
Remember me
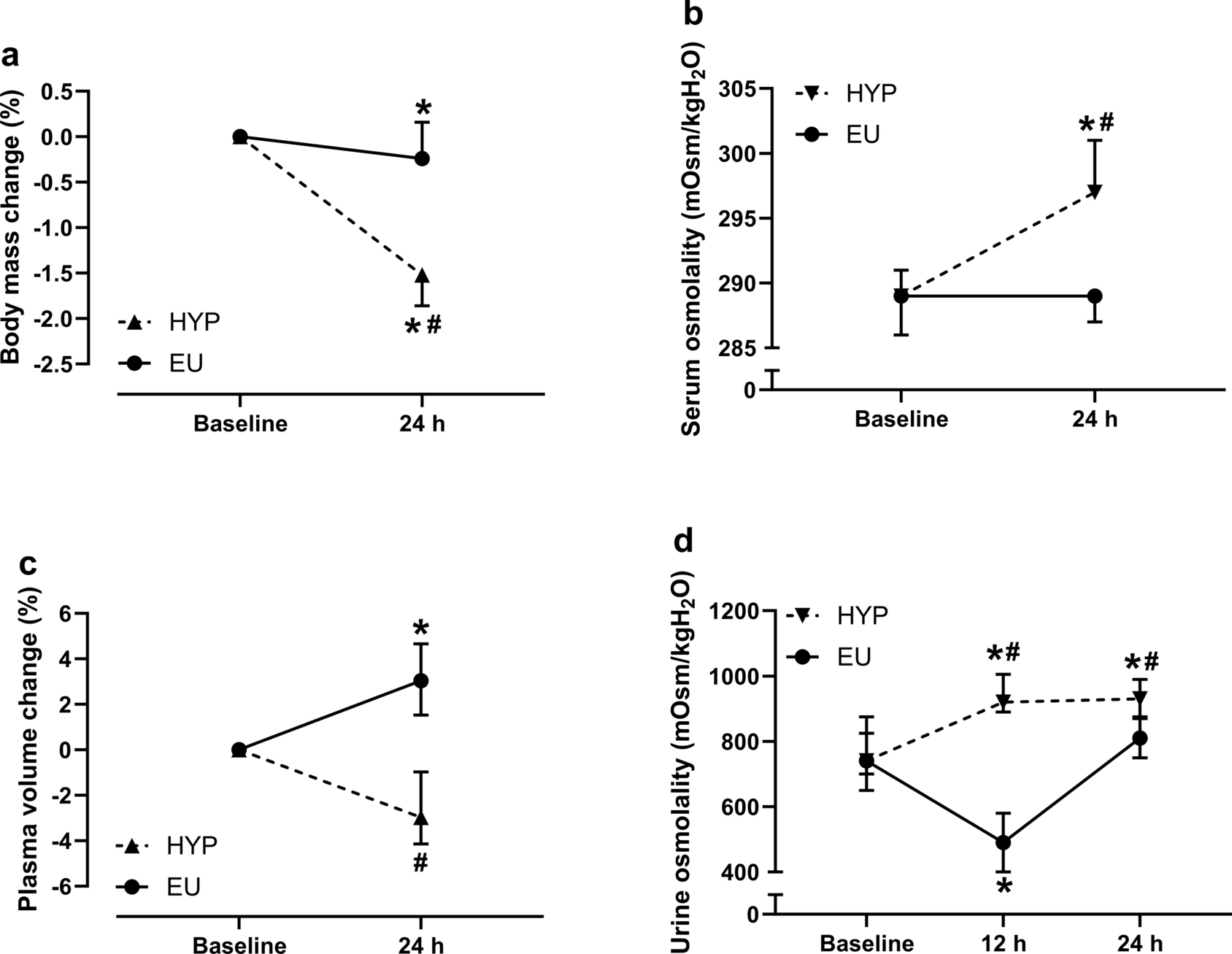
With regard to the design of the study, two groups of adult male volleyball players needed to be recruited: an intervention group that would receive a personalized muscle–tendon training program and a control group that would adhere to their usual training routine. A power analysis was conducted in G*Power (version 3.1.6; HHU, Düsseldorf, Germany) before recruitment to estimate the necessary sample size per group. In an earlier study, we found fluctuations of maximum tendon strain (as an indicator for imbalances in muscle–tendon adaptation) of 0.86 ± 0.40% in adolescent volleyball athletes and 0.31 ± 0.14% in untrained controls (i.e., Cohen’s d = 1.8; Mersmann et al. 2016). We assumed that the personalized intervention could reduce the fluctuations of tendon strain by about 40% (or 0.34 percentage points), which results in an effect size of d = 1.2 for the comparison between athletes of the intervention group and the controls. For a power of 0.8, a sample size of n = 12 per group was calculated. Considering a potential drop-out, 13 and 15 participants were recruited for the control and intervention group, respectively, from two teams from the same division (3rd German Volleyball league). While the players of one team served as control group, the other received the personalized intervention. The sport-specific loading in both groups consisted of an average of two regular training days (2 h each), one competition day (4 h), and one additional athletic training session (1.5 h, focusing on core strengthening and athletic abilities) per week. Participants were excluded if they had neurological or musculoskeletal impairments, while those with patellar tendon pain were included if they could perform maximum voluntary muscle strength testing. Four times over a competitive season (M1–4; M1: one month into the season, M4: one to two month into the off-season), the maximum isometric knee extensor strength, patellar tendon stiffness, and maximum tendon strain were determined using inverse dynamics and ultrasonography. Additionally, we assessed changes in the micromorphological structure of the tendon and the prevalence of tendon pain. Due to scheduling