
Remember me
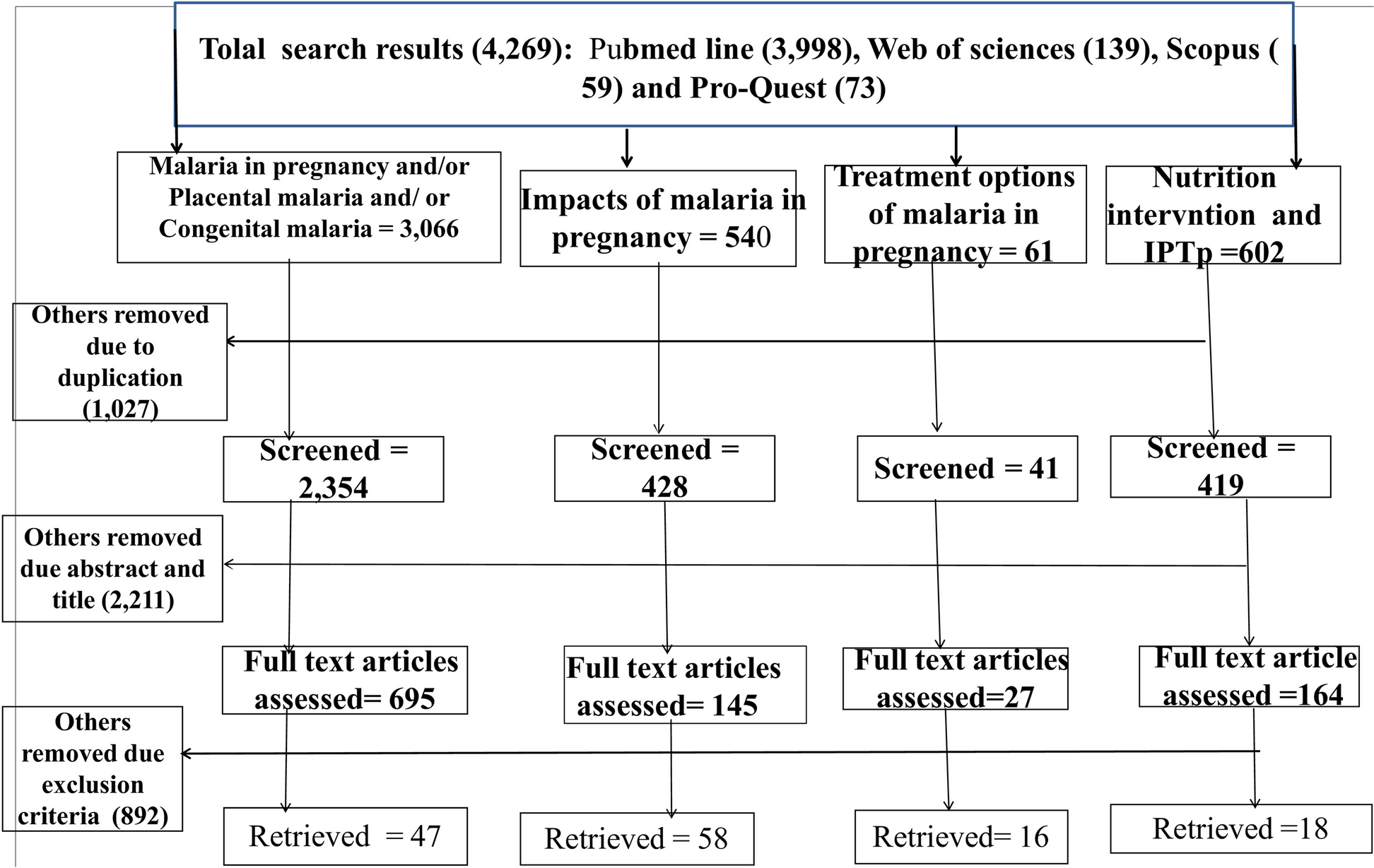






Studies have shown that posterior uveitis is the commonest type of TB uveitis from Gupta (42%), Ng (33%) and Koubaa (38.89%). Our study found anterior uveitis (50%) to be the most common initial presentation while posterior uveitis (40%) and panuveitis (40%) are most commonly seen on follow-up visits. No intermediate uveitis was reported in our study. (Fig. 2)
Fig. 2
Comparison of the clinical spectrum TB uveitis at initial presentation among 4 studies (Referred to [7,8,9]). Anterior uveitis is defined as iritis, iridocyclitis, or anterior cyclitis, with the inflammation located predominantly at the anterior chamber. Intermediate uveitis is defined as pars planitis, posterior cyclitis, or hyalitis, with predominant inflammation at the vitreous. Posterior uveitis is defined as focal, multifocal, or diffuse choroiditis, chorioretinitis, retinochoroiditis, retinitis, neuroretinitis, with inflammation primarily at choroid or retina. Panuveitis is defined as inflammation of all three locations – anterior chamber, vitreous, and choroid or retina. [27]
In our cases series, 30% of patients first presented with bilateral infection. In terms of posterior uveitis, 1 out of 4 in the first presentation and 2 out of 4 in follow-up visit were classified as serpiginous-like choroiditis. Since different studies show different clinical spectrums, we suggest that monitoring of both eyes is essential as unilateral infection can develop into bilateral involvement, as 5 out of 10 patients subsequently presented with bilateral uveitis at follow up. The most common chief complaints were red eye (30%), painful eye (30%) and blurry vision (30%), while photophobia (10%), reduced vision (10%), itchy eye (10%) and visual field defect (10%) were less commonly seen.
