
Remember me








Obesity is a health problem that affects individuals throughout their entire life cycle [1]. The prevalence of obesity in children and adolescents has increased worldwide over the past few decades [2].
Obesity and its metabolic comorbidities have both direct and indirect impacts on the heart. Studies involving echocardiography of obese adolescents and adults have revealed morphological alterations, including increased atrial and ventricular size, as well as left ventricular (LV) mass, while preserving overall systolic function as assessed by conventional parameters such as ejection fraction [3].
Newer ultrasound technology, such as two-dimensional speckle tracking (2D-ST), can detect subtle changes in heart function by evaluating myocardial deformation (strain, ε) in adolescents with metabolic conditions, including obesity [4–7]. Studies consistently report a decrease of 10–12% in LV global longitudinal strain (GLS) values when compared to patients without obesity [6,7]. It is still, however, a load-dependent tool (i.e. preload and afterload). To provide a more comprehensive understanding of LV function and energy expenditure, the assessment of myocardial work (MW) through strain–pressure curves has emerged as a novel approach. The incorporation of noninvasive arterial pressure into the analysis reduces its reliance on afterload [8]. Recently, this technique has been employed and validated in healthy adolescents [9].
Furthermore, the investigation of left atrial strain (LAε) has provided valuable insights into the comprehensive assessment of diastolic function, particularly in pediatric patients [10]. In the context of obesity, LAε has shown promise as a sensitive indicator of early diastolic dysfunction, as it progressively decreases with worsening LV diastolic dysfunction [11,12].
Nevertheless, the assessment of cardiac mechanics in obesity could be limited because of poor image quality (i.e. sound attenuation by adipose tissue).
The objective of this study was to assess the feasibility of obtaining these novel echocardiographic parameters, namely LAε, left ventricular strain (LVε) and MW, in severely obese adolescents. Additionally, the study aimed to explore potential associations between these parameters and variables such as body fat percentage, functional capacity and comorbidities associated with obesity.
Methods Study design and participantsThis descriptive cross-sectional study involved the recruitment of adolescents with obesity, aged between 12 and 18 years, who sought consultation in the obesity clinic from 2018 to 2020. Participants who had a height below 140 cm, were unable to engage in pedaling, had contraindications for cardiopulmonary testing or had known functional or structural heart disease were excluded from the study. The study obtained approval from the institutional ethics committee (approval no. 180124003), and appropriate consent was obtained from the parents or legal guardians of the participants. Additionally, assent was obtained from the participating adolescents themselves.
Participants were referred to the noninvasive cardiology laboratory, where they underwent the assessments on the same day, which included a nutritional assessment, a resting echocardiogram and a cardiopulmonary test. All patients had blood tests, which included assessments of fasting blood glucose, insulinemia, homeostatic model assessment (HOMA) index and lipid profile. The closest results of these tests to the visit were recorded. The presence of metabolic syndrome was determined using the modified Cook criteria [13].
Nutritional assessmentAnthropometric measurements, diet evaluation, blood pressure (BP) and body composition analysis were performed by a registered dietitian using standardized methods. Measurements of weight, height and waist circumference (WC) were obtained. BMI was calculated using the formula BMI = weight in kg/height in m2. Central obesity was defined as WC ≥90th percentile [14]. Nutritional status was determined based on the WHO 2007 curves, using the BMI z-score (zBMI). Obesity was classified as zBMI +2 to +2.99, while severe obesity was defined as zBMI ≥+3 [15].
BP was measured using a Critikon Dinamap Pro100 (Tampa, Florida, USA) pressure monitor, according to a standardized protocol [16]. High BP (HBP) was defined as SBP or DBP ≥90th percentile for age, sex and height [16].
Body fat percentage was assessed using a portable tetrapolar bioimpedance analyzer (Bodystat 1500MDD, Bodystat, Douglas, Isle of Man). Participants were categorized as having a fat percentage above or below the 95th percentile based on the study by Mueller et al. [17].
