Early diagnosis and contemporary advances regarding cancer treatment modalities have increased the 5-year survival rate of childhood cancer survivors. This is related to an increasing percentage of children that present with at least one late effect in any organ because of the disease and its treatment (Oeffinger et al. 2006; Blaauwbroek et al. 2007). The effects on dental tissues and the craniofacial complex are detrimental and can cause anatomic, functional, and aesthetic sequelae, as they affect occlusion and facial development. Therefore, early diagnosis, detection of the defects and their long-term monitoring is essential for effective treatment planning to reduce the side-effects of cancer treatment. In addition, counselling of the patient and their caretakers is also very important to improve their quality of life.
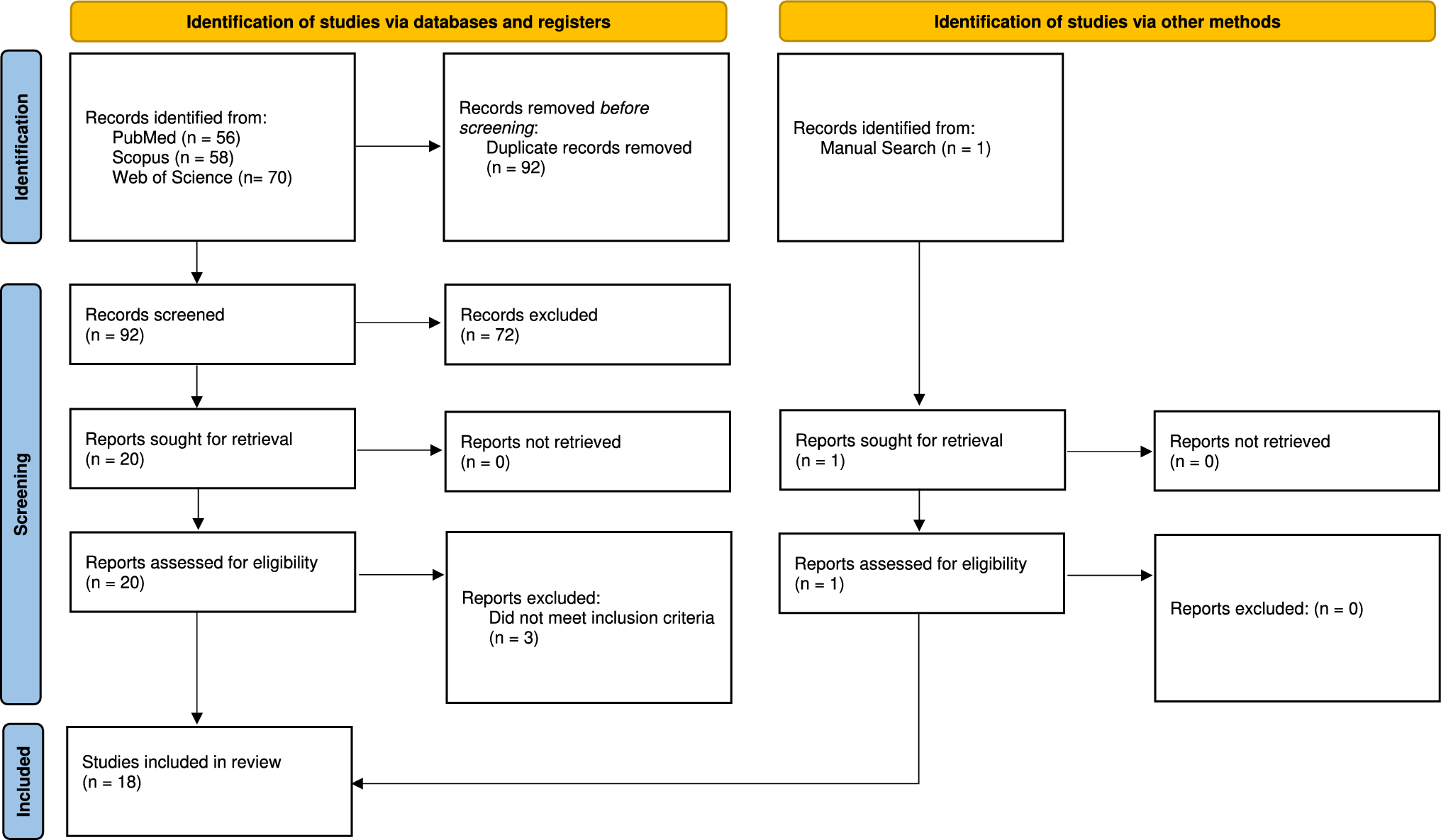
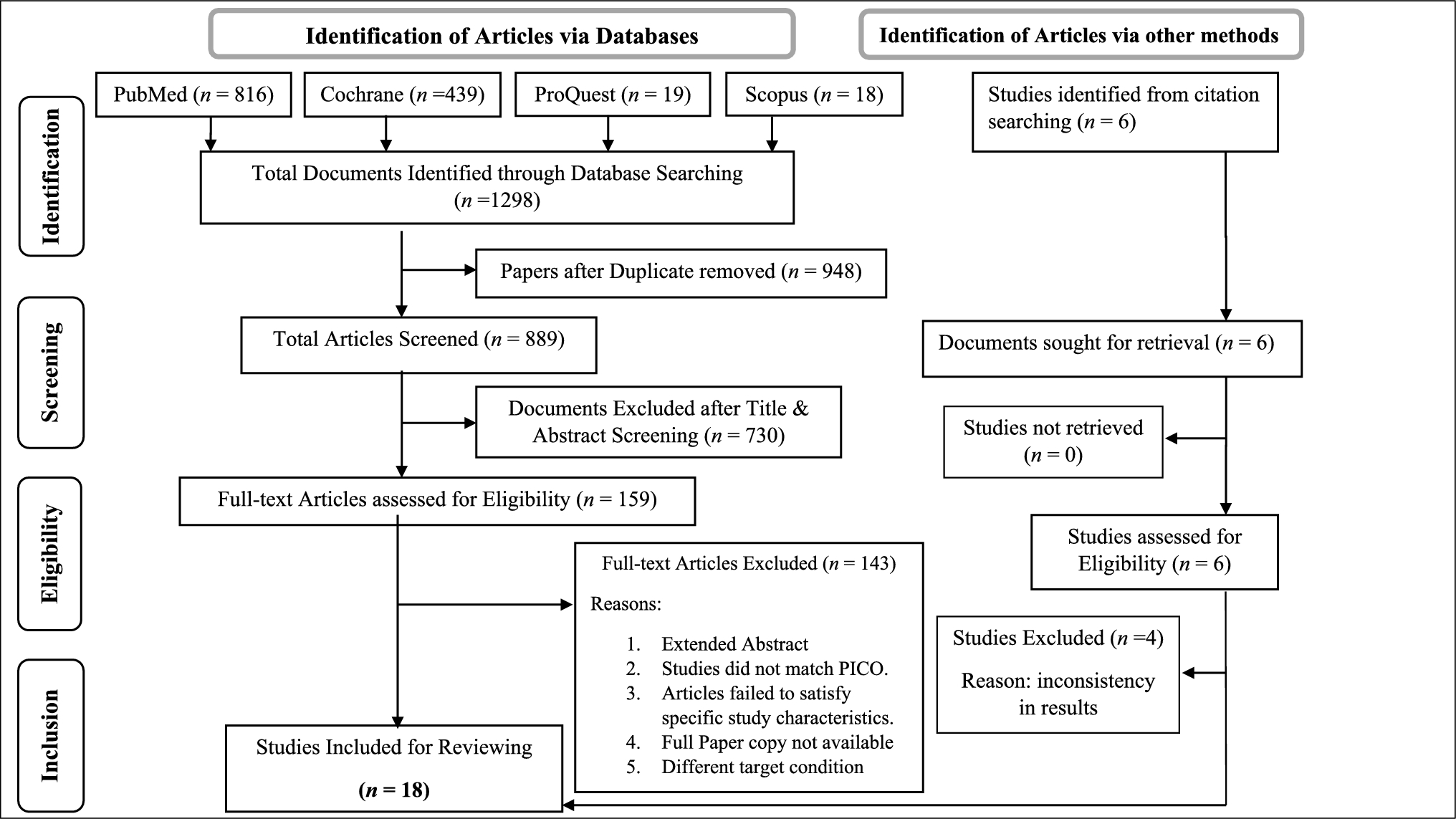
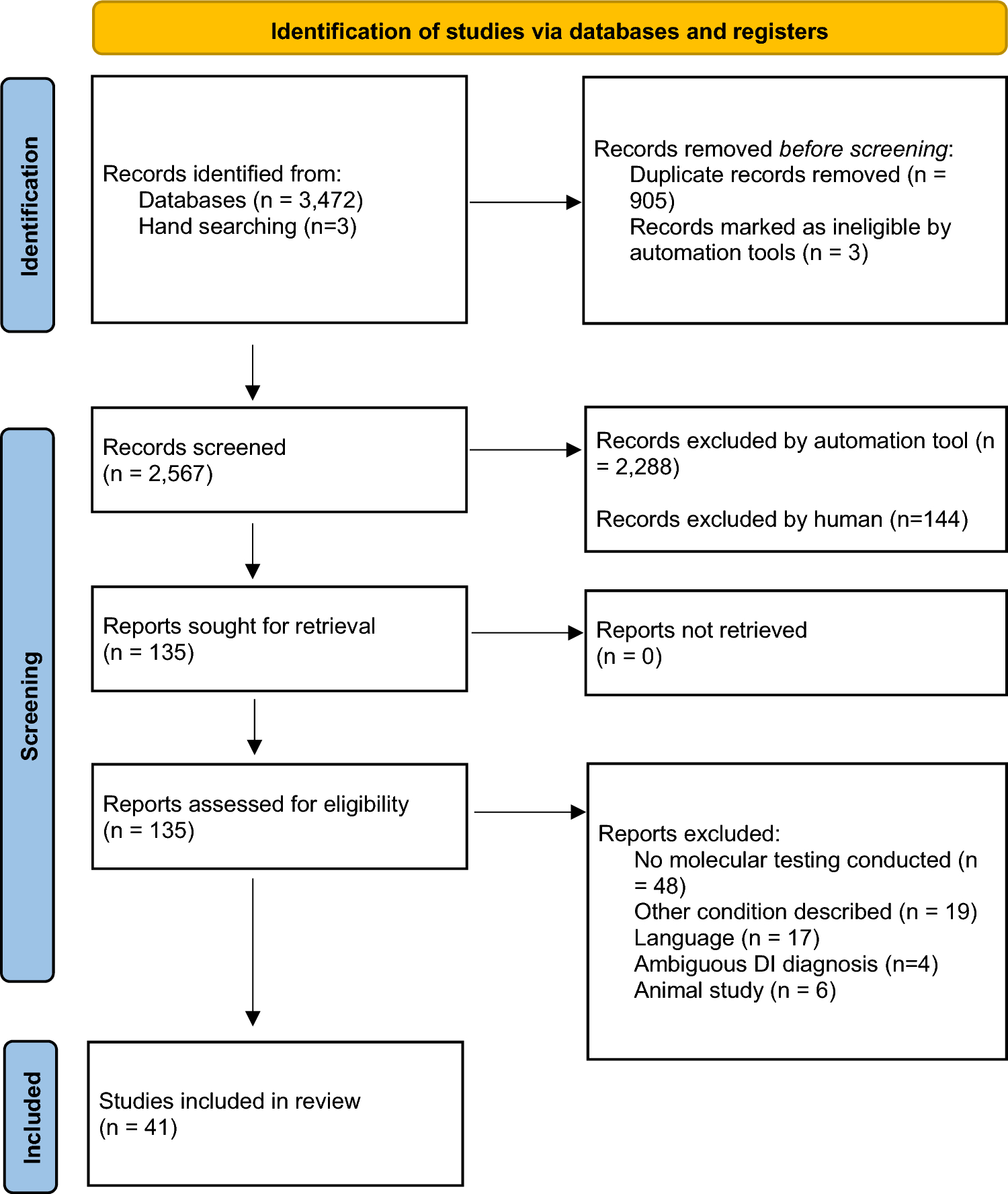
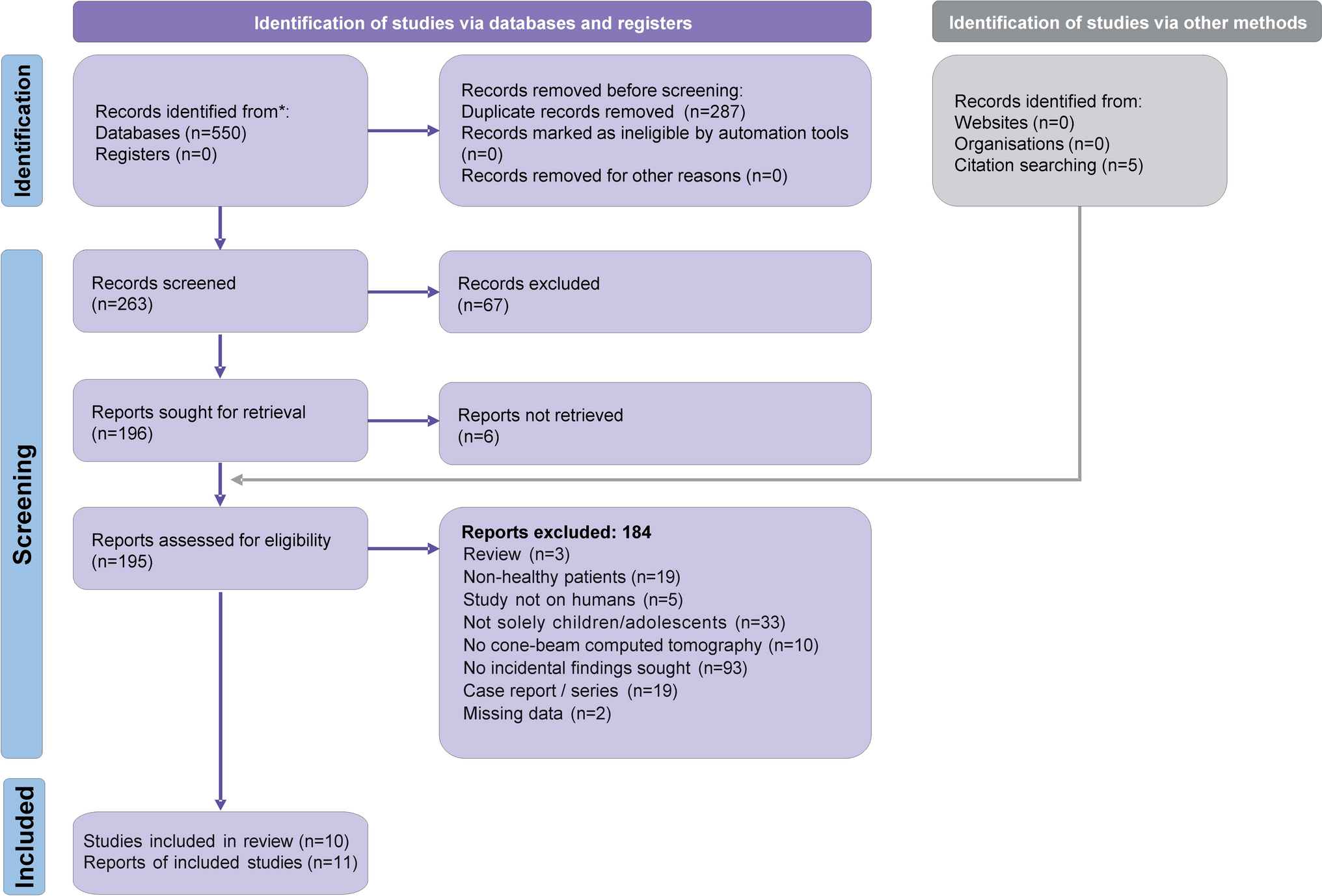
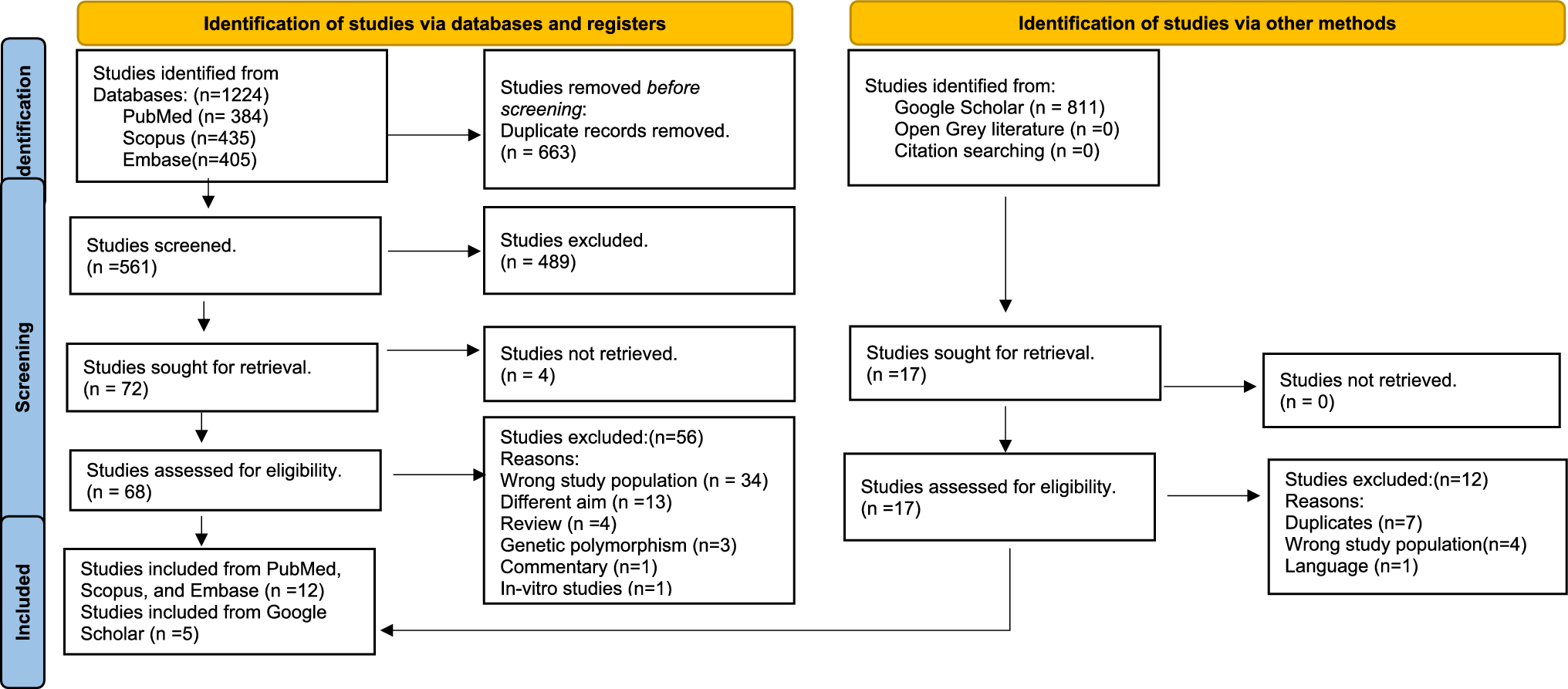
The aim of this systematic review was to summarise the existing knowledge on prevalence of oral, dental, and craniofacial side-effects of antineoplastic treatment in CCS in the context of paediatric dentistry. Seventeen retrospective cross-sectional and case–control studies published from 1994 until 2022, were included from the retrieved studies, yielding a total of 983 CCS that were examined clinically and radiographically