conflicts (e.g., tournaments, sickness, vacation), the time intervals between measurements differed between groups. In the intervention group, the intervals were approximately 17, 12, and 6 weeks between measurements, while the control group had a uniform 12-week interval between measurements. The differing intervals were considered in our analysis (see statistics section). The time between the first measurement and the initiation of the personalized training program was 2.7 ± 0.8 weeks. The participants gave their written informed consent for the experimental procedures, which were approved by the Ethics Committee of the Humboldt-Universität zu Berlin (HU-KSBF-EK_2020_0005) and followed the standards of the Declaration of Helsinki. All measurements were performed on the dominant leg, which was defined as the leg used to kick a ball. The prevalence of patellar tendon-related pain and functional limitations was assessed using the validated German version of the VISA-P questionnaire, which considers symptoms occurring over the past two weeks (Lohrer and Nauck 2011). Participants scoring 87 points or lower were classified as symptomatic, as this score signifies the minimum clinically important difference from the questionnaire's maximum score of 100 points (Lohrer and Nauck 2011). Participants in both groups were excluded if they were not able to attend at least three of the four main measurements. Furthermore, participants of the intervention group who failed to achieve an average training frequency with the personalized exercises of at least two times per week were also excluded. In the intervention group, one participant was excluded from the study due to an injury unrelated to the intervention, two participants did not meet the required training frequency, and two participants withdrew voluntarily before completing the study for undisclosed reasons. In the control group, one participant was unable to complete the study due to an injury unrelated to the study. Therefore, the final sample size in the two groups was 12 and 10 athletes in the control and intervention group, respectively. In the control group, one athlete each in M1 and M4, and two in M3 were unable to attend the measurements.