Baseline echocardiogramBefore the cardiopulmonary test, a highly experienced echocardiographer conducted an echocardiogram using a Vivid E95 system and an M5S transducer (GE Vingmed Ultrasound, General Electrics, Milwaukee, Wisconsin). The echocardiogram followed a standardized protocol based on guidelines published by Lopez et al. [18]. Anatomical and functional parameters were assessed using 2D imaging, color Doppler and tissue Doppler imaging. The LV end-diastolic and wall diameters, as well as the shortening fraction, were measured using 2D imaging in short-axis images. The LV volumes and ejection fraction were calculated using the 5/6 LV short-axis area multiplied by the length (bullet) formula.
For the analysis of LAε, LVε and MW, apical four-, three- and two-chamber views (4C, 3C and 2C) in 2D with a frame rate between 50 and 100 frames per second were obtained.
The BP was measured during the echocardiogram close to the apical acquisition using a Critikon Dinamap Pro100 pressure monitor.
Cardiopulmonary exercise testAll patients underwent a stress test on an upright bicycle (Lode Corival, Groningen, Netherlands). The exercise was conducted based on a ramp protocol, with increments every 3 min of either 20 W or 25 W, considering the patient’s age and level of physical activity. The test was considered satisfactory when the patient achieved the following criteria: reaching the oxygen uptake (VO2) plateau, reaching a heart rate greater than 85% of their maximum theoretical heart rate (as calculated by Tanaka’s formula) or having a respiratory exchange ratio (RER) greater than 1.0. Simultaneously, exhaled gas analysis was performed using the Ultima CardiO2 gas analyzer (MGC Diagnostics Corporation, St Paul, Minnesota). This analysis provided measurements of VO2, and VO2 at the ventilatory anaerobic threshold (VAT) and at maximum effort. VAT was estimated using V-slope method by two independent operators. Normal VO2 peak was defined as >80% of predicted values relative to the reference population based on age and sex [19]. VAT/VO2 peak was defined as normal at ≥40%. All these variables were expressed as a percentage of predicted [19].
Offline analysis of the new parameters: LAε, LVε and MWThe acquired images were analyzed using specialized software (EchoPAC version 204, GE Medical Systems, Milwaukee, Wisconsin), by a single operator.
The LAε analysis was performed using 4C and 2C images, with the QRS complex as the starting reference point (R–R gating). The first peak (between the R wave and the T wave) corresponds to the reservoir function (εR) and the second peak (starting at the P wave) to the atrial contractile function (εCT); and the difference between the two peaks reflects the conduit function (εCD, Fig. 1a) [11]. The values of εCT and εCD (negatives ε) are presented as absolute numbers.
 Fig. 1:
Fig. 1: New echocardiographic parameters in a 14-year-old female participant with severe obesity (zBMI + 3.5). (a) Atrial strain (LAε) with reference point the QRS complex (R–R gating). The first peak (between the R wave and the T wave) corresponds to reservoir function (εR), and the second peak (starting at the P wave) to atrial contractile function (εCT); and the difference between the two peaks reflects conduit function (εCD). Upper panel in four chambers and lower panel in two chambers. (b) Global and segmental myocardial work (MW). Upper panel: pressure-strain curves, in red is global curve and in yellow is selected segment in ventricular mid-anterior segment. Lower panel: bar graph of constructive myocardial work (green) and discarded work (blue), on the left is the ventricular anterior mid-anterior segment and on the right global average. Right panel: myocardial work bullseye (in mmHg%), by segment.
LVε was obtained by manual tracing of the region of interest in each view according to the manufacturer’s recommendations. After processing, if satisfactory tracking was not achieved after multiple manual adjustments by the operator, these segments were excluded. Peak systolic strain (ε) was recorded at any time during systole in each view (4C, 3C and 2C). GLS was then calculated as the average of peak systolic strain across the three views and presented as absolute values.
