1. IntroductionArterial hypertension (AHT) is the leading preventable cause of premature death worldwide [
1]. Left ventricular hypertrophy (LVH) is one of the most important prognostic markers in AHT and a predictor of mortality [
2]. Blood pressure (BP)-lowering treatment reduces LVH [
3] and the rate of a composite cardiovascular endpoint [
4]. LVH can be caused not only from AHT, but also from, to name a few causes, aortic valve stenosis [
5,
6] and hypertrophic cardiomyopathy (HCM). The differentiation between hypertension-mediated LVH and HCM can be difficult in the daily routine, but essential for the treatment. Cardiac magnetic resonance imaging (CMR) can be especially helpful for the discrimination between HCM and hypertensive heart disease (HHD) [
7].The 1988 Framingham Heart Study detected LVH in 16% of the men and in 19% of the women in the general population with or without AHT by echocardiography. Especially in the youngest age groups in this study, LVH was more prevalent in men, whereas, in older subjects, it was more prevalent in females [
8]. These echocardiographic data are more than 30 years old. Since then, the definitions for AHT, the indications for performing echocardiography and the technical means for diagnosis have changed. Population-based studies, including the Atherosclerotic Risk in Communities and the PAMELA studies, have examined the prevalence of the different geometry patterns, and this topic was also covered in a review article [
9,
10,
11,
12]. However, none of these studies analysed the amount of LVH, and there is no information on the prevalence of severe LVH and the characteristics of these patients.Lehtonen et al. only applied electrocardiography, a less sensitive method, which detected a positive Sokolow-Lyon index as a marker of LVH in 11–13% patients with an AHT [
13]. In a very selective cohort of patients with known AHT and normal electrocardiogram (ECG), the prevalence of LVH was reported as 8% [
14].
The aim of this study is to examine the prevalence of LVH in patients with AHT by echocardiography and, specifically, to describe patients with severe LVH in AHT.
3. Results 3.1. Baseline CharacteristicsThe study population included 422 patients. Due to insufficient echocardiography documentation or image quality, 22 patients had to be excluded, resulting in a final study population of 400 patients. One hundred and seventy-seven (44.3%) patients were women. The median age of the overall cohort was 56 years (IQR 43–70 years). One hundred and thirty patients (37.2%) had a secondary form of AHT. The median of the systolic and diastolic 24 h mean, awake and asleep BP was not in the target range (24 h mean ambulatory BP (ABP) ≥ 130/80 mmHg and/or awake ABP ≥135/85 mmHg and/or asleep ABP ≥ 120/70 mmHg) [
18]. Complete baseline characteristics are shown in
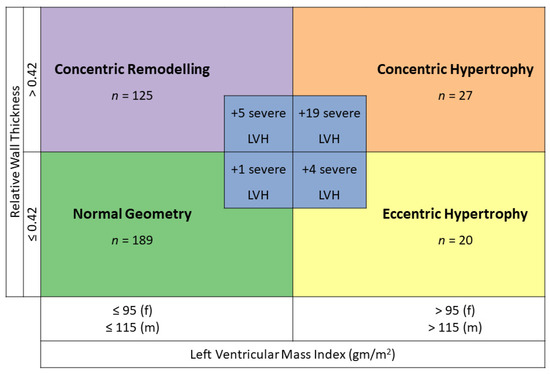
Table 1. 3.2. Prevalence of Left Ventricular HypertrophyBoth LVMI and relative wall thickness were available in 400 patients. Twenty percent of our patients (80 patients) had a concentric or eccentric LVH, thus a hypertensive heart disease related to the geometry. One hundred and ninety patients (47.5%) had a normal geometry, one hundred and thirty (32.5%) a concentric remodelling, fifty-six (14.0%) a concentric hypertrophy and twenty-four (6.0%) an eccentric hypertrophy (
Figure 1). Overall, more than half of our patients (52.5%) with AHT had an abnormal geometry. We identified 29 patients (7.3%) who had a severe LVH in echocardiography. A severe LVH could be found in all geometry forms. If geometry was classified according to the guidelines in those patients with severe LVH, 1 (3.4%) classified as normal, 5 (17.2%) as concentric remodelling, 19 (65.5%) as concentric hypertrophy and 4 (13.8%) as eccentric hypertrophy (
Figure 1). The percentage of men was significantly higher in the group with severe LVH than in the group with normal geometry (75.9% vs. 48.7%, p value 0.009). The prevalence of LVH in patients with an AHT according to gender is shown in
Figure 2. 3.3. Severe Left Ventricular Hypertrophy vs. No Left Ventricular Hypertrophy and vs. Left Ventricular HypertrophyThere were 29 patients with severe LVH and 189 patients without LVH. The differences between patients with severe LVH and patients without LVH are shown in
Table 2.
Patients with severe LVH were excluded from the other groups of LV geometry.
