
Remember me


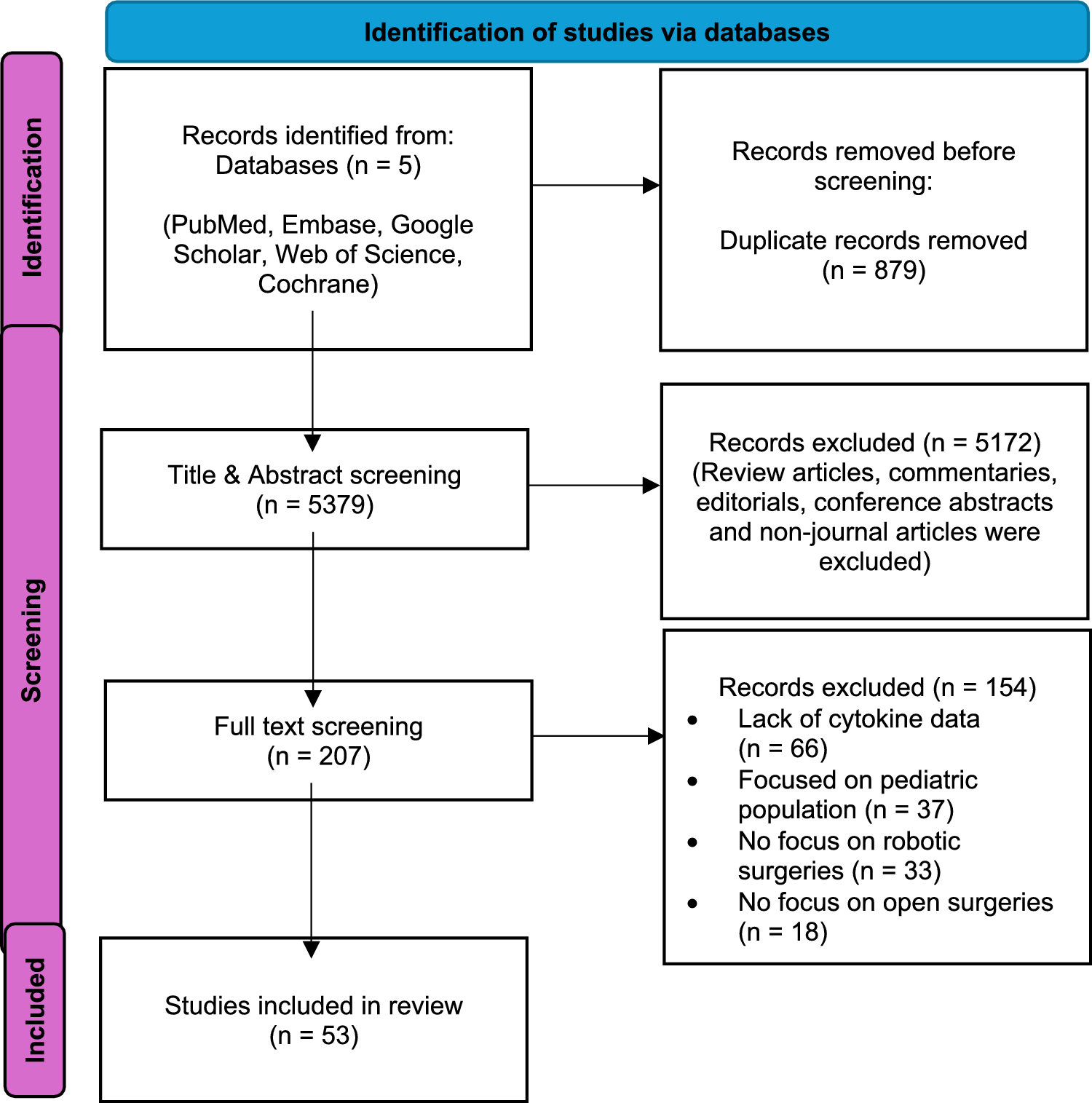
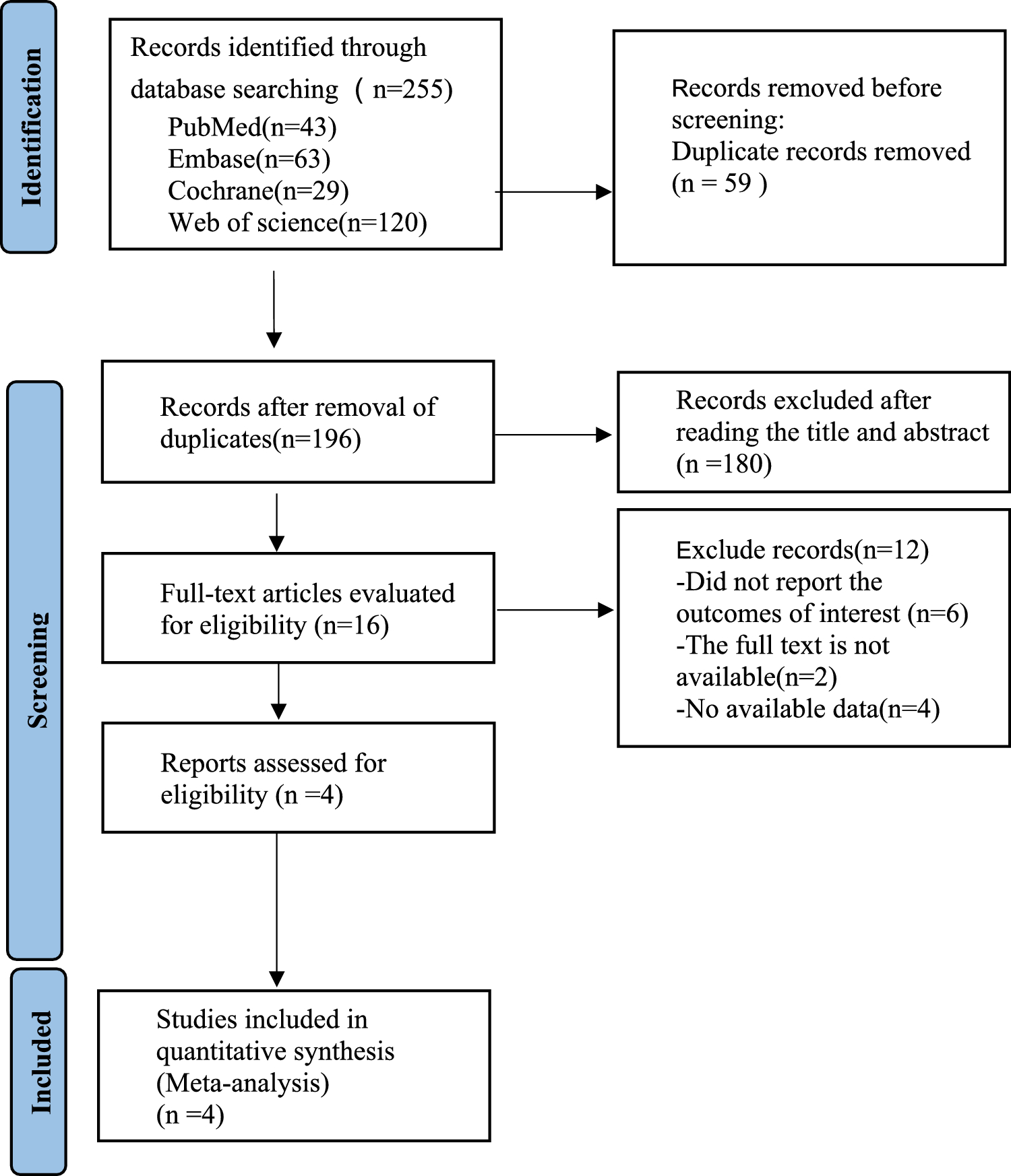

We retrieved 254 citations from the four databases; of these, 199 remained after removal of duplicates. A total of 28 full texts were evaluated for eligibility, among which 8 RCTs were included in the qualitative analysis of this review [9, 11, 23,24,25,26,27,28] (Fig. 1).
