoperative course, the median length of stay was 4 days in both the patients allocated to RLS and LLS (P = 0.008). RLS was, however, associated with slightly lower rates of microscopically positive resection margins (R1; 10.1% vs 15%, P < 0.001), paralleled by higher rates of TOLS (78.3% vs 71.8%, P < 0.001) and TOLS+ (54.9% vs 50.9%, P = 0.005). Conversely, the readmission rate was higher in the robotic group (6.3% vs 4.4%, P = 0.002).
TABLE 1 - Intra and Postoperative Outcomes in the Overall Cohort Stratified by the Used Surgical Approach, Before and After PSM Before PSM After PSM Robotic (n = 1.507) Laparoscopic (n = 8.568) P Robotic (n = 1.505) Laparoscopic (n = 1.505) P Intraoperative Pringle maneuver 589 (39.2) 3450 (41.3) 0.118 587 (39.1) 692 (47.1) <0.001 Pringle duration 30 (20, 45) 40 (25, 60) <0.001 30 (20, 45) 40 (25, 60) <0.001 Operative time 190 (139, 272) 190 (123, 270) 0.013 190 (139, 272) 210 (136.3, 300) 0.015 Intraoperative blood loss 100 (50, 280) 200 (100, 400) <0.001 100 (50, 280) 200 (100, 400) <0.001 Transfusion of packed cells 72 (4.9) 468 (6.2) 0.046 72 (4.9) 105 (7.9) 0.003 No. of transfusions 2 (1, 3) 2 (1, 3) 0.595 2 (1, 3) 2 (1, 3) 0.850 Intraoperative incidents — — <0.001 — — 0.003 Grade 1 129 (8.7) 427 (5.6) — 129 (8.7) 86 (6.4) — Grade 2 36 (2.4) 338 (4.4) — 36 (2.4) 77 (5.7) — Grade 3 3 (0.2) 10 (0.1) — 3 (0.2) 2 (0.1) — Conversion 39 (2.7) 591 (7.1) <0.001 39 (2.7) 130 (8.8) <0.001 Postoperative Length of stay, days 4 (3, 6) 4 (3, 6) 0.008 4 (3, 6) 4 (3, 6) 0.398 Overall morbidity 291 (19.3) 1830 (21.5) 0.060 291 (19.3) 384 (25.7) <0.001 Severe morbidity 97 (6.4) 593 (7.0) 0.465 97 (6.5) 113 (7.6) 0.331 Readmission 93 (6.3) 337 (4.4) 0.002 93 (6.3) 66 (4.9) 0.090 90-day or in-hospital mortality 23 (1.5) 113 (1.3) 0.511 23 (1.5) 21 (1.4) 0.880 Resection margin status — — <0.001 — — 0.015 Microscopically radical (R0) 1130 (89.8) 6546 (84.7) — 1129 (89.8) 1126 (86) — Microscopically irradical (R1) 127 (10.1) 1160 (15.0) — 127 (10.1) 180 (13.8) — Macroscopically irradical (R2) 1 (0.1) 20 (0.3) — 1 (0.1) 3 (0.2) — Prolonged length of stay* 486 (32.5) 2661 (31.7) 0.530 484 (32.4) 501 (33.9) 0.493 Textbook outcome 1093 (78.3) 5275 (71.8) <0.001 1091 (78.3) 941 (71.8) <0.001 Textbook outcome + 779 (54.9) 3918 (50.9) 0.005 779 (55) 689 (50.4) 0.026Values are expressed in counts (percentages) or in median (IQR).
Counts may not add up due to missing data.
*Defined as >4 days for minor and >7 days for major liver resections.