In this study, 70% of patients developed disease associated complications or side effects showing retinal vasculitis (40%), cystoid macular oedema (20%), ocular hypertension (30%), disc swelling (10%), steroid dependent (10%) and TB drug-induced hepatitis. Among 6 patients with prior history, only 3 of them developed complications in our series. We found that 3 out of 4 patients who developed retinal vasculitis were diagnosed with panuveitis, hence we suggest that patients with panuveitis may be prone to develop complications, of which in our series, retinal vasculitis is a commonly seen complication in panuveitic patients.
Diagnosis of TB uveitisAll patients in this case series were diagnosed with TB infection presumptively by at least one clinical sign together with a positive result of immunological or histological test. As the clinical signs and symptoms in TB uveitis are similar to other pathological causes of uveitis, TB diagnostic tests are mandatory to help the diagnosis of TB uveitis. In this study, only 20% of patients had prior known history of TB, which supports that ocular TB involvement cannot be ruled out in patients without history of systemic TB, especially in TB endemic regions. This also holds true for evaluating patients with previous presentation of idiopathic uveitis, for which the cause of the previous uveitic episode may not have been fully worked up for TB, or that the tests showed a false negative for the sample taken at the time. It is important that we think of TB as a differential diagnosis when encountering patients with uveitis in endemic areas, even when these patients do not present with the classical respiratory symptoms of TB, as TB is an entirely treatable and reversible cause of uveitis. In our case series, we demonstrated 40% of patients having had previous idiopathic uveal infection. Other aetiologies of uveitis should also be ruled out, such as herpes simplex virus (HSV), Epstein Barr virus (EBV), cytomegalovirus (CMV) and varicella zoster virus (VZV). With respect to the investigation of TB uveitis, chest x-ray and five types of TB tests including Tuberculin skin test, T-SPOT.TB test, QuantiFERON-TB gold test, and neck lymph node biopsy were used in different patients.