for any dental adverse effects and compared with 1266 healthy age and gender matched controls. The main finding of this review was that the prevalence of both clinical as well as radiographical dental late defects were very high among childhood cancer survivors compared to healthy controls. Overall, one third of CCS experienced at least one late effect, with corresponding value for the control group being below 25% in most cases. Root abnormalities and agenesis were the two most common defects recorded among all patients examined.
Specifically, regarding oral health three studies reported that CCS are more likely to develop dental caries (Wogelius et al. 2008; Proc et al. 2019; Patni et al. 2023), as mean dmft/DMFT value for CCS was higher when compared to the healthy controls. This is in accordance with the findings from previous studies recording worse clinical indices for CCS (Pajari et al. 1995; Singh et al. 1996; Avşar et al. 2007; Proc et al. 2019). Higher dmft/DMFT scores in CCS may be the effect of reduced salivary secretion and of the microbial shift towards a more cariogenic microflora (Seremidi et al. 2023; Gawade et al. 2014). Furthermore, precious studies also showed that younger patients who receive high doses of radiation are at increased risk of developing tooth decay (Jaffe et al. 1984; Pajari et al. 1995; Kaste et al. 1997; Seremidi et al. 2023). In this review, one study demonstrated a positive correlation between radiation therapy and dental caries (Cubukçu and Sevinir 2008).
Similarly, oral hygiene and gingival indices were worse in CCS, findings that is in accordance to a recent review, presenting increased plaque accumulation and gingivitis for these patients as compared to controls (Busenhart et al. 2018). Researchers associated it with specific phases of the antineoplastic treatment, where patients with low thrombocyte levels are refrained from toothbrushing to avoid bacteremia (Lockhart et al. 2008). Although this discontinuation of toothbrushing is not shared by other researchers, who support that patients should be able to perform oral hygiene procedures without bleeding at widely different levels of platelet counts (da Fonseca 2004).