There was a significant male predominance in patients with a severe LVH in comparison to patients without LVH (75.9% vs. 48.7%, p-value 0.009). Patients with a severe LVH were significantly older (64.9 years) than those without LVH (50.4 years, p-value 0.001). Secondary forms of AHT were significantly more common in the group with the severe LVH than in the group without LVH (60.0% vs. 29.5%, p-value 0.005).
Patients with a severe LVH had a significantly higher systolic and diastolic BP regarding the 24 h mean, awake and asleep ABPM values in comparison to patients without LVH (
Table 2).
Patients with a severe LVH had significantly more often a coronary heart disease (37.9% vs. 19%, p-value 0.029) than patients without LVH. Patients with a severe LVH were also more likely to have a lower eGFR (eGFR mean 59.0 mL/min vs. 93.0 mL/min, p-value < 0.0005) and albuminuria > 3.4 mg/mmol (58.8% vs. 12.5%, p-value < 0.0005) as comorbidities compared to patients without LVH.
Significantly more people with a severe LVH had a therapy with diuretics (65.5% vs. 19.7%, p-value < 0.0005) and an antihypertensive triple therapy (44.8% vs. 14.3%, p-value < 0.0005) than patients without LVH. There was no difference in therapy with ACE inhibitors, ARB or calcium channel inhibitors between patients with a severe LVH and patients without LVH.
Though there was a trend, there were no significant differences regarding a positive Sokolow-Lyon index between the two groups, 11.1% in the group with severe LVH und 2.4% in the group without LVH (p-value 0.056). In contrast, we found significantly more T-wave changes, i.e., a negative T-wave in at least one lead V4-V6, in the ECG of patients with a severe LVH compared to patients without LVH (18% vs. 4.1%, p-value 0.014). However, 2 of the 29 patients with severe LVH did not have an ECG.
The Sokolow-Lyon index had a sensitivity of 11%, a positive predictive value of 19%, a specificity of 96% and negative predictive value of 93% for severe LVH in our study.
The differences between patients with severe LVH and patients with LVH but a septal thickness
Table 2. There were 57 patients with non-severe LVH. Especially diastolic BP was significantly higher in the 24 h mean, awake and asleep values in the group with severe LVH in comparison to the patients with non-severe LVH. There were no significant differences in comorbidities, including secondary forms of AHT and antihypertensive medication, between the patients with severe LVH and patients with non-severe LVH. 3.4. Gender Differences Regarding Blood Pressure across All Geometries Women with a severe LVH had significantly higher systolic 24 h mean, awake and asleep ABPM values than women with all other geometries; women with a severe LVH also had higher diastolic asleep values, with a trend for higher diastolic 24 h mean and awake values, although post hoc analyses support only the systolic findings (
Figure S1). In men, however, this association was less pronounced and visually only observable in systolic values (
Figure 3). Women with eccentric hypertrophy showed a trend towards lower systolic and lower diastolic 24 h mean, awake and asleep ABPM values than the other groups, whereas, in men, there was no difference between the ABPM values in those groups (
Figure 3). Post hoc analyses in men showed only significant differences for systolic and diastolic asleep values between patients with a severe LVH and patients with a normal geometry (
Figure S1). Patients with a severe LVH showed significantly more uncontrolled systolic and diastolic BP at night than those with a normal geometry (
Figure S2). There was no association between the duration of AHT and the presence of severe LVH. 3.5. Differences Regarding Blood Pressure across All Geometries The predominant geometry across patients with and without controlled BP was a normal geometry. Patients with uncontrolled systolic or diastolic BP had more frequently a severe LVH. Patients with an uncontrolled systolic BP also had more frequently a concentric hypertrophy. This effect was most apparent in the asleep BP values (
Figure 4). There were no significant differences regarding the AHT duration between patients with and without severe LVH (
Table 2,
Figure 5), although most patients without LVH had a short AHT duration documented, whereas more patients with a more severe form of LVH had a longer AHT duration. 4. Discussion
In our contemporary population of patients referred to a hypertension clinic of a tertiary hospital, 7.25% of all included patients with AHT had a severe LVH and 14.25% a concentric or eccentric LVH, i.e., a hypertensive heart disease based on the LV geometry. Patients with a severe LVH were more likely male and older than patients with a normal LV geometry. Furthermore, they had a higher BP, more antihypertensive medications and comorbidities. These variables can be regarded as markers of more severe forms of AHT. However, it is unclear how adherence was in patients who had to take many medications. Interestingly, there was no statistical significance regarding the duration of AHT, although, numerically, the duration was longer in patients with severe LVH.
Many included patients were relatively recently diagnosed with AHT (median 23 months). However, it is never certain how long the AHT existed before diagnosis. Patients with severe LVH had a tendency to have had AHT longer, although since this was possibly due to the small number of patients, this result was not significant.