The analysis and acquisition of the various MW parameters followed the recommendations of Tretter et al. [9]. In summary, after obtaining the LVε, the closure and opening of the aortic and mitral valves were determined from the 3C image. The arterial BP obtained during the echocardiogram was then incorporated into the MW analysis, recording the following parameters (Fig. 1b) [9]:
(1) Global MW index (GWI): total MW from mitral valve closure to mitral valve opening (mmHg%). (2) Global constructive work (GCW): work performed during shortening in systole adding negative work during elongation in isovolumetric relaxation (mmHg%). (3) Global wasted work: negative work during elongation in systole adding work performed during shortening in isovolumetric relaxation (mmHg%). (4) Global work efficiency (GWE): constructive work divided by the sum of constructive and wasted work (0–100%).Exclusion of any segments in LVε and MW was reported and the feasibility of each new parameter (LAε, LVε and MW) was determined as follows:
(1) LAε: Percentage of participants with excellent or good tracking according to the operator. (2) LVε: Percentage of participants with no more than two segments excluded in total (4Cε, 3Cε and 2Cε) during the analysis. (3) MW: Same as LVε and the presence of adequate 3C images for the determination of aortic and mitral valves opening and closure. Statistical analysisBecause of the small number of subjects, the results are presented as median and interquartile range (IQR: Q1–Q3). To compare variables based on sex, body fat percentage or presence of comorbidities, nonparametric tests were used (Mann–Whitney U). The association between the new echocardiographic parameters and exercise capacity, as well as the results of the cardiopulmonary test, was evaluated using Spearman correlation. For all results, a P < 0.05 was considered statistically significant. IBM SPSS Version 25 (Armonk, New York: IBM Corp) was used for statistical analysis.
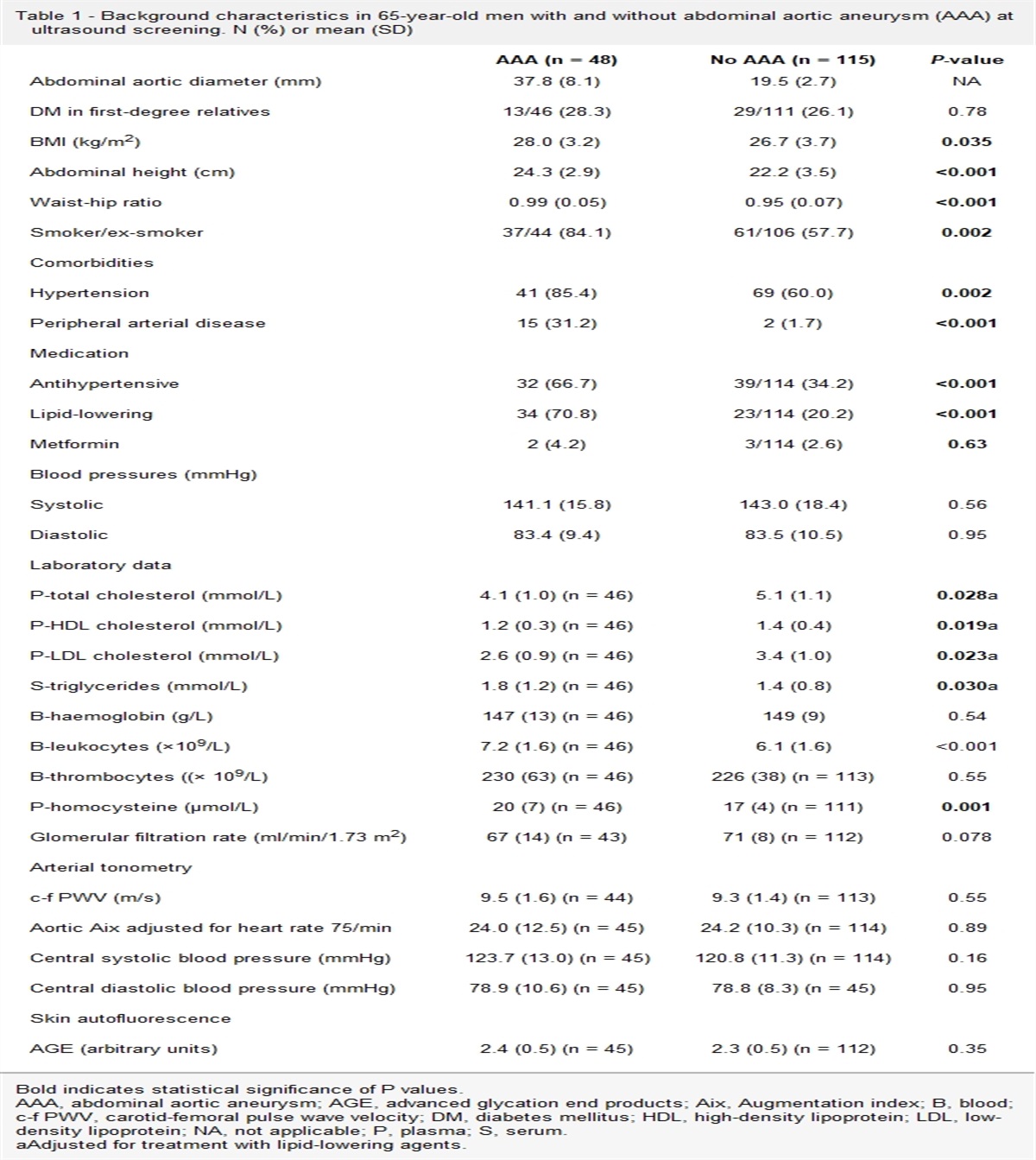
Results ParticipantsA total of 20 adolescents were recruited, 13 (65%) were males. The median age of the participants was 14.2 years (IQR: 12.9–14.9). Demographic and anthropometric data are summarized in Table 1, both overall and stratified by gender. Females were found to be older than males, with median ages of 14.6 years (14.1–15.4) and 13.5 years (12.5–14.7), respectively (P = 0.04). The median zBMI was 3.03 (2.87–3.14), and 14 participants (70% of the sample) had severe obesity (zBMI ≥ +3). Women had higher BMI values, but this difference disappeared when adjusted for age using zBMI. All participants had central obesity, with WC above the 90th percentile. The median fat percentage was 38.6% (36.5–41.2), and it was found to be higher in females compared with males: 41.2% (39.6–45.1) vs. 37.6% (32.7–38.9), P = 0.02. Of the total, 12 participants (60%) had a body fat percentage above the 95th percentile. Regarding comorbidities, 9 participants (45%) had HBP and 8 participants (40%) had metabolic syndrome, with no significant differences observed between males and females.
