
Remember me
Participants were selected from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD), as described previously (16). The HELIAD is a population-based, multidisciplinary-collaborative study designed to explore the epidemiology of subjective cognitive decline (SCD) and, the prevalence and incidence of mild cognitive impairment, Alzheimer’s disease, and other types of dementia in the Greek population. Participants were 65 years of age and over and selected by random sampling of community-dwelling elderly individuals from the records of two Greek urban and rural populations.
The full cohort of the HELIAD consists of 1984 individuals who were randomly sampled and invited to participate in the study; thus, they can be considered representative of the whole elderly population in Greece. All participants were examined at baseline and then asked to attend a follow-up visit about 3 years after the initial evaluation. The baseline visits occurred between December 2009 and June 2016, while follow-up was conducted between January 2013 and July 2019. All participants provided informed consent before participation in the study. The institutional ethics review board of the University of Thessaly and the National and Kapodistrian University of Athens approved all procedures.
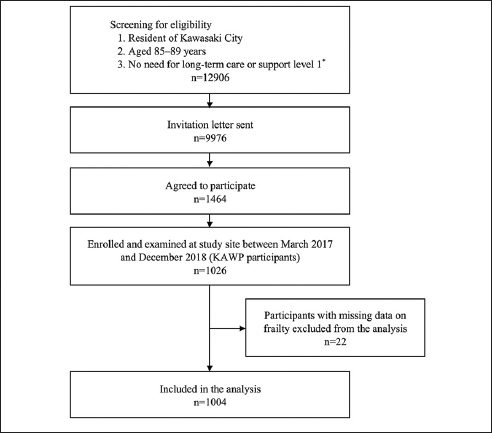
For the present study, the baseline sample consisted of 1,943 participants, (age: M=73.9, SD=5.45 years); of these, 1,121 individuals participated in the second evaluation. For the longitudinal analysis, we excluded participants with a diagnosis of frailty, MCI, dementia, severe anxiety, and depression on the first evaluation, and those with missing data on either assessment (n=146), resulting in a total sample of 975 participants in the follow-up, with an average follow-up interval of 3.1 years (SD=0.84 years) (Figure 3).
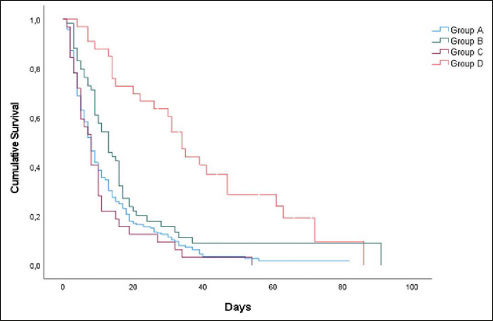
Figure 1
Kaplan-Meier survival curves for frailty (using Fried’s definition) according to SCD complaints regarding orientation
Figure 2
Kaplan-Meier survival curves for frailty (using the Frailty Index) according to SCD complaints regarding orientation
Figure 3
Flow chart of the study sample in the HELIAD longitudinal study related to the present analyses
Evaluation - ProcedureParticipants of the HELIAD underwent a structured clinical evaluation. In a face-to-face interview, participants provided information regarding (previous and current) medical problems, neurological conditions, neuropsychiatric symptoms, hospitalizations, surgeries, injuries, and current medications. In addition, an extensive structured physical examination, evaluating neurological signs and symptoms, was conducted for each participant. Structured questionnaires were administered to gather information about participants’ functioning levels, social, mental, and physical activities, sleep, and dietary habits. Information regarding sociodemographic variables was also collected. All participants were also administered a comprehensive neuropsychological assessment of all major cognitive functions (16–18).
The interviews and assessments were conducted by qualified and licensed neurologists, neuropsychologists, and dietitians. For most of the participants, both evaluations were completed during a single visit, which lasted about 2–2.5 hours per participant. The health professionals were adequately trained on the study’s protocol and procedures, to ensure the reliability and validity of the study’s data.
Diagnosis of each participant’s clinical and cognitive status emerged from regular diagnostic consensus meetings attended by all researchers. MCI was diagnosed when participants had subjective cognitive complaints and objective impairment in at least one cognitive domain, scoring at least 1.5 standard deviation (SD) below average, but preserved activities of daily living. More information regarding the diagnostic criteria and consensus procedures is described in detail elsewhere (16, 19). The diagnosis of dementia was based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria.
