
Remember me






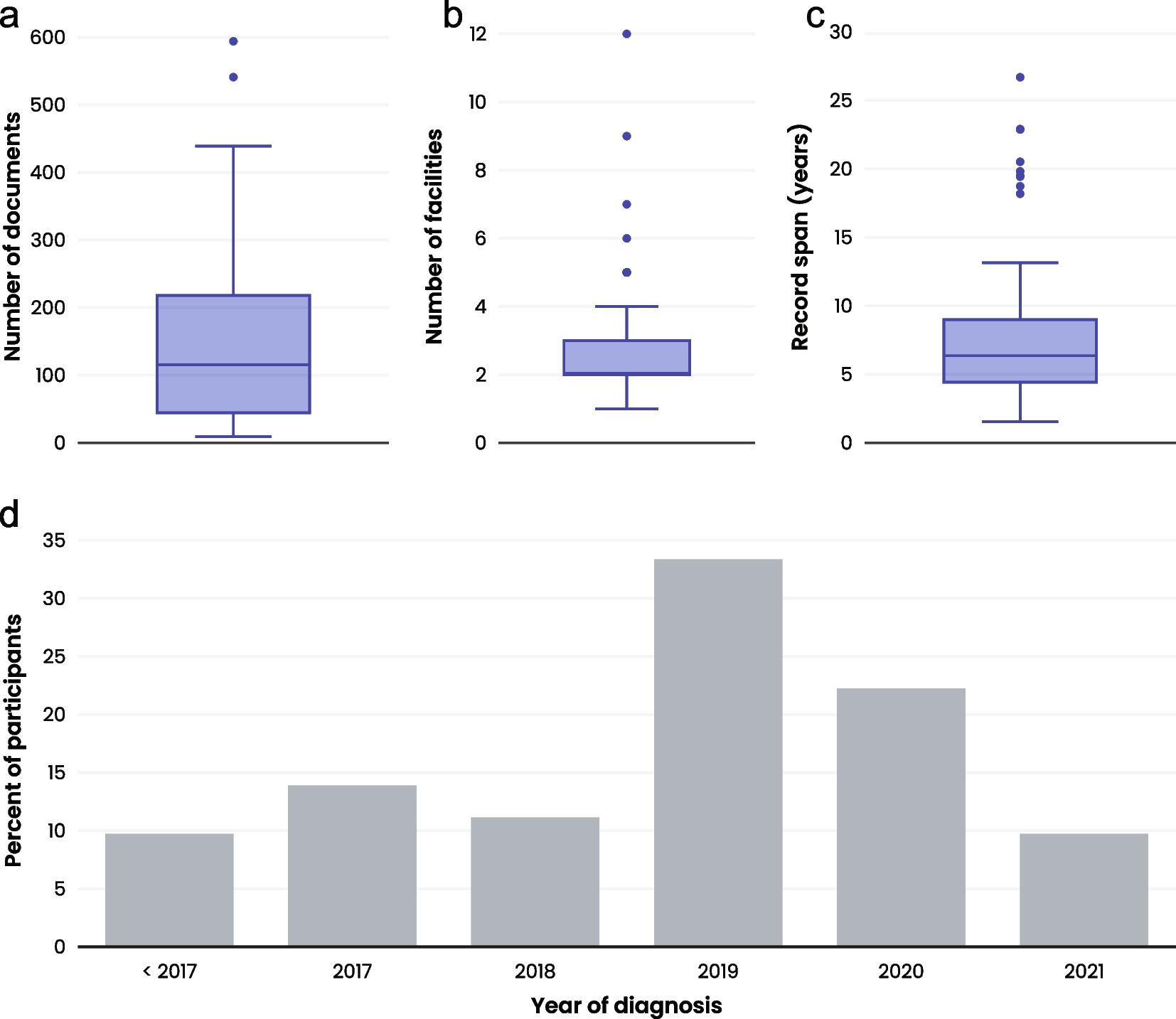

We included 70 patients in the study, including 42 males (60%) and 28 females (40%), with a 1.5:1 male to female ratio. The median age at diagnosis was 36 years (18–69), and the median duration from symptom onset to diagnosis was 2.0 months (0–50.0). The proportion of patients who underwent full body CT scans at diagnosis was 84.3% (n = 59), and FDG-PET was 51.4% (n = 36), and MRI brain was 27.1% (n = 19). All the patients underwent at least one full body radiological examination. Among the entire cohort, 68 patients (97.1%) had clinical manifestations leading to diagnosis (Fig. 1). The most common clinical manifestations were bone pain, accounting for 41.4% (n = 29), followed by nonspecific soft tissue masses 8.6% (n = 6), diabetes insipidus 7.1% (n = 5) and lymph node enlargement 7.1% (n = 5). Three patients had anorexia (4.3%). Gonadal dysfunction and weight loss were present in two (2.9%) patients each. Fever, rash, jaundice, and hearing impairment were found in one (1.4%) patient each. The most commonly affected organs were the bone, accounting for 70.0% (n = 49), followed by pituitary gland 7.1% (n = 5), lymph nodes 5.7% (n = 4), skin 4.3% (n = 3), liver 4.3% (n = 3) and thyroid 1.4% (n = 1). Other affected organs included eyelid, submandibular gland, parotid gland, digestive tract and epidural mass in one case each (Table 1). It is worth mentioning that we described three patients with unifocal liver involvement, and their liver enzymes were as follows: alanine aminotransferase (ALT) range 22–82 U/L, aspartate transaminase (AST) range 21–64 U/L, alkaline phosphatase (ALP) range 112–260 U/L, γ-glutamyl transpeptidase (GGT) range 75–335 U/L, total bilirubin and direct bilirubin were normal.