Table 1 - Demographic, anthropometric and clinical characteristics of the participants, total and by sex Variable TotalValues expressed as median (Q1–Q3) or n (%).
Bold values denote statistical significance (P < 0.05).
BIA, bioimpedance analyzer; BP, blood pressure; HOMA, homeostatic model assessment; WC, waist circumference; zBMI, BMI Z-score. Bold values denote statistical significance (p < 0.05)
The anatomical and functional results of the echocardiograms, including the new functional parameters, are summarized in Table 2. It was found that all patients had normal LV systolic function as assessed by shortening fraction. Three patients exhibited mild dysfunction (range: 48–53%) as determined by the ejection fraction, with no significant differences observed between males and females. Also, no differences by sex were observed in diastolic parameters (i.e. mitral E and E’ waves or left atrium area).
Table 2 - Echocardiographic anatomic, functional and the new parameters of left ventricular strain (LVε), left atrium strain (LAε) and myocardial work (MW) , total and by sex TotalValues expressed in median (Q1–Q3) or n (%).
ε2C, two-chamber strain; ε3C, three-chamber strain; ε4C, four-chamber strain; εCD, conduit function; εCT, atrial contraction function; εR, atrial reservoir function; GLS, global longitudinal strain; LA, left atrium; LAε, left atrial strain; LV, left ventricle; TAPSE, tricuspid annular plane systolic excursion.
The study of LAε, LVε and the MW was feasible in 95%, 100% and 100% of the participants, respectively. Only four participants (20%) had one segment excluded from the analysis of LVε and MW, one in 4C, two in 3C and one in 2C view. No participants had two or more segments excluded. All participants had adequate 3C images of the aortic and mitral valves for the MW analysis. Table 2 shows the results of LAε, LVε and the total MW and according to sex. The LVε (by GLS) was 19.1% (18.3–19.8) and in 4C 18.6% (17.8–20.1), with no differences by sex. The LAε showed εR of 38% (35.5–41.5), εCD of 27% (25–29) and εCT of 12% (9–14), with a tendency to worse εCD, 26% (20–27) in women vs. 28% (26.3–32.8) in men, P = 0.07. Regarding MW parameters, global work index was 1860.5 mmHg% (1591–2015.5), global work constructive 2055 mmHg% (1802–2310.8) and GWE 96% (95–97), with no differences by sex.