Fig. 1
The PRISMA flow chart of study selection and inclusion. THA total hip arthroplasty, RCT randomized controlled trial
Table 1 demonstrates the characteristics of the included trials. We included 8 RCTs published over 25 years from 1998 to 2023. They were conducted in Asia (n = 5) [24,25,26,27,28], the United States (n = 2) [9, 23], and Germany (n = 1) [11], with sample sizes ranging from 54 to 154 hips and mean follow-up time between 1 month and 14 years. Two studies [23, 26] were secondary analyses of the same patient populations at longer follow-up timepoints [9, 25]. Participants’ mean age across the studies ranged from 51.2 to 71.5 years. The ROBODOC system (Integrated Surgical Systems or Curexo Technology Corp., CA, USA) was employed in most studies (n = 7), except one that utilized the TRex-RS (Longwell Company, Shanghai, China), the only system that could operate on both the acetabular and femoral components [28]. The VerSys fiber metal taper stem was used in three studies [25,26,27]. The AML or Osteoloc stem was utilized in two [9, 23] and the S-ROM in one study [11], while two other studies did not specify the stem type used [24, 28]. The posterolateral approach was the most common (n = 5) [9, 23, 25,26,27], followed by the anterolateral approach (n = 1) [11], and modified Hardinge approach (n = 1) [28], with one study not detailing the approach employed [24]. The Harris Hip Score (HHS) was the most common PROMs reported in six studies [9, 11, 23, 24, 26, 28]. Other PROMs were the Short Form-36 (SF36), the Merle d’Aubigne score, and the Western Ontario McMaster Osteoarthritis Index (WOMAC) score, which were reported in two [9, 24], three [11, 25, 27], and one study [24], respectively. Three studies declared funding sources and potential conflicts of interest [9, 24, 25].
Table 1 Characteristics of included trialsRisk of bias in included studiesFigure 2 illustrates our judgement on the study-level risk of bias, and Table 3 elaborates the justifications for our decisions. All studies had high risk of performance bias since surgeons could not be blinded to the intervention. Most studies did not report if some outcome assessors were blinded, whether they registered their trials, nor explain how their sample size was arrived at. The outcome-level risk of bias is reported in Table 2 and the forest plot for that outcome.
Fig. 2
Study-level risk of bias summary
Table 2 Risk of bias of included trials (outcome-level)Table 3 Risk of bias of included trials (study-level) and justifications for judgementsEffects of interventionsThe summary of findings for the main outcomes with the certainty of evidence is presented in the “summary of findings” table, with the reasons for rating down the evidence further elaborated in Table 4.
