The development of robot-assisted spinal surgery (RASS)
Robot-assisted spine surgery (RASS) has undergone a significant evolution since its initial application in spinal surgery in the 1990 s, transitioning from basic exploratory stages to a mature and widely adopted technique. With continuous technological advancements, RASS has evolved from a simple robotic arm system into a multifunctional and highly precise tool for spinal surgical assistance [7]. In spinal procedures, the placement of pedicle screws is crucial, serving to stabilize the spinal structure. This technique is extensively used in the treatment of spinal deformities, fractures, degenerative diseases, and tumors, representing a major milestone in the development of spinal surgery [8]. However, due to the proximity of the pedicle to nerve roots, the spinal cord, and blood vessels, screw placement carries certain risks and potential complications. Therefore, improving the accuracy of screw placement has always been a critical goal in pedicle screw fixation techniques [9].
With the advancement of medical imaging and computer technologies, image navigation and robotic systems have gradually been applied to pedicle screw placement. Renaissance was the first robotic system approved by the FDA for use in spinal surgery [10], and systems such as SpineAssist and Mazor X have garnered widespread global attention and application [11,12,13,14]. Studies have shown that robot-assisted surgery can enhance screw accuracy, reduce radiation exposure, and lower complication rates. However, some literature has reported inconsistent performance in robotic screw placement accuracy. Even prospective randomized controlled trials and meta-analyses have indicated that robotic-assisted placement may not always outperform manual or percutaneous screw placement [15]. These discrepancies may be attributed to factors such as disease type, patient-specific differences, and variations in surgical protocols. It is noteworthy that most spinal surgery robots are semi-autonomous, with many operative steps still requiring manual execution by surgeons, suggesting that multiple factors in clinical practice may influence placement accuracy.
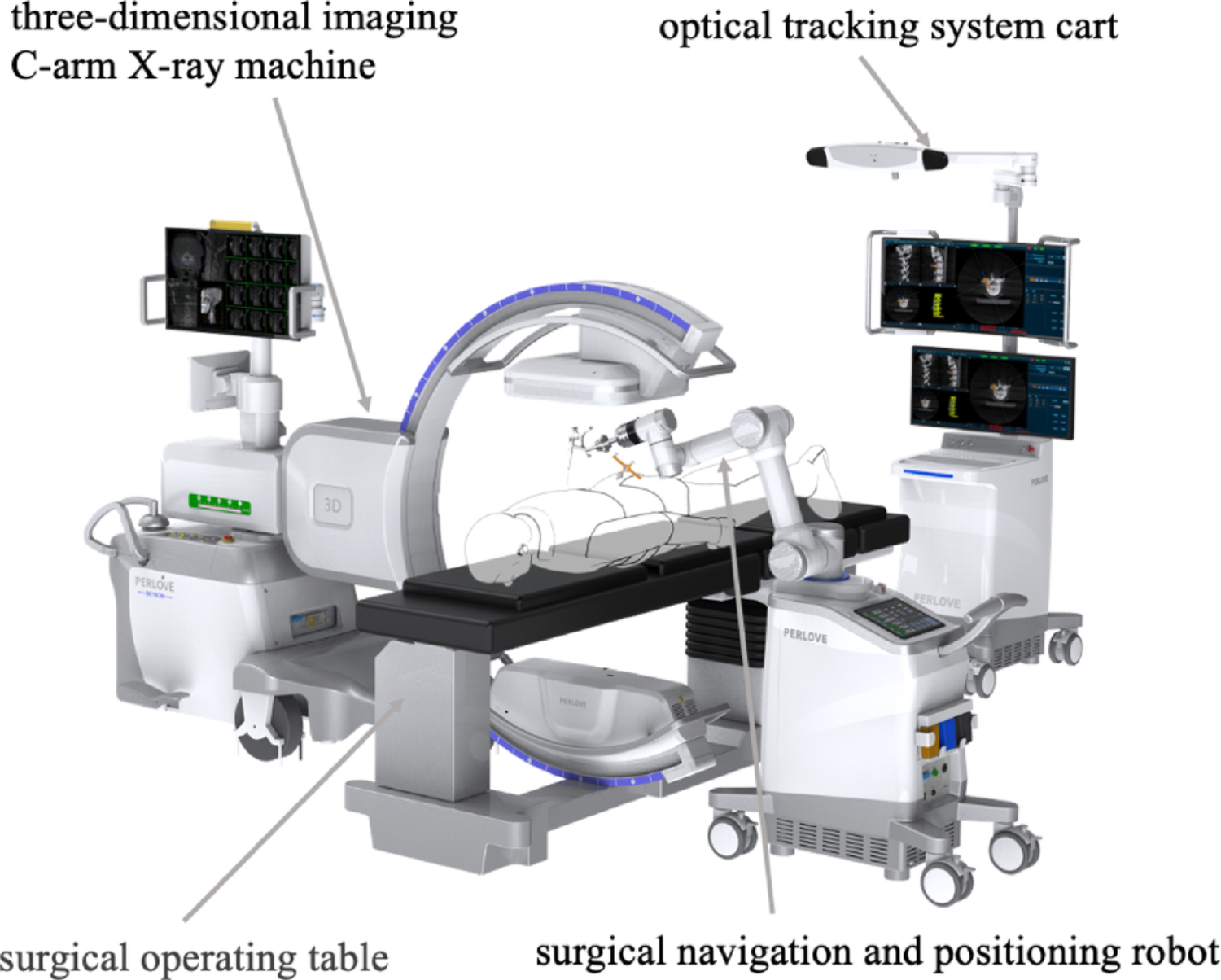
Currently, most spinal surgery robots focus primarily on guiding the trajectory of pedicle screws, assisting surgeons in identifying the optimal insertion path. However, the actual insertion of K-wires and screws remains manual [16]. Addressing this limitation, the ORTHBOT system is the first to achieve automated K-wire insertion, surpassing the traditional navigation-only capability [5]. Its pressure monitoring and cortical wall protection function enables real-time surveillance of pressure changes during insertion, simulating tactile feedback and stopping automatically when abnormal conditions are detected, thereby preventing cortical breach. Furthermore, ORTHBOT is equipped with a binocular visible light navigation system for close-range surgical monitoring, reducing external interference and improving operational efficiency. Its non-invasive, contact-free localization technology avoids the need for invasive bone-mounted markers, significantly reducing surgical trauma to patients [3]. Additionally, its multimodal fusion of preoperative and intraoperative imaging shortens intraoperative planning time and minimizes radiation exposure for both surgeons and patients, offering enhanced precision and safety in spinal surgery.