Patients with a severe LVH had significantly higher systolic and diastolic BP values than patients with a normal LV geometry. In comparison to patients with a concentric or eccentric hypertrophy, only the diastolic values were significantly higher in patients with severe LVH. Furthermore, patients with a severe LVH had significantly more often uncontrolled systolic and diastolic 24 h mean BP values, again only for diastolic values in comparison to patients with concentric or eccentric hypertrophy. Considering that the severe LVH is most likely a consequence of the higher BP values, this seems, at first glance, to be a contradiction to the well-known data of the Dublin outcome study [
19], which showed that the systolic asleep values in particular are most important for prognostic purposes. One key to this may be in the gender distribution. In the Dublin outcome study, 55% of the participants were women, as were 44% of the participants experiencing a cardiovascular death. In our study, fewer women (44%) were included, and only 24% of those patients with a severe LVH were female. Referring to
Figure 3 and
Figure S1, women with severe LVH have higher systolic and diastolic values, whereas, in men, it is numerically only the diastolic values. Therefore, the male dominance in our study could have caused the focus of the diastolic value in our data for the prediction of LVH.With regard to other target organ damage, we could only determine statistical significance with regard to coronary heart disease, albuminuria and eGFR between the patients with severe LVH and patients with normal LV geometry. It has been shown that proteinuria is a very good prognostic parameter to predict long-term cardiovascular events in hypertensive patients [
20]. Our study population was probably too small, or the prevalence of stroke, transient ischemic attack or peripheral arterial disease were too low, to find statistical significance. On the other hand, there were many patients who were recently diagnosed with AHT, so they may not have had any cardiovascular events yet [
21].Surprisingly, only 11% of the patients with a severe LVH and, in contrast, 4 of patients (2.4%) with normal left ventricular geometry had a positive Sokolow-Lyon index, which is recommended in the ESC guidelines 2018 for screening of hypertension-mediated organ damage (HMOD) [
16]. Considering its low sensitivity of 11%, the use of ECG for the detection of LVH should be questioned, although the specificity is high with 96%. Lehtonen et al. reported in their study on the prevalence and prognosis of ECG abnormalities in normotensive and hypertensive individuals [
13] a significant increase of ST/T changes in participants with a Grade 2 AHT in comparison to normotensive participants. Overall, positive Sokolow-Lyon indices were more prevalent in this study than in ours, possibly due to the higher number of patients with AHT included (n = 1497 vs. n = 400 in our study). Furthermore, the true prevalence of LVH in this cohort is not known. The study on the performance of Sokolow-Lyon index in detection of echocardiographically diagnosed LVH in a normal Eastern German population shows that the correlation of the Sokolow-Lyon index and echocardiographic parameters of LVH is weak. Sensitivity of the Sokolow-Lyon index was 5% and the specificity 95% in this study [
22] similar to our study (sensitivity 11% and specificity 96%). It is therefore questionable whether the Sokolow-Lyon index is suitable for diagnosing LVH.
Interestingly, patients with severe LVH had significantly more negative T waves (18% vs. 4%) in the ECG in the leads representing the anterolateral wall, resulting in a sensitivity of 19% and a specificity of 92%. This ECG change appear to be a more sensitive, though less specific parameter, in comparison to the Sokolow-Lyon index, for the LVH in the ECG in our patient population.
Repolarization abnormalities are very common in patients with HCM [
23] and can be a sign of a sarcomeric form of the disease. HCM is defined by the presence of increased LV wall thickness over 15 mm, which is not solely explained by abnormal loading conditions [
7]. HCM cannot be diagnosed with certainty on echocardiography alone [
24]. CMR markers such as native myocardial T1 mapping, late gadolinium enhancement or global longitudinal strain might be helpful; however, CMR was too rarely ordered in our study to be able to make a statement in this regard [
25]. Further factors potentially helping in the differentiation between severe LVH due to AHT and HCM might be age, location of the hypertrophy and remodelling over time or the MESA index; however, these parameters were not studied in our cohort.
Limitations of our study are the small study population, the selection of patients of a dedicated hypertension clinic and the low number of CMRs ordered for the differentiation of causes of severe LVH. Due to the low number of patients included, we did not find a statistical significance for some typical target organ damages of AHT. This may be augmented by the large number of patients recently diagnosed with AHT. We only studied echocardiographies in patients with known AHT; therefore, no healthy controls were included. Moreover, we did not assess any longitudinal data. There were no echocardiographies available before the occurrence of AHT. On the other hand, there is a good comparability between the echocardiographic examinations of the patients, since only patients from our specialised clinic were included and almost all patients received had their echocardiography taken on the same machine and were supervised by the same two experienced cardiologists (TB, ASV). Due to the retrospective nature of the study, we did not have access to home BP measurements, which were not available in all patients at the same quality. Furthermore, we did not have any information on the presence of retinopathy in the majority of patients.
An unanswered question is whether severe LVH is caused solely by AHT, or if there is an overlap with HCM. Further studies are needed to evaluate the usefulness of CMR and/or genetic testing in patients with severe LVH in the context of AHT.


Comments (0)