
Remember me




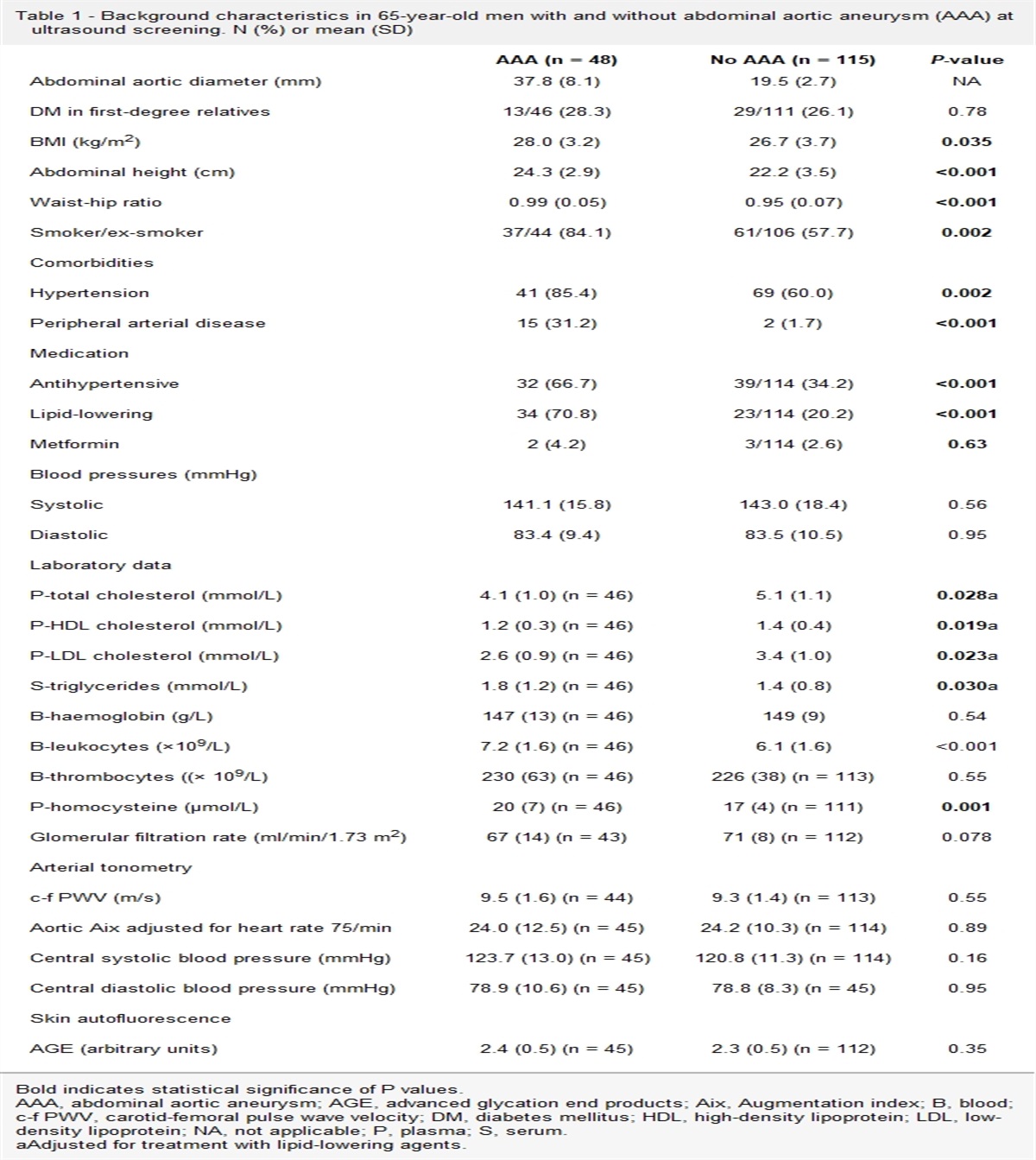




Obesity is a direct contributor to cardiovascular risk, acting independently and through association with metabolic risk factors including dyslipidaemia, hypertension and hyperglycaemia, which may arise as a consequence of lipotoxicity [1–3]. Abdominal obesity is a major risk factor for cardiovascular disease (CVD) and type 2 diabetes (T2D), and high waist circumference (measuring intraabdominal fat) should be considered hazardous to health irrespective of BMI [4,5]. Despite rising prevalence worldwide [4], acceptance of obesity as a chronic disease remains poor [6]. It is often disregarded as a serious health problem that requires medical attention and therefore, effective clinical care is lacking [6,7].