 Major complications and revision
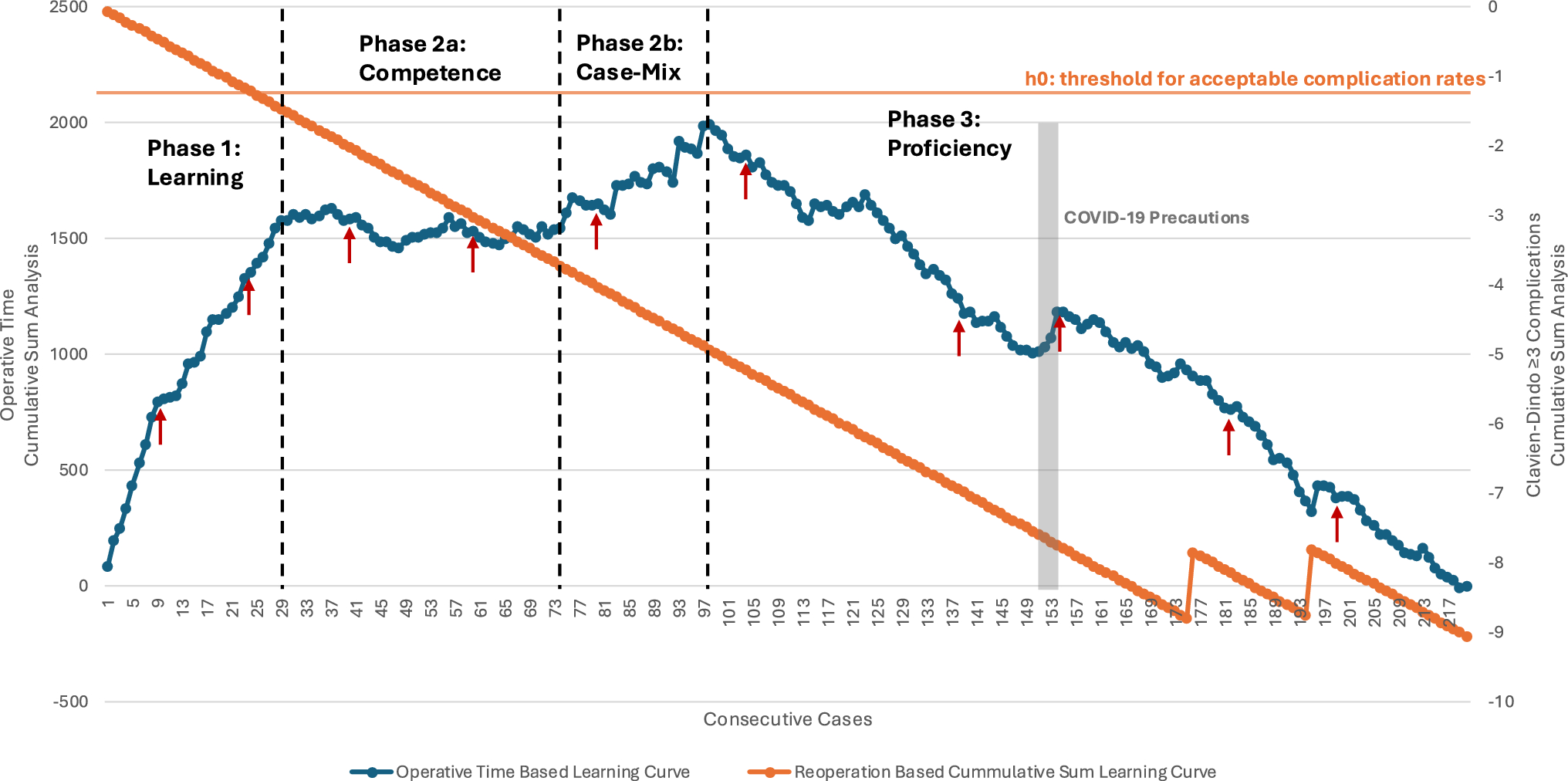
Major complications and revisionFive trials involving 621 hips reported major complications [9, 11, 24, 25, 27]. The combined effect showed that there was no clinically important difference between RATHA and COTHA in the rate of major complication (RR 0.78; 95%CI 0.22 to 2.74, low certainty) as shown in Fig. 3A. Although based on the point estimate, the risk of major complication with RATHA was on average 0.78 times the risk with COTHA, it only translates to a risk difference of 16 fewer per 1000. Also, the estimate was highly imprecise, with the 95%CI covering both large benefit and significant harm. Other than imprecision, the quality of evidence was low due to risk of bias, considerable inconsistency (I2 = 70%), and inadequate information size. The sensitivity analysis found all inconsistency removed (I2 = 0%), and the point estimate and 95%CI shifted further towards the benefit of RATHA (RR 0.55; 95%CI 0.26 to 1.17), but the CI still covered no effect (Fig. 5). There was no significant subgroup effect based on the stem type for major complications.
Fig. 3
Forest plots showing major complication rate (A), revision rate (B), patient-reported outcome measures at 1–5 years (C), leg length discrepancy (D), and femoral stem coronal alignment (E) between robotic-assisted total hip arthroplasty (RATHA) and conventional total hip arthroplasty (COTHA). Note: outcome-level risk of bias legend; (A) randomization process, (B) deviation from intended interventions, (C) missing outcome data, (D) measurement of outcome, and (E) selective outcome reporting. SD standard deviation, IV inverse variance method, CI confidence interval, RATHA robotic-assisted total hip arthroplasty, COTHA conventional total hip arthroplasty
Revision rate was reported in three studies with 364 hips [11, 23, 27]. They were combined with considerable inconsistency (I2 = 89%) and with the point estimate showing a 33% higher risk for RATHA (RR 1.33) which translates to a risk increase of 15 per 1000 compared to COTHA (Fig. 3B). The combined estimate was even more imprecise (95%CI 0.08 to 22.74) than that of complications, and the majority of the combined studies had ‘high risk of bias’, both leading to the very low certainty of evidence for this outcome. Moreover, no sensitivity or subgroup analyses could be performed due to the small number of studies.
