
Remember me




Prognostication sits at the heart of surgical care. For surgeons, a patient’s prognosis informs not only their surgical candidacy but also what types of operations to offer, how best to manage complications, and when to consider withholding further interventions. For patients and their families, carefully delivered prognostic information can reduce uncertainty and alleviate stress, enable informed engagement in shared decision-making, and facilitate future planning.1 As such, in complex, multidisciplinary care of patients undergoing surgery, treatment planning relies on a cohesive prognostic narrative – which we have termed prognostic alignment. To achieve prognostic alignment, all clinical teams must reach a shared understanding of a patient’s illness trajectory through intentional and explicit discussion. Prognostic alignment garners patients’ trust in their clinicians and facilitates goal-concordant care, pursuing treatments most compatible with patients’ values and preferences. As surgeons and palliative care specialists, we hope to shed light on this previously unnamed but critical aspect of serious illness communication and to illustrate its necessity in surgical care.
PROGNOSTICATIONPrognostication poses an undeniable challenge to clinicians caring for seriously ill patients. Prognostication is difficult in part because it is multifaceted, addressing a range of domains including time (eg, anticipated survival), rate (eg, “slow decline”), experience (eg, potential symptom burden), completeness of recovery (eg, return to baseline function), and clinical gestalt (eg, “poor prognosis”). In addition, prognosis is dynamic, and clinicians must speculate as to how the disease course might shift along various treatment pathways.2 Furthermore, prognosis has variable degrees of reliability. It can be evidence-based when using survival curves, anecdotal when reflecting on clinician experiences, or intuition-driven. As such, clinicians’ varied scope of expertize informs their prognostic assessments, and therefore, clinicians in different fields can easily diverge in prognostic understanding. Each of these features contributes to overall poor prognostic accuracy3 and invites prognostic misalignment across teams. While improving prognostic accuracy poses a looming challenge, avoiding misaligned narratives forms the first step toward enhanced prognostic communication.
PROGNOSTIC MISALIGNMENTMost surgeons have observed a case of prognostic misalignment. This discord, as we will illustrate, often arises in medically complex situations requiring multi-specialty input.
Consider Ms. B, an elderly patient with coronary artery disease and advanced chronic kidney disease, recovering from a quadruple coronary artery bypass graft (CABG). Ms. B develops a postoperative infection contributing to delirium and worsening renal function. She requires continuous dialysis and management in the cardiac intensive care unit (ICU). Her surgical team continues to provide care with support from the ICU, nephrology, and palliative care teams.
The ICU team calls a family meeting with the attending surgeon, nephrologist, and palliative care specialist present. In the meeting, the nephrologist expresses concern that Ms. B, like many of his other patients with acute on chronic renal failure, may never transition to intermittent dialysis and would therefore never survive outside of an ICU. In contrast, the cardiac surgeon shares that she has seen many patients recover from postoperative infections. She perceives small signs of improvement and believes Ms. B will ultimately recover and be discharged to rehab. The patient’s family is confused. Everyone turns to the palliative care specialist, who has been helping manage Ms. B’s delirium, hoping for mediation and clarity.
In Ms. B’s case, the surgeon and nephrologist offer not only distinct but also competing perspectives, heavily shaped by their respective clinical milieus. The teams’ pitfall is not their disagreement itself but rather their lack of preparation and failure to identify the discord in advance of the family meeting.
Multidisciplinary care of seriously ill patients is necessary, but often ripe for discrepant messaging as many specialists (eg, surgery, critical care, nephrology) hone in on their own domains of patient care, focusing most on the organs or systems they treat. As described, varied clinical experiences inform prognostic assessments. Surgeons, nephrologists, and palliative care clinicians train in different environments and encounter distinct patients and problems, which invariably color their prognostic understandings. Prognostic differences can be especially pronounced in complex cases, where teams can easily hold discordant opinions and foresee alternate outcomes.