Changes in the performance of daily activities and self-care habits were measured using the Blessed Dementia Scale. For the instrumental activities of daily living (IADLs), participants indicated whether they were able to perform eight IADLs based on the Lawton–Brody scale, such as using a telephone, being responsible for their own medication, managing money, ability to use public or private transport, shopping, grooming, doing housework, and doing laundry. Socioeconomic status was divided into lower and higher categories, based on homeownership status (homeowner/renter), its area (m2), and the number of rooms in the home. Ownership of cars or secondary residences as well as feasibility, length, and destination of summer vacations, was also taken into consideration. The data were adjusted for depressive symptoms over the past week, using the 15-item version of the Geriatric Depression Scale (GDS) and a cut-off score set at 6 points, and each item of the scale assessing the presence or absence of a specific depressive symptom (20, 21). Anxiety over the past week was measured using the 7-item anxiety subscale from the Hospital Anxiety and Depression scale (HADS-A). Each item is rated from 0 (best) to 3 (worst), and the cut-off score for anxiety was set at 8 points (22). A Greek version of the scale has been validated and has shown good psychometric properties (23).
Neuropsychological evaluationParticipants received a comprehensive neuropsychological assessment covering five cognitive domains: memory, language, attention/speed, executive functioning, and visual-spatial perception. Scores on each cognitive test were converted into z-scores using the mean and standard deviation (SD) values from the study sample. Subsequently, z-scores of individual neuropsychological tests were averaged to produce domain composite scores for the five cognitive domains mentioned above. The decision regarding the grouping of neuropsychological tests was based on prior knowledge of the cognitive functions that each test primarily reflects. Furthermore, neuropsychological domain composite scores were averaged to calculate a global composite neuropsychological functioning score. More information regarding the neuropsychological evaluation is described elsewhere (18, 24).
SCD AssessmentWe assessed SCD based on eighteen self-reports of relevant complaints, through a series of single and selected questions taken from the medical history described in previously published articles (18, 24, 25). The questions assessing complaints regarding SCD were used as dichotomous variables based on the participant’s responses. Each question had a possible rating of (0) “I do not have this complaint” or (1) “I have this complaint”. We categorized each of the eighteen questions into four cognitive domains: memory, naming, orientation, and mathematical reasoning. The memory domain included questions that refer to robust memory complaints and had two subdomains: General Memory Decline (GMD) and Specific Memory Decline (SMD). The subcategory GMD included a gold standard set question «Have you had any memory problems lately?». The SMD included seven questions that referred to different memory tasks, i.e., remembering shopping lists, remembering things that happened recently, and a tendency to dwell on the past. Participants were characterized as having SCD if they gave a positive response to a single question in the GMD domain and/or at least one positive response to the seven questions of the SMD domain (SMD1) regarding memory. The other cognitive domains consisted of questions that do not solely refer to pure memory complaints. The domain regarding the decline in naming included two questions, in orientation five questions, and in mathematical reasoning three questions. Participants were characterized as having SCD if they gave at least one positive response to the specific domain’s questions.
To examine SCD in depth, we created a variable that summarizes all positive responses in the four cognitive domains (memory, naming, orientation, and mathematical reasoning) in total with the abbreviation SAD (the sum of all domains with subjective cognitive decline). This variable was calculated as binary (0=no SCD complaints and 1=one or more SCD complaints in the aforementioned cognitive domains).
To examine any association between different categories of SCD and frailty, we performed statistical analyses by examining each cognitive domain of SCD separately with both frailty indices. For these analyses, we maintained the content of the naming, orientation, and mathematical reasoning domains, but created additional variables for the memory domain. The frequency analysis of the seven questions in this subdomain allowed us to redefine three variables using a broad, intermediate, and restrictive approach. The idea was to create a trichotomous variable to investigate the correlation of frailty in people with different levels of SCD burden concerning their memory ability. As the variable of at least one Specific Memory Decline (SMD1) (i.e., the participant gave at least one positive answer) was already in place, we used it as the variable that summarizes all SCD complaints. Additionally, we created the variable of at least two Specific complaints related to Memory Decline (SMD2) as well as that of at least three Specific complaints related to Memory Decline (SMD3), with the participants giving at least two and three positive answers, respectively, to the SMD questions of this category.