The least invasive investigative tools are usually the most acceptable to patients. However, this needs to be balanced with the diagnostic power of the respective tests. Chest x ray imaging, although regarded as one of the least invasive out of all the aforementioned investigations, provides the least diagnostic power for TB uveitis. There are several reasons as to why this is the case. Firstly, chest x ray can only detect pulmonary involvement of TB, including active pulmonary TB infection, or old TB with granulomatous cavitation which are more commonly seen at the lung apices. In addition, lesions seen at the lungs may not be entirely specific for TB, since there could be a wide variety of mimickers including lung abscess, enlarged mediastinal lymph nodes, lung carcinoma, secondary lung metastasis, or other mediastinal tumours including germ cell tumours which could also present similarly with lung nodule, sometimes also with cavitation, and pleural effusion and parenchymal opacities [18]. Further investigations must be performed to rule out other differential diagnoses of pulmonary lesions including the aforementioned. Similarly, other non-invasive examination tools including slit lamp, fundoscopy and optical coherence tomography (OCT) merely demonstrate active involvement of the ocular structures, yet fail to demonstrate the nature of the pathology, nor the pathogen causing the uveitis.
The Mantoux test, or TST, has to be interpreted with caution as this is subject to patient risk factors and the resultant size of the induration, and as a result false positives and false negatives may arise. For instance, an induration of ≥ 5 mm would be considered positive in high-risk patients, such as immunocompromised patients with Human Immunodeficiency Virus (HIV) or those on long-term high dose steroids, patients with end stage renal failure, those with recent contact with active cases, or those with chest x ray lesions consistent with previous TB infection. On the other hand, those with ≥ 10 mm induration are only considered positive if they are intravenous drug users, healthcare workers or those employed at high risk workplaces, paediatric patients exposed to high-risk adults, and immunocompromised patients including diabetics, long term steroid users, and those with malabsorptive state. Patients who demonstrate an induration diameter of ≥ 15 mm are deemed positive when they have no risk factors for TB. [12, 19]. Extra caution has to be taken as false positives may arise, for instance in those who have received their Bacillus Calmette-Guerin (BCG) vaccines, a particularly common practice for those residing in endemic areas such as Hong Kong. This case series highlighted a few cases for which false negatives arose using the above-mentioned guidelines. This includes 1 patient who had ≥ 5 mm induration and was considered negative as he did not have TB contact history nor CXR changes, and 1 patient who was considered negative as the induration was ≤ 5 mm, although subsequent T-SPOT.TB test yielded positive results in both patients. Although the Mantoux test is classically performed as a screening and diagnostic tool for TB, it cannot differentiate between latent and active infection, and cross-reactivity of non-tuberculous mycobacterium as well as previous BCG vaccination could result in false positives. It has also been demonstrated that in endemic areas like Hong Kong, the Mantoux test shows limited usefulness in detecting active TB disease in the elderly population. Compared to the positive rate of other diagnostic tests, chest x-ray demonstrates a rather low sensitivity so a negative chest x-ray result cannot rule out extra-pulmonary infection including ocular TB uveitis. IGRA tests, on the other hand, are advantageous in that it requires less time for generating results, and only requires one clinic visit, as opposed to the Mantoux test which requires 48–72 h of waiting time and requires the patient to come back to the clinic for reading of skin induration. The results are also relatively unaffected by previous BCG vaccine history, which is particularly useful in endemic populations. False negatives could be explained by inadequate sampling, presence of inhibitors, or ineffective lysis of cell wall and thus inadequate DNA isolation [20,21,22].
At present, it remains a challenge for TB infections to be diagnosed and confirmed with a single test, despite the many options for such purpose. 1 patient in our case series had TB diagnosed by Mantoux test in 1980 and treated with single agent for 6 months. In the first visit, this patient complained of sore throat and neck swelling for several month with a history of idiopathic unilateral recurrent acute anterior uveitis for two years. Chest x-ray and AFB smear were both negative, but positive for Mycobacterial infection on neck lymph node biopsy. Due to the history of recurrent uveitis and positive result on biopsy, TB was suspected and PET-CT was done to delineate the extent of systemic TB involvement and anti-TB treatment was commenced immediately. Finally, inflammation of the uvea resolved and vision improved in this case after completion of the anti-TB treatment protocol. We therefore concluded retrospectively that this patient had ocular TB, as inferred from the positive response towards anti-TB treatment.