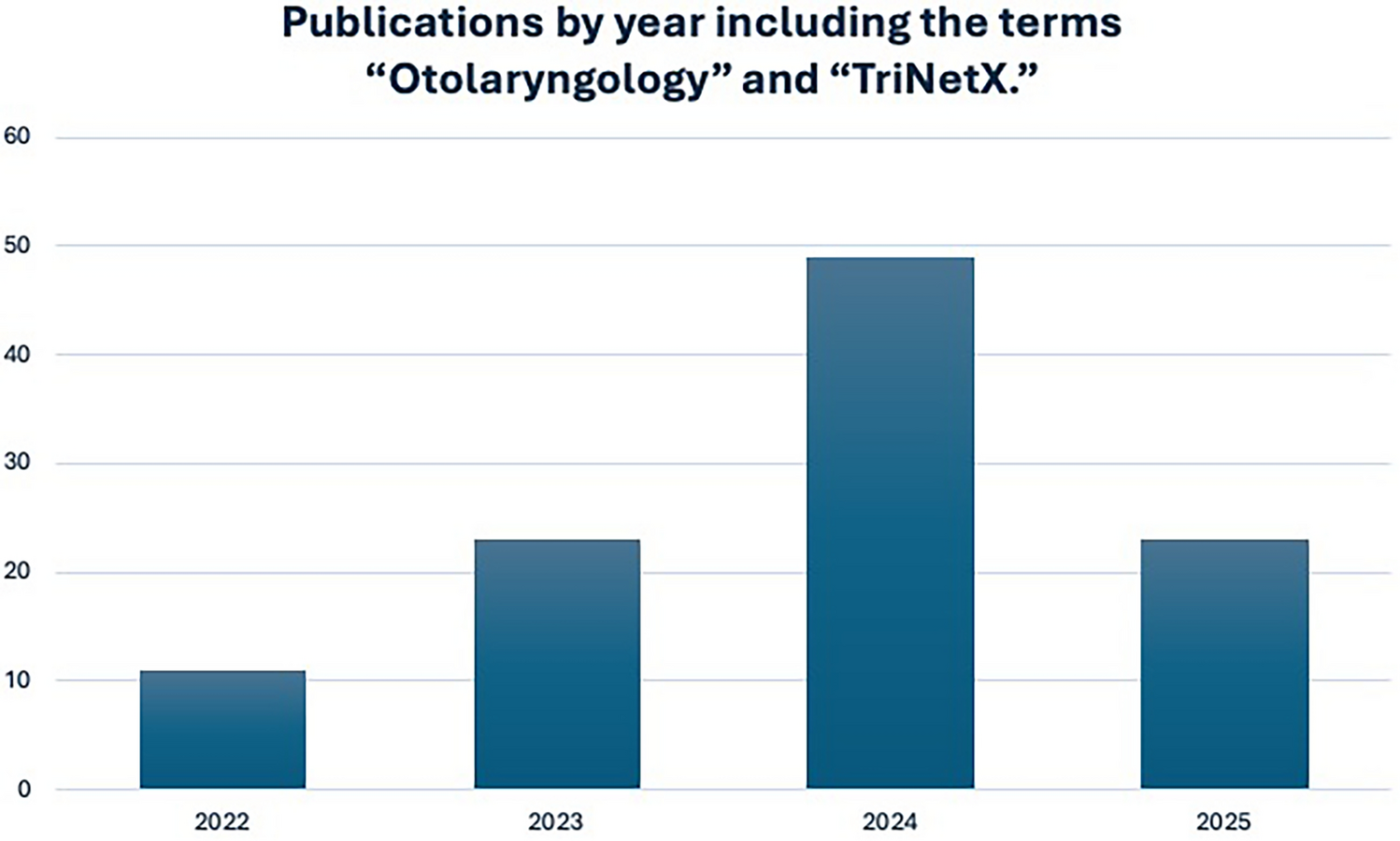
PROMs including pain, walking and daily functionMedium-term PROMs were evaluated in five studies involving 515 patients [9, 11, 24, 25, 27], three of which reported the HHS [9, 11, 24]. RATHA resulted in almost no difference in PROMs compared to COTHA (SMD 0.01; 95%CI − 0.27 to 0.30 SD, low certainty) as presented in Fig. 3C. There was substantial inconsistency (I2 = 61%) that cannot be explained by risk of bias or other study characteristics. The sensitivity analyses of studies without ‘high risk of bias’ (Fig. 5) and with only the HHS (Fig. 6) yielded similar results with very small between-group differences. Similarly, short-term PROMs reported in 3 studies of 368 patients [9, 11, 27] favored RATHA based on the point estimates (0.12 SD higher for RATHA), but the effect size was not likely clinically important, and the 95%CI covered no effect (-0.09 to 0.35 SD) as shown in Fig. 4A. No subgroup effect based on the stem type was found for both PROMs outcomes.
Fig. 4
Forest plots showing patient-reported outcome measures at 3 months (A), intraoperative blood loss (B), operative time (C), femoral stem coronal alignment outliers (D), and femoral stem radiolucency (E) between robotic-assisted total hip arthroplasty (RATHA) and conventional total hip arthroplasty (COTHA). Note: outcome-level risk of bias legend; (A) randomization process, (B) deviation from intended interventions, (C) missing outcome data, (D) measurement of outcome, and (E) selective outcome reporting. SD standard deviation, IV inverse variance method, CI confidence interval, RATHA robotic-assisted total hip arthroplasty, COTHA conventional total hip arthroplasty
