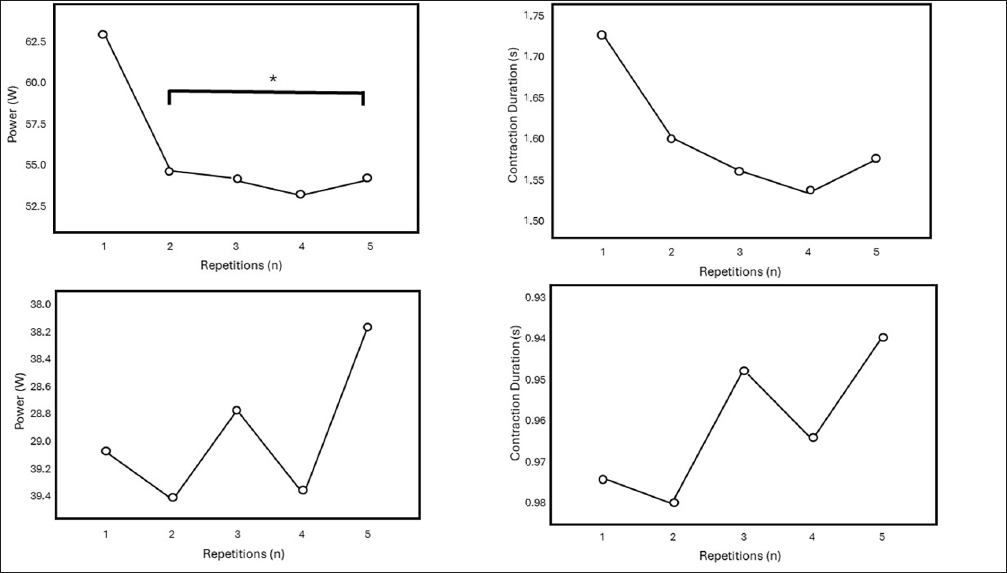
The assessment of lower limb muscle power is an important aspect of the physical evaluation of older adults by providing relevant insights on physical status. This information, in turn, may be used by, contributing to health professionals in the identification of individuals at high risk of experiencing negative events, and to devise the best therapeutic approach. Yet, the clinical evaluation of muscle power is hampered by the lack of an unequivocal assessment tool. Our findings indicate that peak lower limb muscle power is reached in the first concentric contraction and declines significantly thereafter (Figure 1). Furthermore, we observed that 5STS-based biomechanical aspects demonstrate a good capacity to discriminate individuals according to WS performance (Table 2). We also noted that muscle power during specific contractions might contribute to differentiating older women with low and high performance on TUG (SM1) and IHG tests (SM2). Notably, such associations were not observed with muscle power estimated according to 5STS equations. Pearson’s correlation analysis suggested similar results (Table 3 and SM3).
The fact that peak lower-limb muscle power was reached during the first stand movement might suggest that one sit-to-stand action could be a sufficient representation of lower-limb muscle power in older adults. The capacity to produce power decreases in tasks requiring high velocities and is exacerbated during repeated contractions, including cyclic STS movements (20–22). Muscle power is primarily produced by the activity of type II muscle fibers, those more sensitive to fatigue (23–25). As muscles are required to continue producing strength at high velocities, the availability of ATP and phosphocreatine of type II muscle fibers becomes insufficient (24, 26, 27), leading fatigue-resistant fibers to become protagonists of muscle actions (24), causing significant reductions in power output (24, 25).
In the present study, AMP during the second concentric contraction (stand movement) was significantly reduced by 12.5% in comparison to the first muscle action. These abrupt and meaningful losses might represent structural and metabolic changes commonly observed in old muscles, mainly in type II muscle fibers, including relative reduction of these fiber types, reduced phosphorylation of the fast myosin regulatory light chain and rates of myosin force production, and longer myosin attachment times (25).
No significant differences were found in the duration or velocity of sit movements among eccentric contractions (Figure 1). However, visual inspection revealed a “W-shaped” curve during eccentric contractions, in which oscillations are noted between the 2nd-4th and 1st-3rd-5th repetitions. These observations suggest that older adults might have problems controlling eccentric actions performed after explosive moments. These premises are partially supported by clinical observations, given that frail individuals, mainly those institutionalized and hospitalized, have two major motor behaviors when they have to sit: i) extremely controlled movement and ii) fast movement due to incapacity to sustain body weight.