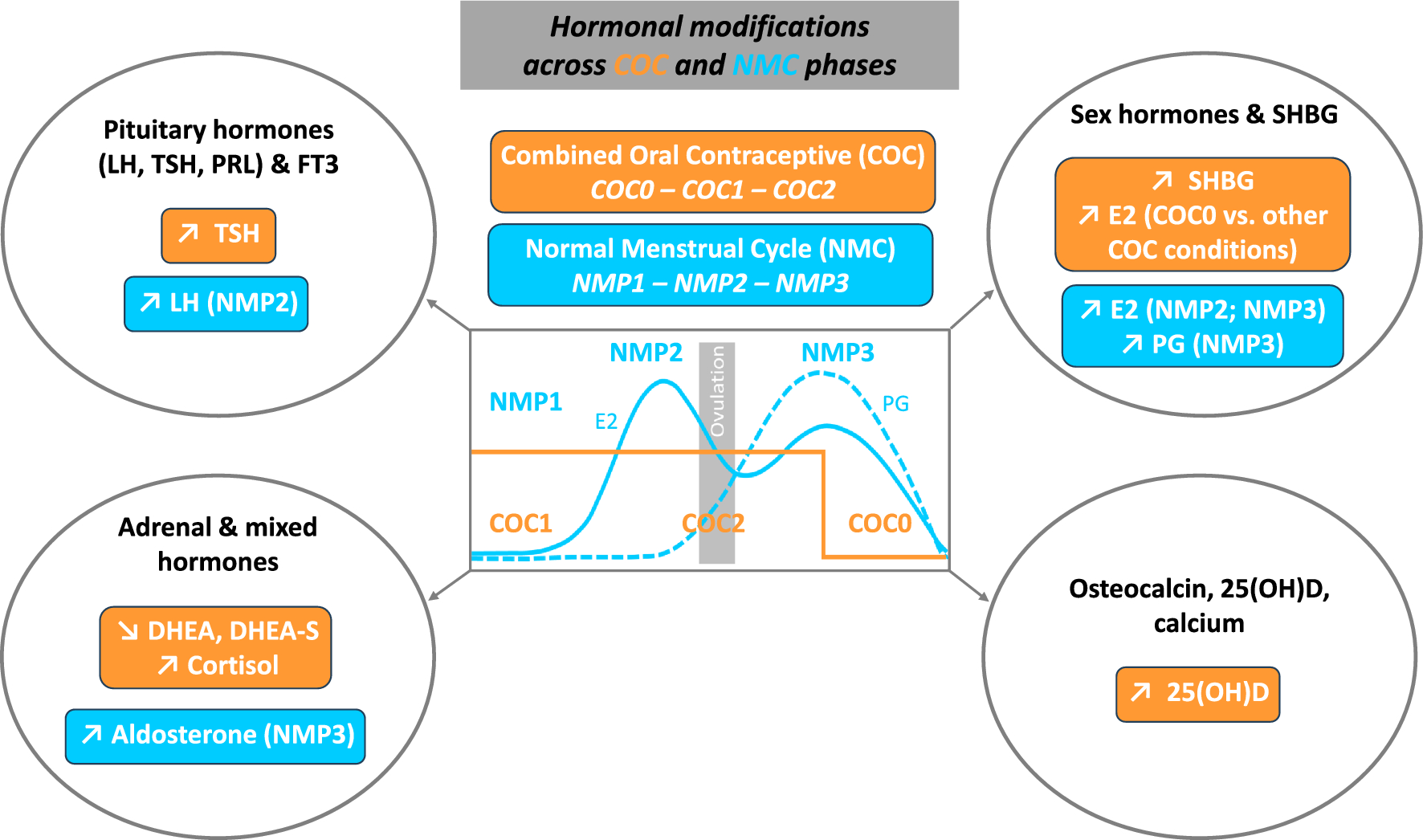
Assessment of maximum knee extensor muscle strengthAfter a standardized warm-up, which included 10 submaximal isometric knee extension contractions with increasing intensity to precondition the tendon (Maganaris 2003) and accustom the participants to the experimental situation, the participants performed two MVCs on a mobile diagnostic device (Fig. 1) at a knee angle of 60° during the plateau of the contraction (0° representing full extension; measured using a goniometer with the assumption of the axis of rotation at the lateral femoral condyle; Churchill et al. 1998) and the trunk in an upright position. This knee joint angle was selected because it is the approximate optimum for knee extensor muscle force generation with regard to the force–length relationship (Herzog et al. 1990). A third trial was performed in case there was an increase from the first to the second trial of > 5%. A strap was fixed around the shank, perpendicularly connected with a non-elastic rope to a force sensor (2 kN; Biovision, Wehrheim, Germany). The applied forces were recorded at 200 Hz, then low-pass filtered with a second-order Butterworth filter and a 6 Hz cut-off frequency, using a custom-written MATLAB interface (version R2016a, MathWorks, Natick, USA). The maximum force value was determined based on a moving average with a time window of 50 ms. Resultant knee joint moments were calculated as the product of the force recorded during the MVC and the distance of the point of force application on the center of the strap to the lateral femoral condyle as the assumed location of the axis of rotation (Churchill et al. 1998). The moments were corrected for the moments of gravity of the shank and foot segment based on the participants’ anthropometry (Dempster 1955). The highest moment of the MVC trials represented the maximum strength of the knee extensors and was used for further analysis (both absolute moments and moments normalized to body mass).