Are cardiologists doing enough to treat obesity?Appropriate management of obesity is essential to improving cardiovascular risk and preventing secondary CVD [1,7]. A recent study confirmed that up to 80% of people with coronary heart disease have comorbid overweight or obesity, the majority presenting with hypertension, dyslipidaemia and diabetes [7]. However, some physicians did not record weight in medical records or address it with patients [7]. Thus, while cardiologists treat many people with obesity and comorbid CVD, these individuals are not receiving appropriate treatment and empathetic support despite the known benefits. The question is, why?
Lack of time, perception that their obesity management skills are inadequate and an inability to recognise obesity as a chronic disease are all reported reasons for not discussing weight [8–10]. Furthermore, many healthcare professionals (HCPs) see limited clinical value in modest weight loss, despite current evidence demonstrating that it can reduce the risk of obesity-related complications [11].
Can treatment of obesity improve cardiovascular outcomes?Modest weight loss of 5–10% can induce clinically significant improvements in cardiovascular and metabolic factors, without the need to achieve an ‘ideal’ BMI [12]. Evidence shows that improvements in glycaemia, blood pressure, triglycerides, cholesterol and measures of feeling and function (quality of life, knee pain, etc.) can be achieved with moderate weight reduction, while further weight loss induces additional improvements [12]. Improving symptoms of obstructive sleep apnoea usually requires ≥10% weight loss [12].
The Look AHEAD trial examined whether intensive lifestyle intervention for weight loss would reduce cardiovascular morbidity and mortality among people with overweight/obesity and T2D [13]. Reduction in cardiovascular outcomes versus controls was not demonstrated at 9.6 years, and the mean initial weight loss of 8.6% at 1 year was followed by regain [13]. After a 9.6-year follow-up, the trial was deemed futile and stopped early [13]. However, a post hoc analysis found that individuals in either group who lost ≥10% of their initial body weight in the first year had a 21% lower risk of the primary outcome (major cardiovascular events; hazard ratio [HR] = 0.79; 95% confidence interval [CI], 0.64–0.98) and a 24% reduced risk of the secondary CVD outcome (HR = 0.76; 95% CI, 0.63–0.91) versus individuals with stable weight or weight gain [14]. This suggests that weight loss of ≥10% may be needed to reduce cardiovascular risk – findings that have been mirrored in outcomes from bariatric surgery [15].
Achieving even modest weight loss can be challenging because it usually requires a multifactorial lifestyle intervention comprising changes to diet, physical activity and regular behaviour therapy sessions [16]. Medications approved for weight management by the US Food and Drug Administration (FDA) or the European Medicines Agency (EMA), which until recently included orlistat, naltrexone–bupropion, phentermine–topiramate (FDA only) and liraglutide 3.0 mg, can increase weight loss by 4–9% versus lifestyle alone [17,18]. However, the use of these therapies is currently limited and none, except liraglutide when used in diabetes management, has been shown to reduce cardiovascular events [19]. This is changing as new, biology-based approaches to weight management emerge and the recent FDA and EMA approval of semaglutide 2.4 mg for the treatment of obesity [20,21]. On average, semaglutide 2.4 mg results in weight loss of 15% when combined with lifestyle, versus 2.4% with lifestyle alone, in people without T2D [22]. A cardiovascular outcomes trial (CVOT) called SELECT is underway to test the superiority of semaglutide 2.4 mg versus placebo for cardiovascular risk reduction in 17 500 people with overweight/obesity and established CVD in the absence of T2D or HbA1c >6.5% [23]. It is the first dedicated CVOT for an obesity treatment that seeks to establish superiority in the prevention of major adverse cardiovascular events (MACE) [23].
For older medications, regulators required non-inferiority trials to ensure safety [22]. Outcomes of the 2010 SCOUT trial, in which sibutramine demonstrated an increased risk of nonfatal myocardial infarction and stroke in people with pre-existing CVD, led to its withdrawal and tighter regulatory requirements for CVOTs in obesity [24]. The LIGHT study (naltrexone–bupropion) and the AQCLAIM trial (phentermine–topiramate) were required non-inferiority CVOT trials; however, neither was completed [24,25]. CAMELLIA-TIMI-61 confirmed the cardiovascular safety of lorcaserin but showed no cardiovascular benefit; it was later withdrawn owing to potential cancer risks [24]. Although the approved label for liraglutide 3.0 mg describes its benefits for cardiovascular risk reduction, these statements are based on the LEADER trial, a CVOT for liraglutide 1.8 mg in a T2D population [26–28]. Semaglutide 0.5 and 1.0 mg demonstrated reductions in MACE among individuals with T2D as part of the SUSTAIN-6 trial [29]; thus, it is hoped that SELECT will produce positive results.