However, prognostic misalignment occurs not in these different perspectives alone but in the failure of teams to communicate across vantage points. Communication between teams often takes place in the last paragraph of consult notes or over short, paged messages. These brief exchanges, often mediated by junior members of the team (eg, junior residents or physician assistants), do not necessarily convey each team’s prognostic understanding, and they fail to leave space for discussing diverging views. These modes of communication prioritize efficient information-sharing over effective dialog and, as such, may mask the extent of prognostic misalignment.
Unsurprisingly, prognostic misalignment bars optimal communication with patients and families. When teams present diverging illness narratives, propose competing plans, or reveal discord in a family meeting, patients and their loved ones become confused at best and distrustful at worst. As surgeons, we stand to lose the rapport we have built with patients and diminish their confidence in our capabilities when they observe a lack of consensus across teams. Recognizing prognostic misalignment early provides an opportunity for teams to correct course, improving communication and, therefore, improving patient care. Importantly, when a surgical decision is on the line or when a patient faces a postoperative complication, surgeons can and should spearhead efforts to achieve prognostic alignment.
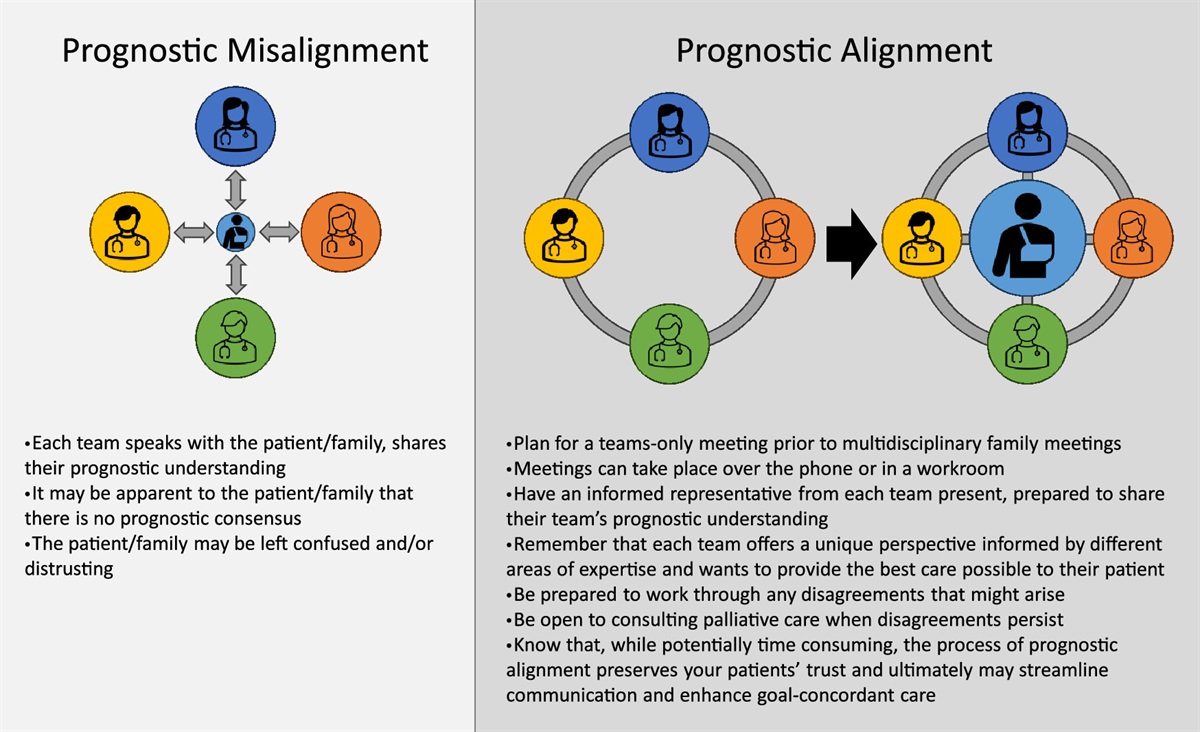
PROGNOSTIC ALIGNMENTWe coined the term prognostic alignment to describe a foundation for serious illness communication built by teams intentionally developing a unified prognostic narrative. We illustrate and outline recommendations for achieving prognostic alignment (Fig. 1), but the process can be as simple as teams coming together – whether in a conference room or by phone – to lay out their understandings and, when relevant, to address points of divergence. Each team must first communicate their prognostic viewpoints among their own members to ensure agreement and consistent messaging. In addition, these conversations should include nursing staff as they work at the frontlines of communication with patients and their families. Thereafter, senior decision-makers (eg, attendings or fellows) should each present their prognostic narratives at the multidisciplinary discussion. When necessary, although not ideal, a junior team member adequately equipped with prognostic information can stand in as a representative.