Frailty AssessmentWe assessed frailty according to two different definitions that have been researched for efficacy, namely, a) Fried’s definition (7) and b) the Frailty Index (FI) (26). These methods have also been described elsewhere (27, 28).
The Fried definitionThis definition is most commonly accepted and belongs to the phenotypic approach derived from the work of Fried and colleagues (2001) in the Cardiovascular Health Study. Research has shown this definition to be consistent with that of clinical syndrome. It describes frailty as a distinct physiological process resulting from the dysregulation of multiple systems within the body. Participants who met three or more of the manifestations below were considered frail. The presence of fewer than three criteria indicates prefrailty (7). Prefrailty is described as the state between frail and robust (non-frail) and indicates the dynamic nature of frailty: (a) Slow walking speed was defined as the lowest 20th percentile of our study population for the 4-minute walking speed test (adjusted for sex and height); (b) shrinking/weight loss was defined as body mass index (BMI) < 18.5 kg/m2; (c) poor endurance/ exhaustion was evaluated as a negative response to the question taken from the Geriatric Depression Scale “Do you feel full of energy?” (29); (d) low physical activity was estimated based on a validated questionnaire, the Athens Physical Activity Questionnaire (APAQ), which calculates participants’ daily energy expenditure for physical activities (30). The lowest 20% for each sex was assumed to be indicative of frailty; (e) weakness was defined as grip strength in the lowest 20% adjusted for sex and BMI. The grip strength of the dominant hand was measured with an electronic dynamometer (Model MG-4800, the United Kingdom) and the mean strength of three trials was used in the current analysis.
The Frailty Index (FI)The Frailty Index (FI) is used more frequently as a multidomain approach to assess frailty and is suggested by Rockwood and colleagues in the Canadian Study of Health and Aging (CSHA) (26). The FI is based on the routinely used Comprehensive Geriatric Assessment (CGA) and is based on 70 age-related multidomain deficits from a broader perspective, including mood, cognition, and incontinence. For the construction of FI, we followed the standard procedure described by Searle and colleagues (31). In the present study, 61 items regarding diseases, syndromes, functioning in activities of daily living, cognitive decline, mood disorders, and performance in physical activities were included for the assessment of frailty. The participants’ deficit scores were totaled and according to this index, a score of 0.25 was determined as the frailty cut-off point (32). The higher the deficit score, the more advanced the frailty state.
Statistical analysisQuantitative variables were expressed as mean values (SD), while qualitative variables were expressed as absolute and relative frequencies. For the comparisons of proportions, chi-squared and Fisher’s exact tests were used. Student’s t-tests were computed for the comparison of mean values between the two groups.
Univariate and multivariate Cox regression analyses were used to determine the association between the presence of SCD complaints (yes or no) at the baseline and having frailty at the second visit. The primary predictor was SCD complaints divided into four cognitive domains, and the outcome was the frailty status. Different categories of SCD complaints were examined with eight variables and frailty with two different methods, one, of the phenotypic-physiologic, and another of the multidomain approach. Irrespective of the definition used, frailty status was entered as a categorical variable (comparing frail to non-frail individuals). For the Fried approach, we included prefrail participants in the non-frail category. SCD complaints were entered into the models mentioned above, both as a continuous and a categorical variable.
We explored the role of various established risk factors of frailty using multivariate Cox regression analyses, in adjusted models. Specifically, the multivariate Cox regression analyses were conducted after adjusting for age, sex, educational level, socioeconomic status, comorbidity, global neuropsychological functioning score, and, the score of each participant on the depression and anxiety scales. Hazard ratios (HR) with 95% confidence intervals (95% CI) were computed from the results of the Cox regression analyses. Age, education (in years), comorbidity, global neuropsychological functioning score, and scores on the anxiety and depression scales were used as continuous variables, whereas sex was used as a dichotomous variable. Socioeconomic status (SES) was measured using four socioeconomic variables: economic reserves or assets, holiday/traveling, and leisure time activities. SES was used as a dichotomous variable with two levels «High» and «Low».
Kaplan-Meier survival estimates for frailty were graphed over the follow-up period. All reported p values are two-tailed. Statistical significance was set at p<0.05.and analyses were conducted using SPSS (version 23.0).
Comments (0)