Prevalence of oral health indices can be affected by confounding factors that cannot be controlled (e.g. frequency and efficiency of brushing, sugar consumption, saliva quality and quantity, etc.) and therefore, the association with specific treatment characteristics is not clear. It is certain that the alterations caused by the antineoplastic medicaments administered during treatment can affect the incidence, but the direct relationship and the degree of the effect cannot be justified, underlying the necessity for proper specialised oral counselling during all stages of treatment.
Late clinical dental developmental defects were documented in 11 studies. In CCS, discolouration was the most common defect followed by microdontia, hypodontia, and enamel disturbances. The overall prevalence of late clinical defects in controls was low. Enamel developmental defects, detected clinically as enamel opacities, are caused by alterations in ameloblast reproduction during tooth formation expressed by secretory function, membrane permeability, and calcium exchange across the cell membrane (Goho 1993). Because of the short half-life of most chemotherapeutic agents used, defects are caused by changes in the function of odontoblasts rather due to their death and are therefore more localised (Avşar et al. 2007).
Defects recorded radiographically were reported in 11 studies and showed that arrested root development was the most prevalent defect followed by agenesis and delayed eruption. The corresponding prevalence in healthy controls was much lower. The range of prevalence of agenesis was less wide in both CCS and healthy controls. However, the percentage of the latter was low. Previous studies have shown that dental development defects, including microdontia, oligodontia, hypodontia, enamel defects, and root malformations, can occur in CCS (Kilinc et al. 2019; Tanem et al. 2022; Halperson et al. 2022; Seremidi et al. 2023). The prevalence of these defects may depend on the type of cancer and the treatment received. Radiation therapy can significantly impair tooth development (Blaauwbroek et al. 2007; Collett and Thonard 1965). The effects of chemotherapy on tooth development still need to be elucidated due to its multi-drug nature and possible differences in the cytotoxic effects of individual chemotherapeutic agents (Jodlowska et al. 2022).
Incidence and severity of these defects depend on risk factors associated with the specific features of antineoplastic therapy. Such a risk factor is age at diagnosis, which is directly related to the stage of tooth development, type, and duration of treatment, absorbed dose and radiation field (Scully and Epstein 1996; Cheng et al. 2000; Seremidi et al. 2019).
Six of the included studies evaluated potential correlations between defects and specific disease and treatment characteristics. For diagnosis Kilinc et al. (2019) and Näsman et al. (1994) reported no effects on crown defects. Proc et al. (2016) reported a positive correlation between age at diagnosis and the presence of microdontia, consistent with Bagattoni et al. (2014) who reported an increased risk of microdontia, aplasia, and root defects in patients treated with doses > 20 Gy.