Fig. 1
Percentage of clinical manifestations of adult patients with unifocal LCH
Table 1 Demographics and clinical characteristics of adult patients with unifocal LCHPast and family medical historyOf the 70 patients, two had a history of previous cancer. One patient with skin involvement LCH had thyroid cancer that had been surgically removed before the diagnosis of LCH. Lung adenocarcinoma was found in one patient at the time of diagnosis of bone-involved LCH. Twenty-five patients (35.7%) had a smoking history, and the median smoking index was 8.1 pack-years (2.4–75.0). None of the patients had a family history of LCH or other histiocytic tumours.
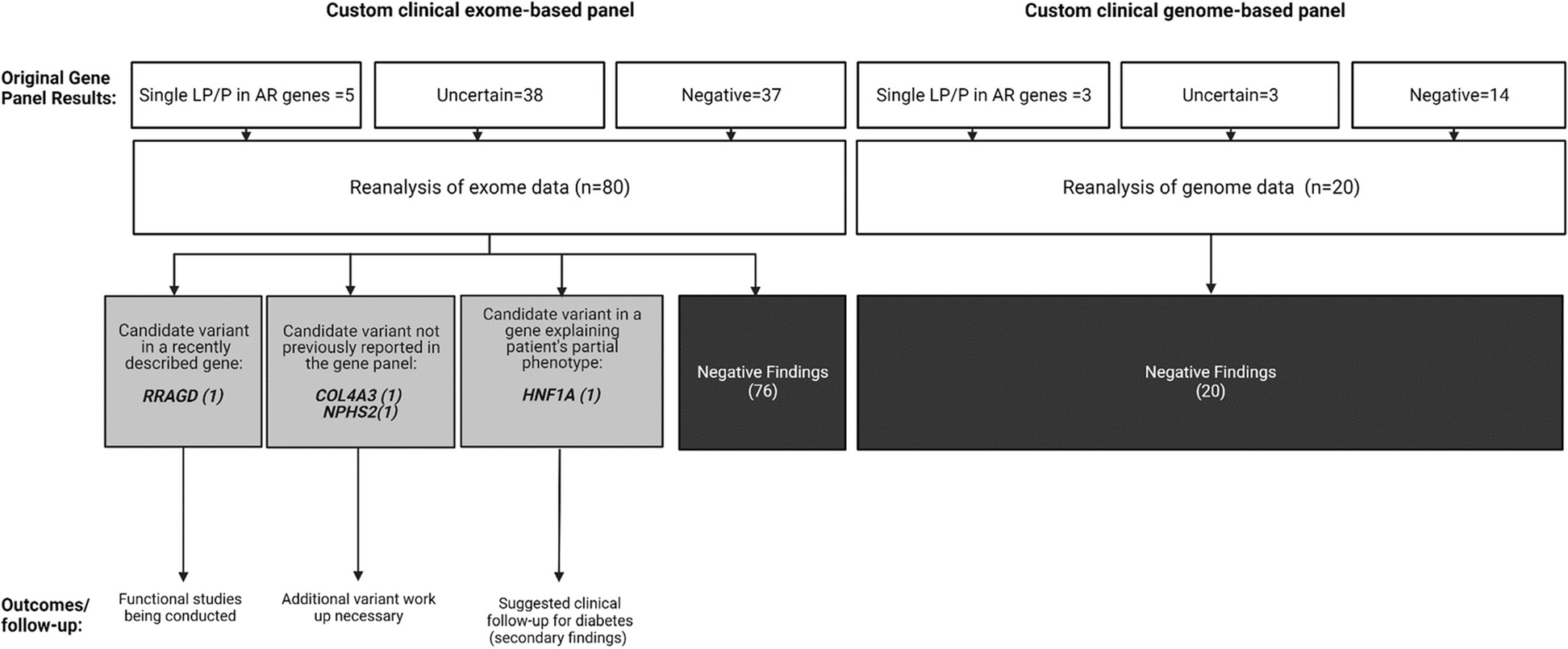
Genomic profilingTarget gene sequencing of lesion tissues was performed on 32 of the 70 patients (Additional file 1: Table S2). Five patients had no mutations, including two bone, one lymph node, one skin and one liver involvement. MAPK/PI3K pathway alterations were present in 78.1% of the patients (n = 25). The frequencies of BRAFV600E mutation, MAP2K1 mutation and PIK3CA mutation were 28.1% (n = 9), 18.8% (n = 6) and 9.4% (n = 3), respectively. KRAS mutations were detected in two patients (6.3%), NRAS in two (6.3%), and PIK3CD in one (3.1%). None of the patients had the BRAFindel. In addition to the BRAFV600E mutation, other BRAF mutations were also detected, including BRAFV600D, BRAFG466E, BRAFE501K and BRAFT599I in one patient each (3.1%) (Fig. 2). BRAFV600E mutations and MAP2K1 mutations were not associated with the type of organ involved.
Fig. 2
Target gene sequencing of lesion tissues of adult patients with unifocal LCH
TreatmentsThe initial treatment for the cohort is illustrated in a flow diagram in Fig. 3. One of the three patients with isolated liver involvement had not yet begun treatment at the time of last follow-up. Forty-one patients (58.6%) received surgical resection for first-line treatment. Because the surgical resection was not complete, two patients received postoperative radiation therapy, and two patients received postoperative VP-based chemotherapy. Eleven patients (15.7%) received radiation, and one patient received VP-based chemotherapy after radiotherapy to consolidate the treatment effect. Seven patients (10.0%) received systemic therapy, including MA for three patients, cytarabine monotherapy (100 mg/m2 subcutaneous injection, day1-5 every month, 12 months) for three patients, and VP-based therapy for one patient. Only 10 patients (14.3%) were observed. In addition to the patient who had not yet begun treatment, two of the three patients with liver involvement were treated with a cytarabine monotherapy regimen, and both achieved complete response.
