
Remember me



Patient characteristics are described in Table 2. In total, 143 patients underwent 167 coronectomies; 60% had a single coronectomy (n = 101), whereas 40% had bilateral coronectomies (n = 66). Majority of patients were female (78%, n = 131). Patients were aged from 17 to 91 years, with a mean age of 32. No relevant medical history was recorded for 94% (n = 157). One patient had well-controlled diabetes mellitus type 2 and one was taking low-dose systemic steroids. Twenty patients were smokers.
Table 2 Baseline characteristics: Patient DemographicsAssessment strategiesClinical indicationCoronectomy was undertaken for M3M affected by multiple episodes of pericoronitis in 84%, cyst or other pathology in 9%, caries in mandibular second molar (M2M) in 5%, risk of caries in M2M in 1% and caries in M3M in 1%.
Pulpal status of M3M was determined to be sound in 86% (n = 143), caries into outer third of dentine in 8% (n = 13), enamel caries in 5% (n = 8), internal/external resorption in 1% (n = 2) and one case of caries extending into outer but not into the inner third of dentine (no pulpal involvement).
The two cases of resorption were found to be successful on follow up, whereas the case of caries beyond outer third of dentine had no scheduled review but did not re-present with symptoms.
Summary of assessment strategies is presented in Table 3.
Radiographic assessmentAn OPT was taken for 95% of cases, whereas a periapical radiograph was used for the remaining 5% of cases as the baseline radiograph. Radiographic assessment identified one or more high risk signs as described by Rodd & Shehab [2] in 95% of cases treated.
A dental CBCT was undertaken for 78% of cases (n = 131). Out of the remaining 22% (n = 35) that did not have a CBCT, 57% (n = 20) declined it, 3% (n = 1) had bony separation present on OPT (thus, CBCT was not indicated). For 40% (n = 14) no information was given about the CBCT.
High risk signs on CBCT were present for 92% cases (n = 120) and 6% (n = 8) of cases lacked the classic ‘high risk signs’. The risk level could not be determined for 2% (n = 3) due to movement artefact or scan not available on the PACS XERO system.
Over 70% of the cases had more than one high risk sign detectable on a CBCT (Table 3). The following were recorded: interruption of cortication > 3 mm (n = 59, 29.8%), deformation of IAN in contact with roots presenting as dumbbell (n = 15, 7.6%), tear drop (n = 23, 11.6%) or other (n = 38, 19.2%), lingual IAN position (n = 32, 16.2%), inter-radicular IAN position (n = 24, 12.1%) and bifid IAN canal in contact with roots (n = 1, 0.5%).
In the cases without the classic ‘high risk signs’, the CBCT found the presence of bony separation (n = 4) and altered root morphology, such as root dilaceration (n = 1), hooked root (n = 2) and root apex ankylosis (n = 1). In these cases, patient-led informed decision directed the treatment choice (coronectomy versus surgical removal).
Table 3 Clinical and radiographic assessment of M3MTreatmentCoronectomy was undertaken under general anaesthetic (n = 133, 79%), local anaesthetic (n = 25, 15%) and operator-led intravenous sedation with midazolam (n = 10, 6%). Majority of bilateral coronectomies were undertaken under general anaesthetic (97%), with only 2 patients having bilateral coronectomy under local anaesthetic over 2 appointments.
Most surgeries were undertaken by Specialist Oral Surgeons (39%), followed by Specialty Trainees in Oral Surgery or Oral and Maxillofacial Surgery (26%). Consultants performed 15% of cases (Table 4).
Table 4 Treatment detailsPost operative complicationsSummary of post-operative complications is listed in Table 5.
Table 5 Summary of post-operative complicationsIntra-operative complicationsA total of 9 intra-operative complications were reported (5.3%), including: intra-operative failure (n = 8) and burn to lip (n = 1).