Cardiopulmonary exercise testAll participants performed a satisfactory cardiopulmonary exercise test, with RER > 1 or >85% of maximum heart rate. Supplementary Table 1, Supplemental digital content 1, https://links.lww.com/CAEN/A58 summarizes the main findings, both overall and stratified by sex. A decreased VO2 peak was observed in the participants, with a VO2 peak 1935.5 ml/min (1660–2099), corresponding to 67.1% (55–84.3) of that predicted by sex and age. This decrease was more pronounced in male participants with 57.1% (51.5–67.1) of predicted vs. female with 84.5% (82.5–87.3) of predicted, P = 0.001. The VAT was obtained on average at 44.5(39–47.8) of VO2 peak, which is in the low range of normality, with no differences by sex.
Association between new echocardiographic parameters according to body composition and comorbiditiesAdolescents who had a body fat percentage greater than or equal to the 95th percentile according to sex and age, presented similar LVε, both GLS and for each view (4Cε, 3Cε or 2Cε), but lower MW index: 1691 mmHg% (1528–1909) vs. 2063 mmHg% (1831–2263), P = 0.01, lower work efficiency: 95.5% (94.3–96.8) vs. 97% (96–98), P = 0.02 and a trend to lower overall constructive work: 1936 mmHg% (1732.5–2137) vs. 2310 mmHg% (1955–2336), P = 0.08 (Fig. 2a–c).
 Fig. 2:
Fig. 2: Box and whiskers plot of new echocardiographic functional parameters. (a—c) Left ventricular strain and myocardial work parameters according to percentile (<95 or ≥95) of body fat %. (d–f) Left atrial strain parameters according to percentile (<95 or ≥95) of body fat %. All longitudinal strain (ventricular and atrial) parameters are expressed as absolute values. 4C, apical four chambers view; LA, left atrium; LV, left ventricle.
Differences were also observed in atrial function, with lower εR [36.5% (34–39.8) vs. 42.5% (37.8–49.8), P = 0.024] and lower εCD [26.5% (24.3–27.8) vs. 33% (26.8–38.5), P = 0.02] in participants with higher body fat percentage, with no difference in εCT (Fig. 2d–f).
When classifying participants according to presence of comorbidities (Fig. 3), lower LVε in 4C was observed in participants with vs. without metabolic syndrome: 17.8% (17.5–19.3) vs. 19.3% (18.3–20.3), P = 0.046, similar to participants with vs. without HBP: 17.8% (17.5–18.6) vs. 19.7% (18.4–20.3), P = 0.02, with no differences between groups when comparing GLS, 2C or 3C or other functional parameters. Participants with metabolic syndrome exhibited lower work efficiency compared with those without the condition when evaluating MW. For participants with HBP, there was an increase in both GWI (P = 0.046) and GCW (P = 0.038), and trended toward a decrease in work efficiency (P = 0.056). Neither metabolic syndrome nor HBP appeared to influence LAε variables (εR, εCD or εCT) in the studied adolescents.
 Fig. 3:
Fig. 3: Box and whiskers plot of new echocardiographic functional parameters. (a–c) According to the presence of metabolic syndrome. (d–g) According to the presence of high blood pressure (HBP). All longitudinal strain (ventricular and atrial) parameters are expressed as absolute values. 4C, apical four chambers view; LA, left atrium; LV, left ventricle.
Association and correlations with cardiopulmonary exercise testingOf all the parameters evaluated, the only echocardiographic tools with significant correlations with exercise capacity parameters (Supplementary Table 2, Supplemental digital content 1, https://links.lww.com/CAEN/A58) were GLS (absolute value) and VAT (ρ, −0.58, P = 0.01) and εCD and VO2 (% predicted) (ρ, −0.49, P = 0.03), but these correlations did not have a clear physiological significance.