Fig. 1
Mobile measurement system. The force generated during knee extensions at 60° knee joint angle (0° represents full knee extension) was recorded with a force sensor, which was oriented perpendicular to the shank. To calculate the forces exerted on the tendon, the measured forces were multiplied by the external lever arm of the applied force—specifically, the distance from the lateral epicondyle to the center of the strap attached to the shank—then corrected for gravitational moments and divided by the patellar tendon moment arm, determined through anthropometry. The elongation of the patellar tendon during contractions was recorded synchronously using ultrasound
Assessment of the patellar tendon force–elongation relationship and maximum strainTo determine the force–length relationship of the patellar tendon, five ramp contractions were performed in the setup described above, where the generated force was steadily increased from rest to 90% of the MVC within ~ 5 s. The participants received visual feedback of the target and generated force during the ramp contractions. The elongation of the patellar tendon during these isometric contractions was recorded using a 10 cm linear ultrasound probe (MyLab60; Esaote, Genoa, Italy; probe: LA923, 7.5 MHz; 25 Hz image frequency). For this purpose, the probe was fixed over the patellar tendon with a modified knee brace, mediolaterally centered and perpendicular to its longitudinal axis. In each trial, a manually triggered 5 Volt signal was simultaneously dispatched to both the MATLAB interface for force recording and the ultrasound device to synchronize the data during the subsequent analysis. For measuring tendon elongation, we quantified the displacement of the deep insertion sites of the tendon at the patella and at the tibial tuberosity, which was tracked with a semi-automatic software (Tracker Video Analysis and Modeling Tool V.4.92, Open Source Physics, Aptos, California, USA). For every trial, the tendon resting length was measured in the resting state prior to the contraction at best possible relaxation and equilibrium of moments, and then averaged over all trials. The slack of the tendon at rest was taken into account by calculating tendon resting length using a spline fit through the lower insertion points of the tendon and two additional markers along the deep peritendinous sheath (Mersmann et al. 2017). The maximum force applied to the tendon (i.e., maximum tendon force; TFmax) was determined based on the highest MVC trial of each participant. It was calculated by dividing the respective knee joint moment by the tendon lever arm, which was predicted based on anthropometric data (Mersmann et al. 2016) and adjusted to the knee angle of 60° (Herzog and Read 1993). The patellar tendon force–elongation relationship for each single ramp trial was saved as a piecewise-linear polynomial function in MATLAB (version R2019b; ‘interp1’ function with ‘pp’ option), using every measured data point of each ramp as input. To achieve a high reliability (≥ 0.95) and observer independence (Schulze et al. 2012) we averaged the five single force–elongation curves. Therefore, at each measured data point, all single ramp trials were evaluated using their respective piecewise-linear polynomials and then averaged (‘fncmb’ function in MATLAB). Then, on the averaged patellar tendon force–elongation curve, a second-order polynomial fit passing through zero (MATLAB function ‘polyfitZero’, version 1.1) was applied to obtain the final patellar tendon force–elongation curve for each participant. Patellar tendon stiffness was calculated as the quotient between 50 and 85% of TFmax from the polynomial function. Normalized patellar tendon stiffness was determined by multiplying tendon stiffness by its resting length (and reported in kN/strain), effectively representing the slope of the tendon force–strain curve, which is more robust against variations in tendon length. Maximum tendon strain was determined by extrapolating the tendon elongation to TFmax, using the polynomial fit of the force–elongation curve, and then dividing the maximum elongation by the tendon’s resting length.