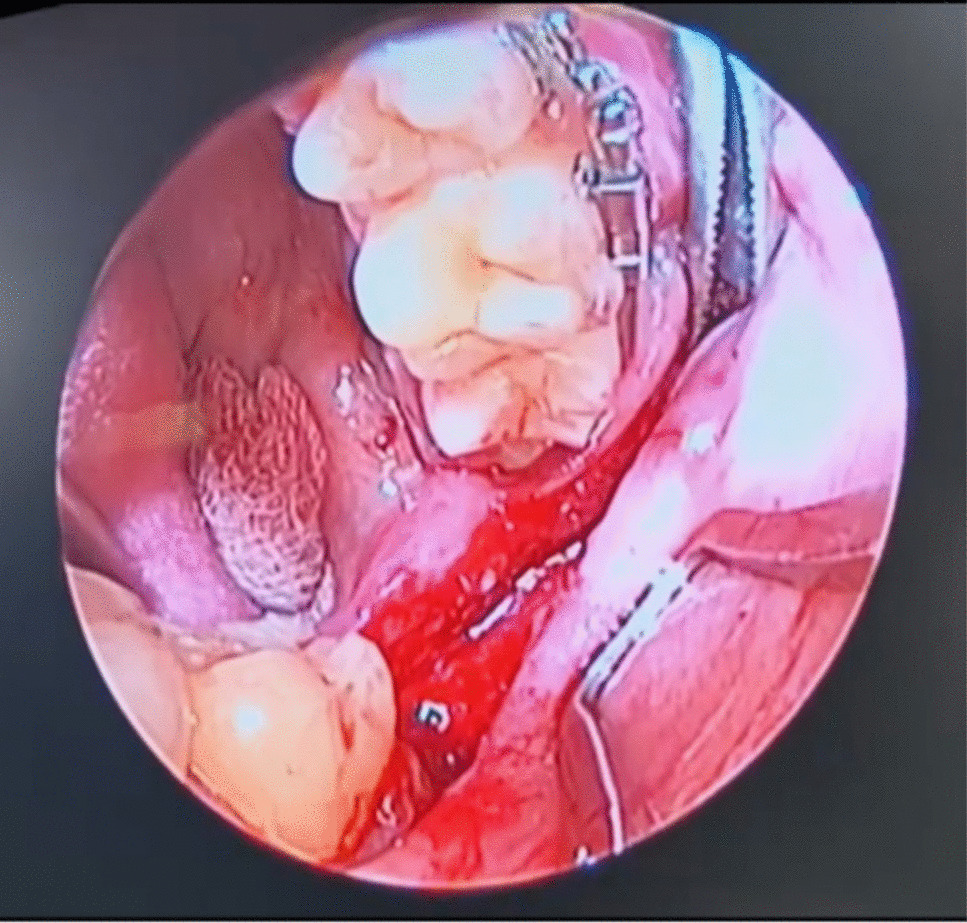
Intra-operative failure included intra-operative root mobility and the need for root removal (n = 5) (Fig. 1) or removal of a single root in a multi-rooted tooth (n = 1); and inability to remove enamel fully due to poor access (n = 2) (Fig. 2) The case depicted on Fig. 1(d) was associated with significant pus discharge and root mobility conforming the need for removal of the entirety of M3M. M3M associated with intraoperative failure had mesio-angular (n = 1), horizontal (n = 4) and vertical (n = 1) angulation and conical (n = 3), short (n = 2) and multi-rooted (n = 2) root morphology.
The rate of intra-operative failure where M3M root was removed was recorded as 3.6%. No patients in this group suffered temporary or permanent IAN or lingual nerve (LN) damage.
Fig. 1
Intra-operative failure where M3M root was removed during the procedure due to increased mobility, marked by arrow
Fig. 2
Pre-operative (a) and post-operative (b) orthopantomograms of Case 1
Pain/infection/dry socketPost-operative complications were recorded as pain 14% (n = 24), 9% infection (n = 15) and dry socket 3.6% (n = 6).
Pain was recorded as patient reported and not managed with self-administered analgesia. Optimisation of analgesia advice was provided. Supplementary analgesia was prescribed, if deemed necessary.
Infection was managed for most cases with oral antibiotics (n = 8), intravenous antibiotics (n = 1) or salt water mouth rinses (n = 1). Symptoms settled for all but one who was experiencing recurrent infections, thus, required root removal at 3 months post-surgery.
Dry socket was managed with Alvogyl dressing (n = 3), Alvogyl dressing and antibiotics (n = 2) and oral antibiotics (n = 1). One patient was experiencing persistent pain and had root retrieval at 3 months post-surgery.
Nerve injuryEight patients suffered a nerve injury, including both IAN and LN. Three patients had more than one site affected. A total of nerve injuries was recorded as 12; 9 temporary (2 IAN – 1.2%, 4 LN – 2.4%, 3 site not specified – 1.8%) and 3 permanent (2 LN – 1.2%, 1 IAN – 0.6%). The details of all nerve injury cases are outlined in the Table 6.