After PSM, the RLS and LLS groups both included 1.505 patients. Optimal balance between the groups, with respect to the preselected covariates, was observed after matching (All SD ≤ 0.055; Supplemental Digital Content Table 1, https://links.lww.com/SLA/F45). Concerning intraoperative outcomes, RLS was now associated with less Pringle usage (31.9% vs 47.1%, P < 0.001), shorter operative times (190 vs 210 minutes, P=0.015), a shorter Pringle duration (median: 30 vs 40 minutes, P < 0.001), less blood loss (100 vs 200 mL, P < 0.001), transfusions (4.9% vs 7.9%, P = 0.003), grade 2 intraoperative incidents (2.4% vs 5.7%, P = 0.003), and conversions (2.7% vs 8.8%, P < 0.001; Table 1). Postoperatively, RLS was associated with reduced rates of overall morbidity (19.3% vs 25.7%, P < 0.001), R1 resections (10.1% vs 13.8%, P = 0.015), increased rates of achieving TOLS (78.3% vs 71.8%, P < 0.001), and TOLS+ (55% vs 50.4%, P = 0.026).
Perioperative Outcomes in the Subgroup of Minor Resections in the Anterolateral Segments, After Propensity Score MatchingThe subgroup of patients who underwent a minor resection in the anterolateral segments consisted of 744 patients allocated to RLS and 4.720 patients allocated to LLS. After PSM, 743 patients remained in each group. The included covariates were well balanced after matching (All SD ≤ 0.052; Supplemental Digital Content Table 2, https://links.lww.com/SLA/F45). Intraoperatively, RLS offered several benefits over LLS, in terms of less Pringle usage (26.5% vs 34.2%, P < 0.001), shorter Pringle duration when applied (median: 25 vs 33.5 minutes, P = 0.023), less blood loss (median: 100 vs 150 mL, P < 0.001), transfusions (2.6% vs 5.5%, P = 0.010), and conversions (1.2% vs 4.8%, P < 0.001; Table 2). Despite observing slightly higher rates of R0 resection margins, TOLS, and TOLS+ readmissions, these differences were not statistically significant.
TABLE 2 - Intra and Postoperative Outcomes of Minor Resections in the Anterolateral Segments Stratified by the Used Surgical Approach, After PSM Robotic (n = 743) Laparoscopic (n = 743) P Intraoperative Pringle maneuver 196 (26.5) 247 (34.2) <0.001 Pringle duration 25 (18.3, 37.8) 33.5 (20, 50) 0.023 Operative time 165 (120, 225) 160 (110, 235) 0.394 Intraoperative blood loss 100 (30, 200) 150 (50, 300) <0.001 Transfusion of packed cells 19 (2.6) 36 (5.5) 0.010 No. of transfusions 2 (1, 3) 2 (1, 3) NA Intraoperative incidents 0.439 Grade 1 64 (8.8) 26 (3.9) — Grade 2 9 (1.2) 15 (2.2) — Grade 3 1 (0.1) 3 (0.4) — Conversion 9 (1.2) 35 (4.8) <0.001 Postoperative Length of stay (d) 3.9 (2, 5) 4 (2, 6) 0.362 Overall morbidity 144 (19.4) 153 (20.8) 0.558 Severe morbidity 39 (5.3) 42 (5.7) 0.822 Readmission 39 (5.3) 28 (4.1) 0.314 90 d or in-hospital mortality 14 (1.9) 9 (1.2) 0.383 Resection margin status 0.124 Microscopically radical (R0) 536 (89.8) 549 (87.6) — Microscopically irradical (R1) 60 (10.1) 77 (12.3) — Macroscopically irradical (R2) 1 (0.2) 1 (0.2) — Prolonged length of stay* 227 (30.7) 250 (34.4) 0.130 Textbook outcome 564 (82) 508 (79.1) 0.452 Textbook outcome + 410 (58.5) 358 (53.5) 0.069Values are expressed in counts (percentages) or in median (IQR).
Counts may not add up due to missing data.
*Defined as >4 days.
NA indicates not available.