Regarding treating obesity, the mechanism of cardiovascular risk reduction with anti-obesity medications (AOMs) may be through weight loss and its impact on intermediaries – lipids, glycaemia, blood pressure, and inflammatory and prothrombotic mediators. However, the AOM may itself promote benefits. This is the case with semaglutide and other glucagon-like-peptide-1 (GLP-1) analogues, because of their pleiotropic effects on cardiovascular biology which include lipid, cardiorenal, blood pressure and inflammatory benefits [30]. The future of weight management is promising, thanks to improved understanding of the biology underpinning energy–balance regulation and food intake [31,32]. New AOMs based on this biology are under development, with tirzepatide, a GLP-1 and glucose-dependent insulinotropic polypeptide dual agonist, demonstrating weight loss of up to 13.1% at 40 weeks in people with T2D versus 6.7% with semaglutide 1.0 mg [33,34], and no increase in MACE risk at 104 weeks of exposure [35]. In a phase 3 trial of adults with obesity, once-weekly tirzepatide 15.0 mg resulted in a mean weight loss of 20.9% at week 72 versus 3.1% with placebo (P < 0.001) [36]. Furthermore, phase 1b data for cagrilintide 4.5 mg plus semaglutide 2.4 mg, a new long-acting amylin analogue and GLP-1 agonist combination, demonstrated weight loss of up to 15.4% at 20 weeks versus 8.0% in a matched cohort receiving placebo plus semaglutide [37] (Fig. 1). As promising results for these combinatory approaches emerge, it becomes clearer that a deeper understanding of the molecular pharmacology of body-weight regulation is integral to the development of new-generation AOMs [33].
 Fig. 1:
Fig. 1: Proportion of weight loss achieved with anti-obesity medications versus placebo or an active comparator at approximately 1 year. Data for the STEP trials were reported at approximately 1.3 years. Data for tirzepatide were reported at 72 weeks. †Data reported at 20 weeks; matched comparator cohort received placebo plus semaglutide 2.4 mg.
Achieving weight loss of ≥15% has the potential to transform chronic obesity management, because of its ability to improve multiple intermediate endpoints. However, it is still important to assess whether this translates into cardiovascular event reduction. For cardiologists, this means including obesity as a cardiovascular risk factor in addition to lipid levels, blood pressure and dysglycaemia, which are already well-managed.
How can cardiologists and other healthcare professionals approach obesity in practice?Despite its links with CVD and T2D, obesity is underdiagnosed [5,7]. While addressing obesity can be challenging [5], especially in the presence of CVD [38], all HCPs should ask permission to discuss weight in a sensitive, non-stigmatising manner [11,39]. Cardiologists and other HCPs treating people with obesity and high cardiovascular risk should conduct assessments to classify the severity of obesity and identify root causes [9]. This involves measuring waist circumference to evaluate visceral adiposity and BMI (ethnicity-specific), identifying contributors to weight gain such as medication, and the presence of obesity-related risks and complications [9,40].
A key part of weight management is setting personalised goals that support sustainable outcomes [9,39]. Cardiologists should conduct a thorough history focussing on eating patterns, physical activity, previous weight management, sleep and psychological status [40]. Providers must work with patients to identify elements of their lifestyle they wish to change, set realistic expectations for weight loss and highlight the benefits of modest weight reductions [11,41]. When lifestyle interventions are insufficient, cardiologists should discuss initiating AOMs [11,40]. They should advise individuals on the available treatments, considering their benefits and risks including cardiovascular factors, and highlight that these therapies should be used alongside lifestyle changes [40].
An alternative approach for people who have not been able to achieve weight loss targets with lifestyle or AOMs is referral to appropriate specialists for consideration of bariatric surgery [40]. This has been shown to induce greater weight losses compared with other traditional treatments and is associated with numerous health benefits, including long-term remission of most adiposity-related diseases, a reduced need for medication and control/remission of T2D in conjunction with optimised medical management [9,42]. In individuals with a BMI ≥40 kg/m2 or a BMI ≥35 kg/m2 with at least one adiposity-related disease, bariatric surgery could be a suitable option [9,39] (Fig. 2).
 Fig. 2:
Fig. 2: A call to action for cardiologists – reasons to address obesity in clinical practice and advice on how to do it. CVD, cardiovascular disease.
When a person with CVD and obesity receives comprehensive and compassionate care, they may be better placed to improve disease-related factors such as blood pressure, glycaemia and visceral fat – the root of multiple complications. Together, these improvements may result in improved quality of life and life expectancy.