Fig. 3
Treatments and outcomes of adult patients with unifocal LCH. *One patient had not yet begun treatment at the time of the last follow-up. CR complete response, VCR vincristine, VDS vindesine, MA methotrexate combined with cytarabine, CHOP cyclophosphamide, epirubicin, vindesine, prednisone
PrognosisOf the 70 patients, one patient was lost to follow-up, and follow-up data were available for 69 patients. The median follow-up duration was 39.4 months (range 0.7–211.8 months). Ten (14.3%) patients developed disease progression, of whom 4 had local recurrence, 2 progressed to SS-M and 4 progressed to MS LCH. The 3-year PFS was 81.9% for all patients (Fig. 4A). The progression rate of bone involvement was 12.2% (6/49), and it was 40.0% (2/5) for pituitary involvement, and 25.0% (1/4) for lymph node involvement. Among the 6 patients with bone involvement who had disease reactivation, 3 patients had local recurrence, 2 progressed to SS-M and 1 to MS. The affected site of the patient who progressed to MS was in the mandible. In addition, two patients with pituitary involvement and one patient with thyroid involvement progressed to MS, and one patient with lymph node involvement had local recurrence (Fig. 5). Factor associated with worse 3-year PFS was age < 30 years at diagnosis (52.2% vs. 97.0%, p = 0.005) (Fig. 4B). During follow-up, one patient with initial pituitary involvement progressed to MS after 34 months. This patient died at 98.8 months following the initial LCH diagnosis, due to an infection after chemotherapy for LCH progression. The 3-year OS rate was 100% (Fig. 4A). Organ involvement, treatment option, BRAFV600E mutations and MAP2K1 mutations were not associated with PFS or OS.
Fig. 4
Progression-free survival (PFS) and overall survival (OS) of adult patients with unifocal LCH (A), and PFS (B) according to age at diagnosis
Fig. 5
Progression pattern of each affected organ of adult patients with unifocal LCH. MS multiple system, SS-M single-system multifocal; Others: eyelid, submandibular gland, parotid gland, digestive tract and epidural mass in one case each
Comments (0)