DiscussionThis study shows that the use of new 2D-ST myocardial deformation tools such as LVε, LAε and MW analysis is a feasible technique to perform in adolescents with severe obesity. The application of these novel parameters revealed changes not detected in conventional systolic and diastolic parameters such as ejection fraction, or tissue Doppler velocities. Importantly, new parameters such as LV global work index, LAε reservoir and conduit function, displayed alterations in participants with higher body fat. Additionally, LV 4Cε and work efficiency were reduced in individuals with metabolic syndrome and HBP, conditions known as precursors to cardiovascular damage.
The subclinical systolic and diastolic dysfunction revealed in some of our participants by the new echocardiographic parameters may be attributed to myocardial damage in the presence of higher body fat percentage or metabolic comorbidities of obesity (i.e. HBP, or metabolic syndrome). These comorbidities could directly affect the myocardium or are indicators of prolonged or more severe exposure to obesity. One possible explanation for this finding is the excessive accumulation of fat, including epicardial fat, and its detrimental effects on the heart. First, it increases mechanical stress on both ventricles, resulting in an elevated cardiac workload and LV hypertrophy and aggravating the atrial enlargement and ventricular diastolic dysfunction because of reduced compliance [20–23]. Second, epicardial fat is associated with a higher proportion of inflammation-promoting genes and the secretion of proinflammatory adipokines. This leads to local and systemic proinflammatory cytokines that contribute to oxidative stress, cardiomyocyte disarray, fibrosis and infiltration of adipocytes into the myocardium, disrupting cardiac metabolism by promoting excessive utilization of free fatty acids [24,25]. Cardiac magnetic resonance studies could be a valuable next step, as they can evaluate both the presence and magnitude of epicardial fat, along with systolic and diastolic functions. Additionally, incorporating serological markers of inflammation might provide a more comprehensive assessment.
In our study, diastolic function, evidence compromise in participants with higher body fat percentage only assessed by LAε parameters (i.e. εR and εCD). Steele et al. [12] reported comparable results in adolescents and young adults with obesity and diabetes, even in subjects with normal atrial volume, with no compromise of the εCT. While limited literature supports this preserved atrial contraction behavior, it could be attributable to the young population studied, as compromise in contractile function might emerge later in time.
The study of LVε in our adolescents showed a similar reduction in GLS to those published in other studies in children and adolescents with obesity [6,7]. In our study, it stands out that only 4Cε showed association with comorbidities such as HBP or metabolic syndrome. This association found exclusively in this view and not in the others or in GLS may be explained by the better definition of both walls that allow optimal tracking, despite the fact that there was no major difference in our study in the segments excluded in the different views. The study of strain exclusively from the 4C view could be a useful tool in certain contexts where regional or segmental involvement is not anticipated [26,27] or when suboptimal images are obtained because of variations in body size. Focusing on the 4C view alone allows for optimization of time and performance in such situations, with similar performance to GLS [27].
The recent addition of MW evaluation through strain–pressure curves in echocardiography, combined with 2D-ST, has emerged as a valuable approach. This method allows for the assessment of LV function and metabolism by incorporating noninvasive arterial pressure into the analysis. It provides insights into myocardial performance and oxygen consumption independently of afterload [8]. Paysal et al. [28] conducted one of the few studies that evaluated the impact of nutritional disorders using MW. They found baseline regional differences in MW in adolescents with anorexia, obesity and controls. This highlights the potential of MW as a valuable tool in identifying cardiac abnormalities in these patient populations (I). The MW obtained in our study shows comparable results to those published by Tretter et al. [9] in 52 healthy adolescents of comparable age. They report a mean global work index of 1802.0 ± 264.4 mmHg%, whereas in our work we found a median of 1860.5 mmHg% (1579–2022.5). Similar findings were also observed in overall constructive work [2054.5 ± 297.3 mmHg% vs. our 2055 mmHg% (1802–2310.8)] and overall work efficiency [95.5 ± 1.1% vs. our 96% (95–97)]. Strikingly, although these results are comparable to a population without obesity when grouping patients according to body fat percentage or presence of comorbidities, differences are observed in both MW and LAε that were not demonstrated with other conventional systolic or diastolic function parameters, or even with LVε. This suggests that the use of these new tools could demonstrate subclinical impact of myocardial involvement in different obesity-related conditions.