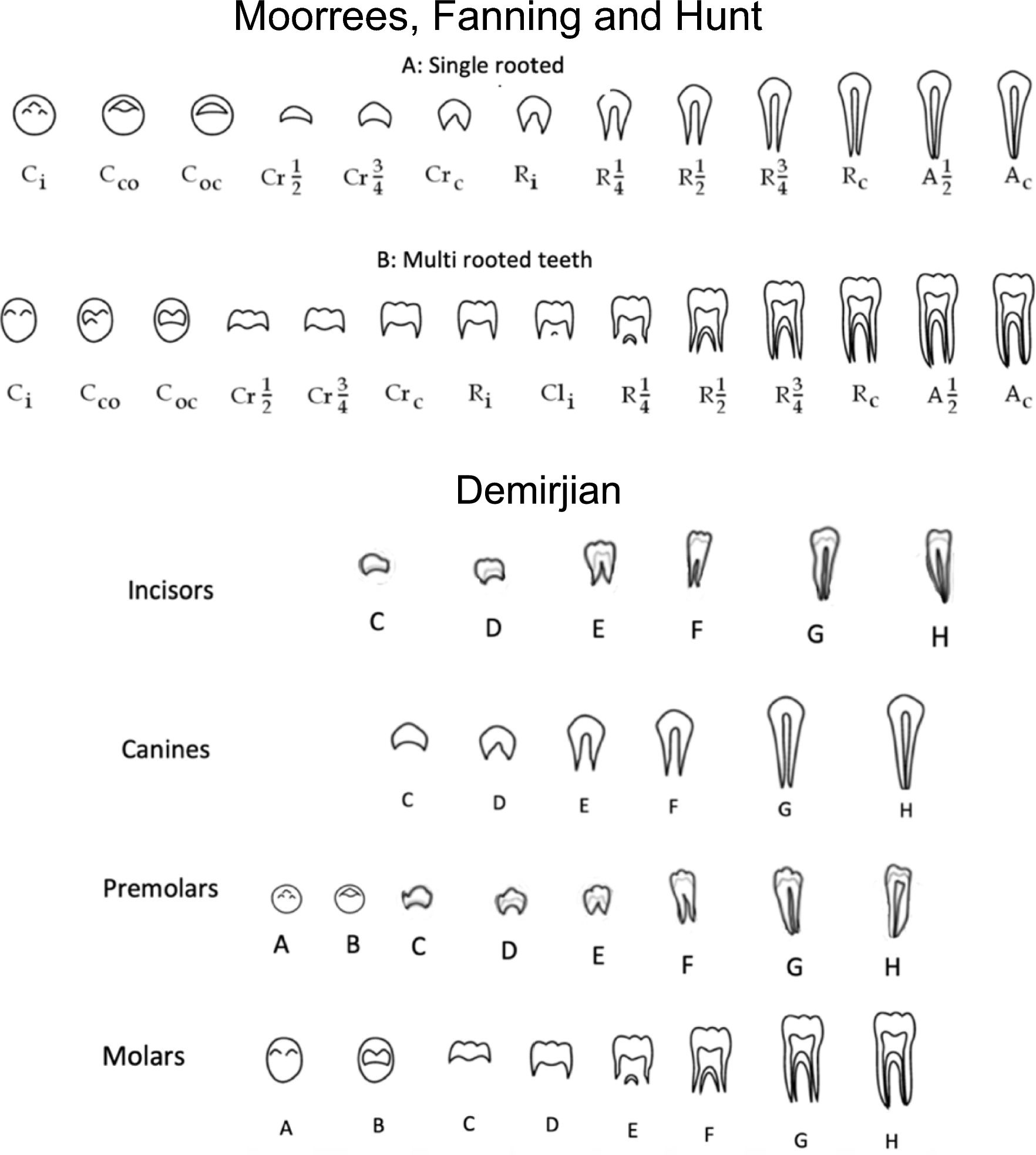
Cancer therapy can have an impact on dental maturity although how dental maturity is influenced by cancer therapy remains unclear and this reflects the results of the included studies in this systematic review. Dental maturity was assessed in four studies, and investigators documented the significance of deviations in dental age and chronological age within study groups and between study and control groups. The results from the included studies are contradicting since two studies overestimate dental age and two underestimate (Mitsea et al. 2022; Proc et al. 2021; Flores et al. 2015; Bagattoni et al. 2014). The same researchers both overestimate and underestimate dental age for the control group, respectively. Newer evidence supports that there is only small correlation between dental maturity and physical development, with the former only slightly related to skeletal maturation and craniofacial growth (Kanbur et al. 2006).
Saliva production and secretion are important for maintaining a good oral health and function. Therefore, complications resulting from salivary dysfunction such as caries, increased difficulty in swallowing, chewing and speech, can lead to an impaired quality of life. In this systematic review two studies reported the effect of anti-tumour treatments on salivary gland function. Nemeth et al. (2014) reported a lower saliva flow rate (stimulated and unstimulated) in CCS compared to controls. In the same study, 18% of CCS had moderate buffering capacity and 82% had high buffering capacity, whereas 57% of controls had moderate buffering capacity and 40% had high buffering capacity. In a study by Näsman et al. (1994), the unstimulated saliva rate was lower in patients that had stem cell transplantation and received radiation therapy compared to healthy controls and patients only receiving chemotherapy. No difference was seen regarding salivary pH between chemotherapy-treated patients and those who underwent stem cell transplantation and radiation therapy.
Regarding, secondary outcome only one study (Shum et al. 2020) reported oral health-related quality of life. Participants with agenesis had a significant higher mean value on the Oral Health Impact Profile compared to those without agenesis indicating a worse OHRQoL. Also, patients that presented with microdontia were more likely to report “Fairly Often” and “Very Often” in more than 1 domain of the profile, although no statistically significant differences were calculated for counts of “Fairly Often” and “Very Often” reporting with any of the dental late effects. In another study (Wogelius et al. 2011), results show that children with cancer rate their OHRQoL better or equal to those without cancer and that cancer and cancer treatment during childhood is not associated with a decreased OHRQoL. Stolze et al. (2020), reviewed the impact of haematological malignancies on OHRQoL in both adults and children. No robust conclusions could be made regarding the global OHIP-14 score but among OHIP-14 domains, functional limitations and physical pain were given the highest score while social handicap and social disability were given the lowest (Stolze et al. 2020).