 FIGURE 1:
FIGURE 1: The model of prognostic alignment. Complex care often invites prognostic misalignment, in which teams hold discordant views of a patient’s prognosis. When teams present discrepant messaging to patients, it limits the patient and family’s ability to engage in decision-making. In the model of prognostic alignment, team communication can allow for a unified understanding, which empowers patients and facilitates engagement in health decisions.
We recommend checking for and working to establish prognostic alignment whenever multiple teams play significant roles in the management of a medically complex patient. In addition, patients in the ICU for indeterminate periods or those with poor surgical prognoses warrant an interdisciplinary exchange of prognostic information. Most critically, the effort to reach prognostic alignment should precede any multidisciplinary family meetings. In doing so, teams craft a cohesive prognostic narrative and treatment recommendation, informed and strengthened by collective expertize. Especially when teams recognize prognostic misalignment prior to a family meeting, they can identify where and why misalignment exists, and work to develop a shared understanding.
Sometimes, despite best efforts, consensus remains difficult to reach. In these cases, teams can shift the focus of their alignment efforts toward clearly verbalizing their disagreements. Teams should prepare to present disagreements to patients and families in a way that minimizes the distress that could arise for patients choosing between clinicians’ distinct recommendations. Palliative care clinicians can assist in these cases by eliciting the patient’s values, which may clarify which aspect of prognosis (eg, time, function, cognitive ability) could help guide the patient and/or family’s decision-making.
Consider Ms. B again and reset the clock. She remains in the ICU after a CABG complicated by a postoperative infection resulting in delirium and renal failure. This time, the cardiac surgeon suggests a teams-only huddle before the family meeting. Informed representatives from the surgery, ICU, renal, and palliative care teams gather in a conference room to share their prognostic understanding and recommendations for Ms. B. It becomes apparent that the surgeon foresees Ms. B’s condition improving as her infection resolves, while the nephrologist suspects her kidneys will never recover from this insult. The 2 clinicians share the data points and clinical experiences, informing their divergent conclusions. The teams agree to acknowledge the uncertainty to Ms. B’s family and discuss parameters that would signify recovery. They suggest a time-limited trial of continuing high-intensity treatments with plans to reconvene in the next few days. The family is grateful for this clarity and agrees with the teams’ recommendation.
CONCLUSIONPrognostic alignment is a new term describing a shared understanding of a patient’s illness trajectory within and across clinical teams. It represents a fundamental aspect of serious illness communication for patients receiving multidisciplinary care. In naming this entity and illustrating a case of prognostic alignment in a postoperative patient, we hope to encourage surgeons to spearhead efforts toward prognostic alignment. Prognostic alignment helps engender patients’ trust in their care teams, imbues patients and families with the knowledge needed to engage in shared decision-making, and facilitates goal-concordant surgical care.
REFERENCES 1. Smith AK, White DB, Arnold RM. Uncertainty — The other side of prognosis. N Engl J Med. 2013;368:2448–2450. 2. Taylor LJ, Nabozny MJ, Steffens NM, et al. A framework to improve surgeon communication in high-stakes surgical decisions: Best case/worst case. JAMA Surg. 2017;152:531–538. 3. Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: Prospective cohort study. Brit Med J. 2000;320:469–472.
Comments (0)