Assessment of patellar tendon micromorphologyThe micromorphology of the tendon was estimated based on a spatial frequency analysis of ultrasound images as suggested by Bashford et al. (2008) of the proximal part of the patellar tendon (Mersmann et al. 2019). The assessment was conducted prior to the measurement of muscle strength and the tendon force–elongation relationship to minimize potential effects of acute tendon loading (Drongelen et al. 2007; Rosengarten et al. 2015). To remove tendon slack, yet not applying substantial forces to the tendon, participants were placed in a supine position with a 90° knee angle. A linear probe of the ultrasound system (LA523, 13 MHz, depth: 3.0 cm) was positioned over the patellar tendon parallel to its longitudinal axis and below the distal end of the apex patellae. Two sequences were recorded, and the images were analyzed using a custom MATLAB interface. A polygon, covering a length of 40% of the tendon’s resting length and the full thickness of the tendon, extending from the inferior insertion at the patellar apex to the midportion of the tendon was defined as region of interest (ROI). The maximum possible number of 32 × 32 pixel kernels within the ROI were analyzed by applying a 2D Fast Fourier Transform, followed by a high-pass filter with a radial frequency response and a half-power cut-off frequency of 1.23 mm−1. The filtered kernels were zero-padded in both dimensions to a size of 128 × 128 pixels and the average distance from the peak spatial frequency (PSF) of all kernels to the spectral origin in the frequency spectrum was used to evaluate the packing density and orientation of the collagen bundles. Low PSF values correspond to a less compact and isotropic speckle pattern in the ultrasound images, which is characteristic of tendinopathic tendons (Kulig et al. 2013) and may also be a consequence of high tendon strain (i.e., mechanical demand) in asymptomatic tendons (Mersmann et al. 2019, 2021). The average of the two recorded trials per participant was used for statistical analysis.
Personalized exercise prescriptionThe intervention group underwent a personalized exercise program throughout the competitive season, with the objective of promoting a balanced muscle–tendon adaptation. Dependent on the individual’s maximum patellar tendon strain, the loading program for the subsequent exercise phase (~ six weeks until the next diagnostic assessment) was selected as follows: If the maximum tendon strain (εmax) was below 4.5%, it was interpreted as an indication that the muscle had a strength deficit relative to the stiffness of the tendon. Consequently, the intention was to schedule a training that is considered more effective in increasing muscle strength than tendon stiffness. For example, performing medium-load contractions until muscle failure provides an effective stimulus for muscle hypertrophy (Mitchell et al. 2012; Burd et al. 2010), but does not promote tendon adaptation due to the low levels of strain during exercise and, thus, can induce a disproportionate increase of muscle strength compared to tendon stiffness (Lambrianides et al. 2024). However, none of the participants met this criterion at any time point during the intervention. Patellar tendon strains in athletes that fell within the intermediate range of 4.5 ≤ \(_}}}\) < 9% were classified as having a balanced relationship between muscle strength and tendon stiffness, while strains ≥ 9% indicated a relative deficit in tendon stiffness compared to muscle strength. In both cases, an isometric loading program was prescribed with a personalized relative load corresponding to 5.5% of tendon strain, as this falls within the range of strain effective for tendon adaptation (Arampatzis et al. 2007, 2010; Bohm et al. 2014). The relative load was calculated based on the assumption of a linear relationship between tendon force and strain, and limited to a maximum of 90% MVC (i.e., in participants with maximum strains between 4.5 and 6.1%), to ensure a sufficient number of loading cycles could be realized during training. Consequently, the prescribed relative load for the target tendon strains was low in athletes with high levels of maximum strain, which was thought to provide a stronger stimulus for the tendon compared to muscle when the loading volume and, thus, the level of muscular fatigue were low.