In the subgroup of patients who underwent a minor resection in the posterosuperior segments, 435 patients were allocated to RLS and 2.427 patients to LLS. After PSM, both groups consisted of 431 patients. The chosen covariates were well-balanced after matching (Supplemental Digital Content Table 2, https://links.lww.com/SLA/F45). In these patients, RLS was associated with a shorter Pringle duration (median: 30 vs 45 minutes, P = 0.011), less blood loss (median: 100 vs 200 mL, P < 0.001), and a lower conversion rate (2.9% vs 10.9%, P < 0.001). In addition, RLS achieved higher rates of R0 resection margins (88.3% vs 85.1%, P = 0.104) and TOLS (75.9% vs 71.2%, P = 0.184), although not reaching statistical significance (Table 3).
TABLE 3 - Intra and Postoperative Outcomes of Minor Resections in the Posterosuperior Segments Stratified by the Used Surgical Approach, After PSM Robotic (n = 431) Laparoscopic (n = 431) P Intraoperative Pringle maneuver 227 (52.8) 230 (53.9) 0.884 Pringle duration 30 (20, 45) 45 (25, 69.5) <0.001 Operative time 192 (150, 270) 210 (140, 300) 0.144 Intraoperative blood loss 100 (50, 280) 200 (100, 400) <0.001 Transfusion of packed cells 26 (6.1) 25 (6.5) 1 No. of transfusions 2 (1, 3) 2 (1, 3) 1 Intraoperative incidents 0.278 Grade 1 44 (10.5) 31 (7.9) — Grade 2 11 (2.6) 21 (5.3) — Grade 3 0 1 (0.3) — Conversion 12 (2.9) 45 (10.9) <0.001 Postoperative Length of stay (d) 4 (3, 5.8) 4 (3, 6) 0.584 Overall morbidity 80 (18.6) 96 (22.3) 0.218 Severe morbidity 28 (6.5) 24 (5.6) 0.677 Readmission 24 (5.8) 19 (5.0) 0.749 90 d or in-hospital mortality 3 (0.7) 6 (1.4) 0.505 Resection margin status 0.104 Microscopically radical (R0) 331 (88.3) 315 (85.1) — Microscopically irradical (R1) 44 (11.7) 53 (14.3) — Macroscopically irradical (R2) 0 2 (0.5) — Prolonged length of stay* 168 (39.6) 176 (42.5) 0.375 Textbook outcome 296 (75.9) 262 (71.2) 0.184 Textbook outcome + 189 (47.2) 170 (44) 0.303Values are expressed in counts (percentages) or in median (IQR).
Counts may not add up due to missing data.
*Defined as >4 days.
Of the patients who underwent a major resection, 328 patients were allocated to RLS and 1.421 patients to LLS. After PSM, 321 adequately matched patients remained in each group (all SD ≤ 0.084; Supplemental Digital Content Table 3, https://links.lww.com/SLA/F45). Intraoperatively, RLS was associated with less Pringle usage (49.1% vs 60%, P < 0.001), reduced blood loss (median: 190 vs 300 mL, P < 0.001), and lower conversion rates (5.4% vs 10.3%, P = 0.027). Postoperatively, RLS was associated with a lower overall morbidity rate (20.6% vs 33.8%, P < 0.001), and tended to achieve higher TOLS rates (72.9% vs 67.5%, P = 0.086; Table 4).
TABLE 4 - Intra and Postoperative Outcomes of Major Resections Stratified by the Used Surgical Approach, After PSM Robotic (n = 321) Laparoscopic (n = 321) P Intraoperative Pringle maneuver 157 (49.1) 189 (60) <0.001 Pringle duration 30 (20, 50) 43 (30, 57) 0.049 Operative time 270 (200, 366) 300 (240, 370) 0.197 Intraoperative blood loss 190 (50, 400) 300 (200, 527.5) <0.001 Transfusion of packed cells 26 (8.2) 25 (8.8) 0.760 No. of transfusions 2 (1.3, 2) 2 (1, 4) NA Intraoperative incidents 0.128 Grade 1 20 (6.3) 25 (8.9) — Grade 2
Comments (0)