Finally, head and neck cancer can lead to physical, physiological, and social problems such as craniofacial deformities in patients (Pertschuk and Whitaker 1985). To solve these problems, depending on the patient's condition, the dentist may consider orthodontic and prosthodontic treatment with surgical intervention. Long-term follow-up of oral rehabilitation was evaluated in six case reports, including nine CCS with severe dental sequelae after cancer treatment (Liu et al. 2021; Kotsiomiti et al. 2013; King 2019; Michalak et al. 2019; Zwetchkenbaum and Oh 2007; Chang and Lin 2021). The dental sequelae reported in the nine case reports were dental caries, root abnormalities, aplasia and underdevelopment of the maxilla and the alveolar ridge. In some case reports, periodontal disease has also been noted. In most case reports, restorative treatments combined with prosthetic rehabilitation were chosen to improve function, preserve bone structure, and improve aesthetics. Dental implants and implant-supported dentures were also used in many case reports of young survivors. Note that prostheses reported in young survivor case reports were a form of interim solution, as they were sometimes replaced to accommodate growth.
Concerning orthodontic treatment, the conclusions are ambiguous, as in two case reports (Chang and Lin 2021; King 2019) the authors suggested that such treatment was contraindicated. In a third case report, the malocclusion was treated with orthodontics (Kotsiomiti et al. 2013). However, when treatment was contraindicated, the patient showed severe root defects or agenesis in combination with an underdeveloped alveolar ridge. Long-term follow-up of patients revealed progressive effects of disease and its treatment, making oral rehabilitation difficult.
Strengths and limitations
The review tried to present an evidence-based overview of the defects associated to cancer and its treatment in the craniofacial complex with its major strength being the strict inclusion criteria imposed and its broad spectrum of defects assessed in a relatively homogenous manner. Adding evidence to the three previous systematic reviews it attempted to report importance of paediatric dentists in the oncology team, especially during the active cancer treatment to manage acute complications but also when late-stage complications occur.
However, results should be interpreted with caution before any specific conclusion can be drawn due to limitations of the included studies. Language and study design, with a non-randomised sample increases risk of selection and reporting bias. Case–control studies are generally considered to have a higher risk of bias than cohort studies since cases and controls may not have equal opportunity to determine exposure, making these types of studies susceptible to selection and recall biases. The same applies to cross-sectional studies. This can lead to various biases in meta-analyses of case–control, cross-sectional and cohort studies.
Limited comparisons between the included studies could be made due to the heterogeneity of the samples included both regarding disease diagnosis (type and stage of cancer) and treatment characteristics (treatment protocols, duration of treatment, stem cell transplantation). Also, included studies were observational, presenting the subjective perception of each researcher due to the lack of specific indices to categorise and quantify the defects further increasing the risk of overreporting. Finally, pre-existing defects and confounding factors, factors that play a crucial role in the outcome, were not controlled in the included studies.
Future research
Advanced research should focus on correct screening and early identification of survivors at risk for developing dental late defects. Further evidence is needed to investigate dental late effects, both regarding prevalence and severity, as well as associated risk factors among survivors.
The beneficial effect of individualised pre-screening and preventive dental care must be investigated. Pre-treatment evaluation, evaluation at the end of antineoplastic treatment and long-term monitoring of survivors will allow for more clear conclusions on the effects of treatment on dental structures. Early screening and education of parents and health care providers should aim at improving survivors’ perceived quality of life.
Future studies should also focus on the relationship between specific aspects of HRQoL and disease and treatment-related factors for overall well-being to be achieved. Given that the effects produced by the disease and its treatment vary in extent and severity, it is important to identify the domains that are mainly affected and to achieve satisfaction in those that are important to everyone. Finally, investigation of the empirical relation between physical and psychological variables of HRQoL and cancer survivorship, could contribute to the development of effective psychosocial interventions.
The long-term progression of these defects should also be evaluated. Furthermore, the effect of different oral care and dental treatment protocols on the defects to offer evidence regarding long-term stability through specific guidelines for the long-term follow-up of these patients should be evaluated.
Finally, dentists’ and other healthcare providers knowledge on survivor’s dental care should be assessed, underlining the importance of the multidisciplinary approach and the early and precise involvement of the dentist in the oncological team.


Comments (0)