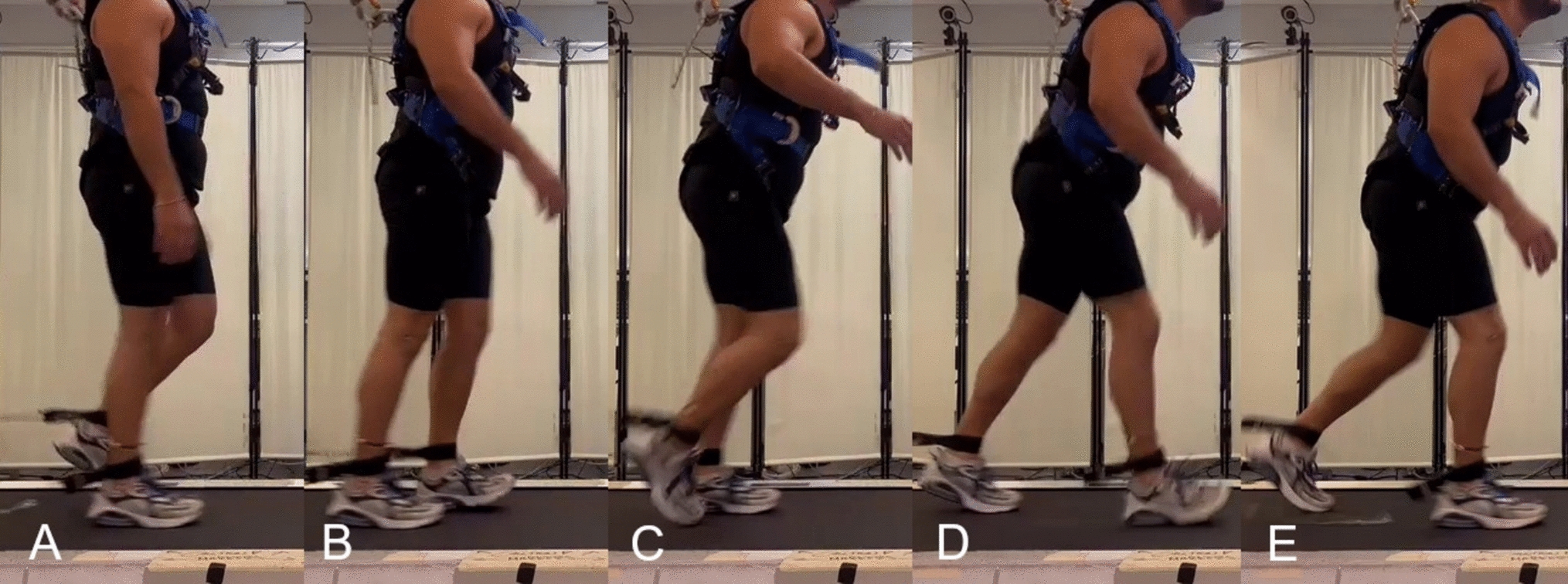
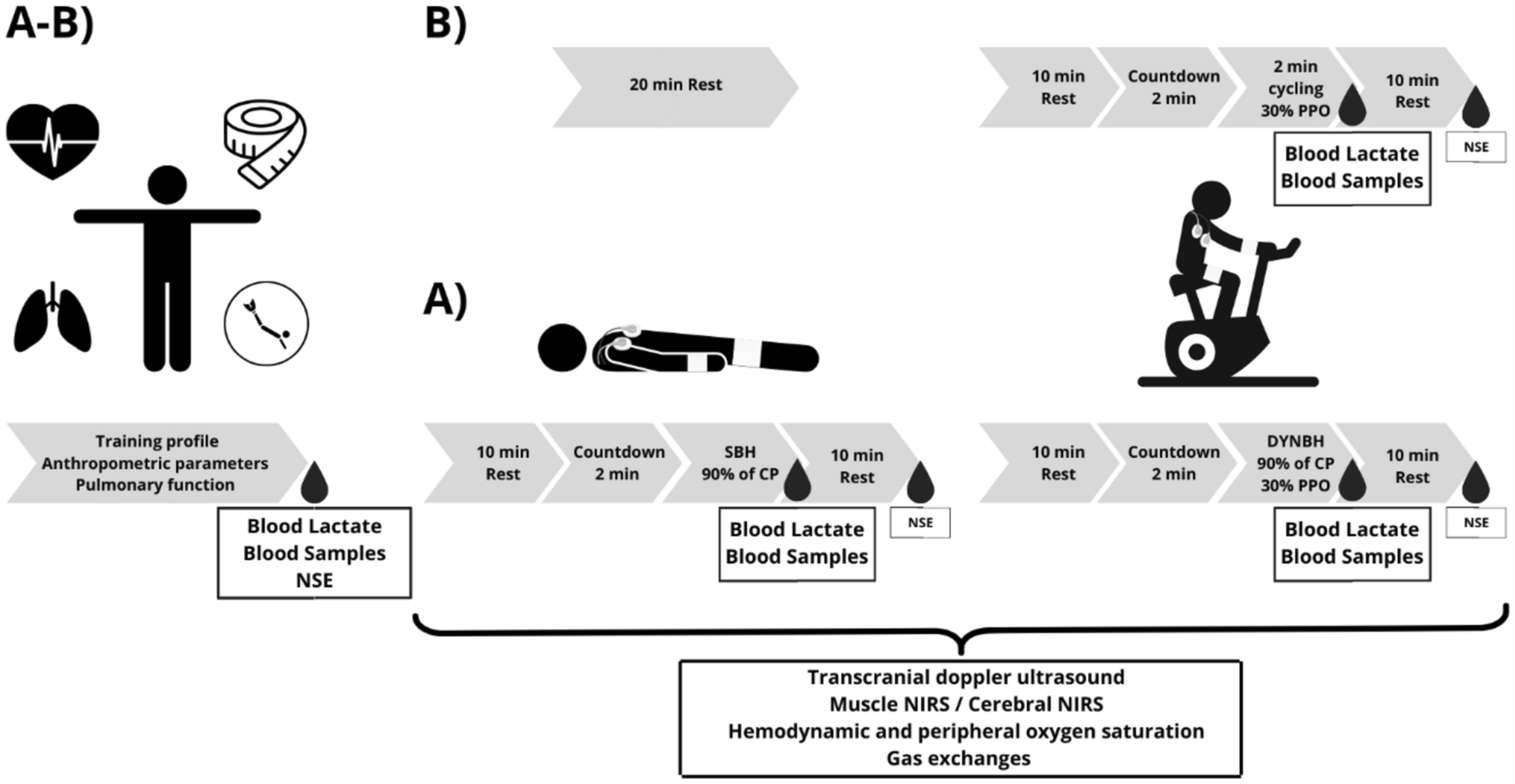
The isometric loading protocols were conducted using mobile training devices, which were designed to closely resemble the experimental setup of the main measurements to achieve the best possible consistency between the tendon strains achieved at a given relative load in the two settings (i.e., measurement and training). Accordingly, the devices consisted of a length-adjustable rigid band in series with a load scale, which was attached to the participants’ shank and allowed for real-time feedback of the applied forces during isometric knee extension contractions, which were performed at a knee angle of 60° as in the diagnostics (Fig. 2A). By performing an MVC in this specific training device to account for potential differences in the positioning of the point of force application and the orientation of the load scale with regard to the shank, each participant's individual absolute training load in this setting corresponding to the prescribed relative loading intensity (i.e., %MVC) was determined. Based on previous systematic research (Arampatzis et al. 2007, 2010; Bohm et al. 2014), the loading protocol then consisted of five sets of four isometric contractions. Each contraction was maintained for three seconds, followed by a three-second relaxation phase (Fig. 2B). The exercises were not performed additionally, yet incorporated into the athletes’ existing training schedule (i.e., as component within the regular and athletic training sessions) three times per week and were conducted on both legs at the same relative load. Adjustments of the absolute load (i.e., determination of a new MVC) were implemented every two weeks using the mobile training devices to account for increases in muscle strength. Intermediate diagnostics of muscle strength and tendon mechanical properties were carried out in addition to the regular measurements six weeks after M1 and M2 (note that M3 and M4 were only 6 weeks apart in the intervention group), to adjust the relative exercise load intensity based on the maximum strain of the patellar tendon. The actual strains corresponding to the relative loads were calculated retrospectively based on the individual force–strain curves.