Eccentric actions involve a lower activation of motoneurons, when compared to concentric actions, and a specific recruitment of type II muscle fibers (25). It has been seen that eccentric muscle strength presents a virtually lesser decline with age in comparison to concentric and isometric muscle actions, leading many authors to argue that this physical capacity is preserved in advanced age (28). However, these conclusions are obtained after testing exclusively eccentric actions (28) and no studies have examined the impact of explosive movements in a subsequent capacity to generate eccentric strength. In one of the few studies examining this subject, it was found that fatigue induced significant decreases in eccentric muscle strength, mainly when it is required during high velocities (29).
Although this interpretation is only speculative, these results emphasize the need for more specific investigations to understand if the patterns of eccentric actions noted during 5STS are a result of type II muscle fibers’ overload, in which movements in the boundaries, with extreme caution and/or inability to sustain body weight, reveal the lack of strength to maintain muscle actions. Slow (controlled) eccentric movements produce worse performance on 5STS and are captured in test results. But then, a question that arises from this view is whether fast eccentric actions, and consequent better 5STS results, represent good performance or neuromuscular weakness.
Results indicated that 5STS-based biomechanical aspects were better discriminators and more associated with IHG, TUG, and WS performances than 5STS muscle power equations (Table 2, SM1, SM2, SM3). These findings are partially supported by other investigations that found no significant associations between muscle power estimated according to 5STS performance and WS (10). This scenario is surprising given that TUG and WS performances are dependent on muscle power (13, 30–32).
5STS-based muscle power equations have faced criticism due to their assumption that only a portion of the body’s mass accelerates during the concentric phase of movement, whereas the production of mechanical power in similar conditions should account for alterations in the kinetic and potential energy of the entire body (11). The authors also highlighted conceptual problems with the definition of the concentric phase (11). Notably, both 5STS-based muscle power equations aspects criticized by Fabrica & Biancardi (11) are associated with the concentric phase of the movement, in which more balance is likely required (33), affecting TUG performance, and is associated with the propulsion required to move fast in mobility tasks (4).
On the other hand, the analysis of individual biomechanical aspects captures specific moments of physical tasks (e.g., propulsion, dynamic balance), which explain the association among these parameters. The fact, for example, that significant differences in MPE3 were found between participants with high and low TUG performance suggests that eccentric actions might be a better discriminator of mobility than concentric and combined contractions. Moreover, Pearson’s correlation results indicate that numerous biomechanical 5STS parameters (e.g., MPC, MCP2, MCP3, MCP4, MCP5, DC5, MPE2) were significantly associated with IHG, TUG, and WS, suggesting that all these variables might contribute to identifying people with low physical function.
The fact that MPC, MPE, and DC variables becamesignificantly associated with physical performance tests when results were adjusted according to BMI, suggests an important role of body mass distribution in this scenario. Individuals with higher BMI need to produce more strength than those with lower BMI values to move the body rapidly during sit and stand movements. The inability to generate strength properly in these circumstances reflects in lower power production and longer contraction durations and might explain the associations observed in the adjusted analysis.
The present study is not free of limitations. First, specific muscle power, adjusted according to muscle mass (e.g., computer tomography, magnetic resonance imaging, or dual X-ray Absorptiometry), was not estimated in the present study. Second, participants were not screened for sarcopenia or frailty. Third, important information associated with the presence of chronic conditions, such as pharmacological therapy and disease status, was not recorded. Fourth, only community-dwelling women were examined, and extrapolations to men or people in other contexts (e.g., institutionalized) should be made with caution. Fifth, correlation analysis was not corrected according to numerous covariables that might influence muscle power, including physical activity levels, diet quality, and sleep. Sixth, the linear encoder only captures movements in one plane, indicating that disturbances during sit and stand actions were not recorded. Finally, the results shown in this work are derived from cross-sectional observations. The possibility cannot be ruled out that differences in birth cohorts may have influenced some of the assessed parameters. A deeper understanding of age-dependent differences in muscle power requires an analysis of prospective data that are unavailable at this stage for our study.

Comments (0)