Table 6 Case details of nerve injury (MA = mesio-angular, TI = transverse, DA = distoangular, VI = vertical, N/R = not recorded, N/A = not applicable)Case 1A 38-year-old male patient underwent bilateral coronectomies of deeply impacted right and left M3Ms, both associated with a cyst, performed under GA. The right M3M was deeply impacted and mesio-angular (Fig. 2a). The IAN was passing lingual to the apices of M3M, associated with narrowing and deviation. The right M3M demonstrated signs of ankylosis. The left M3M was disto-lingually positioned and deeply impacted with IAN running at the coronal level of the M3M lingually. Access and visibility were described as ‘limited’. A lingual flap was raised and a ‘Howarth’s’ retractor was used for lingual nerve protection of the lower left M3M. Crowns of both M3Ms could not be predicably sectioned and enamel remnants were retained (Fig. 2b). The patient experienced dysaesthesia of right IAN and anaesthesia of left LN. Intra-oral healing was otherwise unremarkable, with full mucosal closure. No evidence of communication or infection were present. Re-operation and removal of retained enamel fragments were considered but thought not to benefit the patient, thus, were not undertaken. The patient was followed up for a duration of 10 months and discharged with persistent right IAN dysaesthesia and fully recovered left LN. Three years passed since the procedure completion. At the time of publication, the patient was not known to experience any issues relating to retained enamel fragments and accepted the status of nerve damage.
Case 2A 30-year-old female underwent a coronectomy of left M3M for chronic pericoronitis. The M3M was vertically impacted. No bony separation between the root and the IAN canal was confirmed on a CBCT. A lingual flap was raised and lingual retraction was used during surgery. Post-operatively, the patient experienced initial paraesthesia and developed complete anaesthesia of left LN within 12 months of the surgery. The patient was referred for LN repair at a specialist unit resulting in successful outcome and improvement of numbness. The patient remains under follow up.
Case 3A 40-year-old male underwent a coronectomy of right M3M for chronic pericoronitis. The M3M was mesioangular demonstrating darkening of roots and deflection of the IAN canal on OPT (Fig. 3). CBCT confirmed lingual position of the IAN canal that was deviated and significantly narrowed. No lingual retraction was used. Post-operatively, the patient experienced paraesthesia of right LN and altered taste. The patient was followed up for 12 months, accepting of the injury as ‘permanent’ and was discharged.
Fig. 3
Pre-operative (a) and post-operative (b) orthopantomograms of Case 3
Notably, an enamel fragment was retained mesially (Fig. 3b). Full mucosal healing was achieved and no post-operative infection was recorded. The procedure was performed by a junior staff member, likely conforming a technique resulting in incomplete enamel removal.
There could be a number of theories for LN injury in this case. It is unlikely that retained enamel is the culprit. However, attempts to section the tooth resulting in lingual plate breach could be a factor in mechanical LN injury. No investigations, such as CBCT, were available to confirm this deduction. Finally, a possible mechanism of LN injury also includes a poor IAN block technique under GA.
Re-operationThe reoperation rate was 1.8% as 3 patients required removal of M3M root (Table 7). Two patients underwent root retrieval at 3 months following coronectomy without the evidence of root migration (Fig. 4(a) Case 1; (b) Case 2). Both patients recovered fully and did not experience temporary or permanent IAN injury. One patient required surgical removal of M3M retained roots 2 years after coronectomy. Root migration was noted on radiographs, highlighting successful outcome and the intent of the procedure (Fig. 4(c) Case 3). No post-operative IAN injury was recorded.
Table 7 Clinical details of re-operation cases. (F = female, N/R = no relevant; HI = horizontal, DA = distoangular, VI = vertical; ST = specialty trainee, SPD = specialty dentist)Fig. 4
Orthopantomograms of cases requiring re-operation. (a) Case 1, (b) Case 2 (c) Case 3 demonstrating root migration
Follow up protocolOverall, 15% of post-operative coronectomy cases presented with an acute issue within 1–2 weeks following the surgery. 82% of coronectomy cases had a scheduled follow up appointment. 19% of cases presented prior the scheduled appointment. Out of those who did not have a scheduled follow up, 7% presented acutely.
Success of coronectomyThe outcome of coronectomy can be determined as a factor of surgical outcome, presence or absence of permanent IAN injury, persistent symptoms or any other long-standing complications (such as LN injury), and the need for re-operation considering root migration status (Fig. 5). The flowchart accounts for total rate of complication, and success is considered in the absence of these (Success rate = 100% - total % of complication).
Fig. 5
Coronectomy success assessment tool. Success rate = 100% - total % of complication (* = discounted from total complication rate)
The complication rates in our study are applied in the flowchart in Fig. 5. In our instance, the rate of persistent symptoms and re-operation rates represent the same cases. Re-operation where root migration was evident carries a low risk of IAN injury. Cases falling into this group are given a successful outcome, thus, were discounted from the total complication rate (*). In this study, the successful outcome of coronectomy was 93%.
Comments (0)