Radiological outcomesFor LLD, the results from four studies [11, 24, 25, 28] recruiting 346 hips were combined with considerable heterogeneity (I2 = 86%). LLD for RATHA was on average 4 mm less than that of the COTHA group (95%CI − 7.08 to − 1.0 mm, low certainty) (Fig. 3D). Both sensitivity analyses found results in the same direction favoring RATHA but still with at least substantial inconsistency and small effect sizes that are not clinically meaningful (Figs. 5 and 7). Studies that used non-fully coated stem yielded significantly lower LLD for RATHA compared to those employing fully coated stem (p-value = 0.04) (Fig. 8), though no subgroup effect was found based on study recruitment year (Fig. 9).
Pooled results of 445 hips from 4 studies [9, 11, 24, 27] showed that RATHA resulted in a trivial reduction in femoral coronal stem alignment than COTHA (effect size of 0.57°), with 95% CI including no effect (− 1.16° to 0.03°, moderate certainty) (Fig. 3E). The sensitivity analysis excluding ‘high risk of bias’ studies gave concordant result (Fig. 5). There were no significant subgroup effects, although a tendency towards better alignment in favor of RATHA was found in studies using non-fully coated stems (Fig. 8).
Additional outcomesOverall, RATHA resulted in higher intraoperative blood loss (MD 162.8 ml; 95%CI − 232.2 to 557.9 ml) and prolonged operative time (MD 41.1 min; 95%CI 7.7 to 74.6 min) compared to COTHA (Fig. 4B, C). The superiority of COTHA over RATHA for these two outcomes was significantly more prominent if non-fully coated stem was used (Fig. 8). However, RATHA yielded significantly lower rate of femoral stem coronal alignment outliers (RR 0.08; 95%CI 0.01 to 0.59) (Fig. 4D), although it was not superior to COTHA in terms of preventing femoral stem radiolucency (RR 0.98; 95%CI 0.09 to 10.21) (Fig. 4E). Regardless, it is important to note that the very low number of pooled participants and events in the analyses of these two radiologic measurements.
Comments (0)