Fig. 2
Training setup (A) and loading protocol (B) for the personalized tendon exercises. Isometric knee extensions were performed at 60° knee joint angle, with 0° representing full knee extension. A digital scale, attached to an adjustable non-elastic band, monitored the applied load. The personalized training load was derived individually from an MVC performed in the training device (updated every 2 weeks) and the relative load determined based on tendon strain determined at the main measurement time points and respective intermediate measurements
StatisticsThe statistical analyses were performed using R (v4.1.2, nlme package, R foundation for statistical computing, Vienna, Austria). A linear mixed-effects model (LMM) with restricted maximum likelihood estimation was applied to the investigated parameters. The standardized residuals were tested for normality using the Shapiro–Wilk test, and no violations were observed for any parameter. The LMM included the factor “group” (intervention and control) with group-specific y-intercept, slopes and variance of the residuals to examine time- and group-dependent developments. To account for variations in the time intervals between measurements across individuals and groups, the measurement time points were individually converted into weeks (from 0 to ~ 35 weeks.). Linear mixed-effects models are capable of handling missing data, which occurred in the present study due to participants not attending every measurement time point. The model equation was as follows:
$$_=_+__+__+___+_+__+_.$$
In this equation, \(i\) indexes the participants, \(j\) indexes the measurement sessions, \(_\) is a binary variable representing the group (0 for control group, 1 for intervention group), \(_\) is the time in weeks of the \(j\)-th measurement for participant i, \(_\) is the y-intercept constant for the control group, \(_\) is the slope constant for the control group, \(_\) is the difference in intercepts between the two groups, \(_\) the difference in slopes between the two groups, \(_\) is the participant-specific y-intercept (random effect), \(_\) is the participant-specific slope (random effect), and \(_\) is the residual. As the terms involving \(_\) are zero for the control group, \(_\) and \(_\) represent the intercept and slope for this group, respectively. For the intervention group, the intercept and slope are given by \(_+_\) and \(_+_\), respectively. This allows for testing the significance of changes over time in the control group (slope constant \(_\)), differences between groups at M1 (intercept constant \(_\)), and group differences in the time-dependent changes (slope constant \(_\); henceforth referred to as time-by-group interaction). The intervention group was separately tested for the difference in the slope from zero. To identify the individual deviations from linear development (i.e., fluctuations) for the relevant parameters, we additionally tested the residuals of the LMM as absolute values with regard to effects of group, time and time-by-group interaction. The associations of maximum tendon strain at M1 to the changes in maximum tendon strain (i.e., M4–M1) and the relative changes of normalized stiffness (i.e., (M4–M1) ⋅ M1−1 ⋅ 100) over the season were examined using the Pearson correlation coefficient (r). The anthropometric parameters (age, body height and mass) at the initial measurement time point (M1) and training age (i.e., years of volleyball training) were compared between groups using a t-test for independent samples. Additionally, the frequency of VISA-P scores with ≤ 87 points as a classification for symptomatic tendons was documented (Lohrer & Nauck 2011). The alpha level was set at 0.05 for all statistical tests.
Comments (0)