The lack of correlation of these new echocardiographic parameters with cardiopulmonary test variables may be related to the limitations of performing the cardiopulmonary test in patients with obesity and its comparison with the reference population [29]. Although multiple adjustments for body composition have been attempted, they have not shown consistent results in relation to the effect of obesity on exercise capacity [30,31]. On the other hand, the presence of early echocardiographic alterations by new assessment methods may not yet be reflected in the exercise parameters evaluated in this study.
LimitationsBecause of the small number of participants in this pilot study, there are some associations that may not appear because of a lack of statistical power. Despite this, we were able to demonstrate interesting differences or trends that allow us to project this line of research in the future.
Nor was a control group recruited that could compare these parameters and thus better understand their behavior under both normal and pathological conditions. In a future study, it would also be interesting to compare it with athletes, to evaluate the full potential impact of these parameters in the complete spectrum of nutritional states and physical capacity.
ConclusionThis study shows that echocardiographic assessment of LAε, LVε and MW are feasible to study in adolescents with obesity, even severe obesity. Participants with higher body fat percentage had lower LAε and MW and in those with metabolic syndrome or HBP, lower LVε was demonstrated in 4C. Functional echocardiographic measurements, however, both conventional and these new myocardial mechanics parameters, did not correlate with exercise capacity.
These new measurements open a potential area of study that not only encompasses the impact of obesity in adolescents but also makes it possible to distinguish those at higher cardiovascular risk, associated with obesity cardiometabolic complications.
AcknowledgementsThis study is supported by the initial research fund of the Division of Pediatrics of the Pontificia Universidad Católica de Chile.
Conflicts of interestThere are no conflicts of interest.
References 1. World Health Organization. Ending childhood obesity. WHO Library; 2016. 50 p. https://apps.who.int/iris/bitstream/handle/10665/204176/9789241510066_eng.pdf 2. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017; 390:2627–2642. 3. Koopman LP, Mertens LL. Impact of childhood obesity on cardiac structure and function. Curr Treat Options Cardiovasc Med 2014; 16:345. 4. Yoldaş T, Örün UA, Sagsak E, Aycan Z, Kaya O, Özgür S, et al. Subclinical left ventricular systolic and diastolic dysfunction in type 1 diabetic children and adolescents with good metabolic control. Echocardiogr 2018; 35:227–233. 5. Samiei N, Bayat M, Firouzi A, Dehghani F, Parsaee M, Rahimi S, et al. Subclinical systolic and diastolic dysfunctions in patients with metabolic syndrome and angiographically normal coronary arteries: an echocardiographic study. J Clin Ultrasound 2018; 46:195–201. 6. Labombarda F, Zangl E, Dugue AE, Bougle D, Pellissier A, Ribault V, et al. Alterations of left ventricular myocardial strain in obese children. Eur Heart J Cardiovasc Imaging 2013; 14:668–676. 7. Mangner N, Scheuermann K, Winzer E, Wagner I, Hoellriegel R, Sandri M, et al. Childhood obesity: impact on cardiac geometry and function. JACC Cardiovasc Imaging 2014; 7:1198–1205. 8. Scatteia A, Baritussio A, Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance. Heart Fail Rev 2017; 22:465–476. 9. Tretter JT, Pradhan S, Truong VT, Mullikin A, Mazur W, Hill GD, et al. Non-invasive left ventricular myocardial work indices in healthy adolescents at rest. Int J Cardiovasc Imaging 2021; 37:2429–2438. 10. Mawad W, Friedberg MK. The continuing challenge of evaluating diastolic function by echocardiography in children. Curr Opin Cardiol 2017; 32:93–100. 11. Cho GY, Hwang IC. Left atrial strain measurement: a new normal for diastolic assessment? JACC Cardiovasc Imaging 2020; 13:2327–2329. 12. Steele JM, Urbina EM, Mazur WM, Khoury PR, Nagueh SF, Tretter JT, et al. Left atrial strain and diastolic function abnormalities
Comments (0)