In conclusion, TB investigation is suggested if patients have the following presentations especially in enedemic regions like Hong Kong: (1) recurrent uveitis of unknown cause; (2) chronic uveitis, especially for anterior and posterior uveitis; (3) not responding to conventional uveitic therapy; (4) immunosuppressed patients and (5) severe uvea involvement such as panuveitis or bilateral disease. We suggest that TB test should be performed routinely in uveitic patients with or without TB history or extra-ocular symptoms of TB, notably in endemic regions where TB is a differential diagnosis that has to be considered in every patient. This is because from our case series, not all of the patients had a documented or known history of latent TB disease, yet TB was the ultimate presumptive diagnosis and was eventually responsive to anti-TB therapy. Therefore, we should always have such infective differential diagnosis at the back of our minds, to detect and treat the disease in a timely manner. Taking all the pros and cons into consideration, T-SPOT. TB test and QuantiFERON gold test are useful in the diagnosis of ocular tuberculosis.
Medical TreatmentThere is still no consensus on the treatment protocol for tuberculosis uveitis, but the full treatment regime for active TB infection by the WHO is increasingly recommended. In this case series, isoniazid or rifampicin was started in the first two months, whereas other drugs including ethambutol, levofloxacin, moxifloxacin, rifampicin, pyrazinamide were added according to clinical response. Our patients were all treated in a multidisciplinary approach with respiratory physicians through directly observed treatment (DOT) and ophthalmologists monitoring the response to treatment. The treatment duration varied from 9 to 15 months, and 4 out of 9 patients received at least 12 months of anti-TB treatment, as several studies showed that prolonged anti-TB treatment can reduce uveitis recurrence [23,24,25,26]. All patients were prescribed steroids ranging from topical steroids, oral prednisolone or intravitreal dexamethasone implant in order to reduce inflammation or macular oedema. Three patients demonstrated ocular hypertension as a side effect of steroid use, and IOP lowering agent Timolol was prescribed in these patients for 4 to 15 weeks.
In our study, patient 1 (Table 2) refused to initiate anti-TB treatment and this patient experienced multiple uveitis recurrences up until 2020. When using anti-TB medications and steroids concurrently, strict monitoring is required as anti-TB drugs have mulitple side effects, as illustrated in 1 patient who experienced TB drug-induced hepatitis during treatment. 2 patients developed cystoid macular oedema, and anti-VEGF intravitreal injection was administered to reduce the oedema. Visual acuity, visual field, colour vision, urea, electrolytes and liver function should be assessed and baseline values should be obtained prior to starting treatment with ethambutol, rifampicin, isoniazid and pyrazinamide, such that any manifestations of their side effects may be picked up in a timely manner. Regular follow-ups such as OCT assessment should be performed, especially for high-risk patients including diabetics, elderly, those with renal or liver disease and chronic alcoholics.
Treatment outcomeThe visual acuity improved from 0.85 (initial) to 0.77 (final) within a mean treatment duration period of 10.63 months. The visual acuity of 60% patients was improved and 40% worsened. Among those who improved, 4 out of 6 patients were unilaterally infected and 2 out of 6 patients were bilaterally infected. This result may imply that unilateral uveitis tend to have a better visual prognosis then bilateral uveitis. In the 6 patients with improved vision, only 3 out of 6 patients had prior history of TB infection or uveitis, suggesting past history may not affect the prognosis. Moreover, we suggest that different types of uveitis have different prognoses. This study found that 100% of anterior uveitis, 75% panuveitis and 25% posterior uveitis patients had visual acuity improvement. In this case series, only 2 out of 6 patients who had complications had better final visual acuity after anti-TB treatment, so we believe that the prognosis of patients with complications may be suboptimal even after completion of anti-TB treatment.
LimitationsPotential limitations of this study should be mentioned. A small sample size of ten patients were analyzed, as this was a single centre cross-sectional study. A wider scale study could be done in the future, incorporating cases from the entirety of the Hong Kong public and private system, to better describe the characteristics of TB uveitis in our locality.
Comments (0)