AcknowledgementsThe development of this article was supported by an unrestricted educational grant from Novo Nordisk A/S.
The authors are grateful to Dr. Ruth Wills of International Medical Press for editorial support in the development of this article.
Conflicts of interestThe authors have the following potential conflicts of interest to declare.
D.H.R. has acted as an advisor or consultant for Altimmune, Amgen, Boehringer Ingelheim, Calibrate, Carmot, Epitomee, Gila Therapeutics, ifa Celtic, Janssen, Lilly, Novo Nordisk, real appeal (United Health), Roman, Scientific Intake, Wondr Health, Xeno Bioscience, Ysopia and Zealand. She has participated in speakers bureau for Novo Nordisk and has ownership interest (stock options) in Epitomee, Calibrate, Roman, Scientific Intake, Gila Therapeutics and Xeno Bioscience (returned in 2022). She is a member of the SELECT Steering Committee (Novo Nordisk) and the DSMB (IQVIA for Rhythm). S.J. has participated in company-sponsored speakers bureau for Amarin, Amgen, AstraZeneca, Bayer, BMS, Berlin Chemie, Boehringer Ingelheim, Lilly, Merck, MSD, Novo Nordisk, Novartis, Pfizer, Roche, Sanofi-Aventis and VIFOR. He has received honoraria or consultation fees from Amarin, Amgen, AstraZeneca, Bayer, BMS, Berlin Chemie, Boehringer Ingelheim, Lilly, Merck, MSD, Novo Nordisk, Novartis, Pfizer, Roche, Sanofi-Aventis and VIFOR. J.E.D. has received CME honoraria and/or consulting fees from Amgen, Boehringer Ingelheim, Merck, Pfizer, Aegerion, Novartis, Sanofi, Takeda, Novo Nordisk and Bayer. He has received research grants from BHF, MRC (UK), NIHR, PHE, MSD, Pfizer, Aegerion, Colgate and Roche. He is a member of SOUL and SELECT Study Steering Committees for Novo Nordisk.
References 1. Powell-Wiley TM, Poirer P, Burke LE, Després JP, Gordon-Larsen P, Lavie CJ, et al. Obesity and cardiovascular disease. Circulation 2021; 143:e984–e1010. 2. Redinger RN. The pathophysiology of obesity and its clinical manifestations. Gastroenterol Hepatol (N Y) 2007; 3:856–863. 3. Marín-Royo G, Ortega-Hernández A, Martínez-Martínez E, Jurado-López R, Luaces M, Islas F, et al. The impact of cardiac lipotoxicity on cardiac function and Mirnas signature in obese and non-obese rats with myocardial infarction. Sci Rep 2019; 9:444. 4. Rhee EJ. The influence of obesity and metabolic health on vascular health. Endocrinol Metab 2022; 37:1–8. 5. Després JP, Carpentier AC, Tchernof A, Neeland IJ, Poirier P. Management of obesity in cardiovascular practice: JACC focus seminar. J Am Coll Cardiol 2021; 78:513–531. 6. Ritten A, LaManna J. Unmet needs in obesity management: from guidelines to clinic. J Am Assoc Nurse Pract 2017; 29:S30–S42. 7. De Bacquer D, Jennings CS, Mirrakhimov E, Lovic D, Bruthans J, De Smedt D, et al. Potential for optimizing management of obesity in the secondary prevention of coronary heart disease. Eur Heart J Qual Care Clin Outcomes 2022;8:568–576. 8. Kim T. Barriers to obesity management: patient and physician factors. J Obes Metab Syndr 2020; 29:244–247. 9. Wharton S, Lau DCW, Vallis M, Sharma AM, Biertho L, Campbell-Scherer D, et al. Obesity in adults: a clinical practice guideline. CMAJ 2020; 192:E875–E891. 10. Glauser TA, Roepke N, Stevenin B, Dubois AM, Ahn SM. Physician knowledge about and perceptions of obesity management. Obes Res Clin Pract 2015; 9:573–583. 11. O’Shea D, Kahan S, Lennon L, Breen C. Practical approaches to treating obesity: patient and healthcare professional perspectives. Adv Ther 2021; 38:4138–4150. 12. Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: differences at 5%, 10%, 15%, and over. Curr Obes Rep 2017; 6:187–194. 13. Wing RR, Bolin P, Brancati FL, Bray GA, Clark JM, Coday M, et alLook AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 2013; 369:145–154. 14. Gregg E, Jakicic J, Blackburn G, Bloomquist P, Bray G, Clark J, et alLook AHEAD Research Group. Association of the magnitude of weight loss and changes in physical fitness with long-term cardiovascular disease outcomes in overweight or obese people with type 2 diabetes: a post-hoc analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol 2016; 4:913–921. 15. Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery. J Intern Med 2013; 273:219–234. 16. Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation 2014; 129:S102–S138. 17. Tak YJ, Lee SY. Anti-obesity drugs: long-term efficacy and safety: an updated review. World J Mens Health 2021; 39:208–221. 18. Sjöström L, Rissanen A, Andersen T, Boldrin M, Golay A, Koppeschaar HP, Krempf M. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. European Multicentre Orlistat Study Group. Lancet 1998; 352:167–172. 19. Ryan DH. Drugs for treating obesity. In: Eckel J, Clément K, editors. Handbook of experimental pharmacology. Springer, Berlin2021. pp. 1–28. 20. US Food and Drug Administration. FDA approves new drug treatment for chronic weight management, first since 2014. 2021. www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014. [Accessed 12 May 2022]. 21. European Medicines Agency. Wegovy. 2022. www.ema.europa.eu/en/medicines/human/EPAR/wegovy. [Accessed 12 May 2022]. 22. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med 2021; 384:989. 23. Ryan DH, Lingvay I, Colhoun HM, Deanfield J, Emerson SS, Kahn SE, et al. Semaglutide effects on cardiovascular outcomes in people with overweight or obesity (SELECT) rationale and design. Am Heart J 2020; 229:61–69. 24. Wilding JPH, Jacob S. Cardiovascular outcome trials in obesity: a review. Obes Rev 2021; 22:e13112. 25. EU Clinical Trials Register. A Qsymia CardiovascuLAr morbidity and Mortality (AQCLAIM) study in subjects with documented cardiovascular disease. 2013. www.clinicaltrialsregister.eu/ctr-search/search?query=AQCLAIM. [Accessed 12 May 2022]. 26. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JFE, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375:311–322. 27. Saxenda. liraglutide 6 mg/mL solution for injection in pre-filled pen, SmPC. Electronic Medicines Compendium2022. www.medicines.org.uk/emc/product/2313#gref. [Accessed 12 May 2022]. 28. Saxenda Prescribing Information. US Food and Drug Administration. 2018. www.accessdata.fda.gov/drugsatfda_docs/label/2018/206321s007lbl.pdf. [Accessed 12 May 2022]. 29. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375:1834–1844. 30. Drucker DJ. The cardiovascular biology of glucagon-like peptide-1. Cell Metab 2016; 24:15–30. 31. Muller MJ, Bosy-Westphal A, Heymsfield SB. Is there evidence for a set point that regulates human body weight? F1000 Med Rep 2010; 2:59. 32. Spiegelman BM, Flier JS. Obesity and the regulation of energy balance. Cell 2001; 104:531–543. 33. Muller TD, Blüher M, Tschöp MH, DiMarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov 2022; 21:201–223. 34. Frías JP, Davies MJ, Rosenstock J, Pérez Manghi FC, Fernández Landó L, Bergman BK, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med 2021; 385:503–515. 35. Sattar N, McGuire DK, Pavo I, Weerakkody GJ, Nishiyama H, Wiese R, Zoungas S. Tirzepatide cardiovascular event risk assessment: a pre-specified meta-analysis. Nat Med 2022; 28:591–598. 36. Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med 2022; 387:205–216. 37. Enebo LB, Berthelsen KK, Kankam M, Lund MT, Rubino DM, Satylganova A, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2·4 mg for weight management: a randomised, controlled, phase 1b trial. Lancet 2021; 397:1736–1748. 38. Lavie CJ, Arena R, Alpert MA, Milani RV, Ventura H. Management of cardiovascular diseases in patients with obesity. Nat Rev Cardiol 2018; 15:45–56. 39. Durrer Schutz D, Busetto L, Dicker D, Farpour-Lambert N, Pryke R, Toplak H, et al. European practical and patient-centred guidelines for adult obesity management in primary care. Obest Facts 2019; 12:40–66. 40. Forgione N, Deed G, Kilov G, Rigas G. Managing obesity in primary care: breaking down the barriers. Adv Ther 2018; 35:191–198. 41. Pétré B, Scheen A, Ziegler O, Donneau AF, Dardenne N, Husson E, et al. Weight loss expectations and determinants in a large community-based sample. Prev Med Rep 2018; 12:12–19. 42. Crémieux PY, Ledoux S, Clerici C, Cremieux F, Buessing M. The impact of bariatric surgery on comorbidities and medication use among obese patients. Obes Surg 2010; 20:861–870.
Comments (0)