Numerous studies have demonstrated that RASS presents a relatively short learning curve for pedicle screw placement. Shi and Chen retrospectively analyzed 95 patients (541 screws) who underwent robot-assisted spinal surgery using the ExcelsiusGPS system to assess the learning curve and proficiency development. The results showed that total operative time significantly decreased after approximately 14 cases, and screw insertion time improved after about 13 cases, indicating that surgeons can rapidly acquire key skills for robot-assisted surgery. Interestingly, robot registration time remained relatively unchanged, and the trends persisted even after controlling for fusion segment number, supporting the notion of a short learning curve and rapid skill acquisition, which bolsters the clinical adoption of RASS. Feng and Fan conducted a comparative cohort study involving 199 patients who underwent posterior pedicle screw fixation, with two junior surgeons performing screw insertions under senior expert supervision. A total of 769 screws were inserted in the robot group and 788 in the manual group. The study found that in the upper thoracic segment, the robot group had a shorter learning phase, while longer learning periods were observed in the lower thoracic and lumbosacral segments. Overall, the robot group exhibited a gentler learning curve slope, and the accuracy of screw placement in the upper thoracic region was significantly higher in the robot group (89.4% vs. 76.7%, P < 0.001), with more pronounced differences in deformity cases. Although the robot group had slightly shorter screw placement times in the upper thoracic region, the manual group performed faster in lower thoracic and lumbosacral regions, with three screw-related neurological complications occurring exclusively in the manual group. These results suggest that robotic assistance offers significant advantages in the upper thoracic region and in cases of deformity, allowing junior surgeons to quickly grasp critical skills and achieve high accuracy and safety even in early adoption stages. Whether utilizing specialized navigation systems like ExcelsiusGPS® or targeting specific procedures such as percutaneous pedicle screw placement or vertebroplasty [17], surgeons can significantly shorten operation time and master robot registration and insertion techniques after roughly a dozen cases. Some literature has emphasized the consistent superiority of robotic screw placement in upper thoracic and structurally deformed cases [18], even in early use. With increasing experience and proficiency, overall operation time, radiation exposure, and complication rates in robot-assisted surgery can be effectively maintained at low levels [19,20,21,22], providing further support for the clinical implementation of RASS.
RASS not only assists with pedicle screw placement but is also widely applicable in the comprehensive treatment of spinal deformities, tumor resection, fracture repair, and degenerative diseases [23]. Despite challenges such as high equipment costs and complex operations, RASS is increasingly becoming a key component of spinal surgery as the technology matures and gains acceptance in major healthcare institutions.
Risk factors for pedicle screw misplacement
The accuracy of pedicle screw placement is one of the key determinants of success in spinal surgery. Misplacement of screws can lead to postoperative complications such as thrombosis, fixation failure, and chronic pain. Even in RASS, the risk of screw deviation remains a concern [24,25,26,27]. Studies have shown that osteoporosis (especially with T-scores below − 3.5), high degrees of spinal rotation (Nash-Moe grade ≥ II), and severe facet joint degeneration (Fujiiwara-MRI grade ≥ III) all significantly increase the likelihood of cortical breach and facet joint violation [1, 25, 28]. In this study, two patients with Grade E screws had all three of the above high-risk factors, suggesting that degenerative spines and reduced bone density pose significant challenges to the navigation accuracy of RASS [29]. Additionally, for severely obese patients, those with osteoporosis, or cases requiring screw placement more than three segments away from the reference point, surgeons must exercise heightened caution to avoid postoperative complications due to unsatisfactory screw positions [3].
From a clinical translation perspective, our analysis of risk factors highlights the necessity of implementing precision strategies for specific patient populations. For patients who are elderly (≥ 65 years), have low bone density (T≤−2.5), spinal rotation ≥ Grade III, or facet joint degeneration ≥ Grade III, it is essential to enhance preoperative bone density assessment and quantify spinal rotation. For T-scores ≤−3.5, preoperative planning for cement augmentation or using cortical screws may improve screw anchorage. This should be combined with intraoperative image guidance and manual adjustments. Furthermore, robotic systems should be optimized to address issues such as thick soft tissue and positioning changes by developing specialized puncture channels and improving registration algorithms.
Although RASS can utilize 3D imaging and robotic navigation to reduce errors, it still largely depends on manual execution by the surgeon. Therefore, reducing placement errors in high-risk populations has become a new research focus. The ORTHBOT system used in this study incorporates intelligent needle insertion and pressure monitoring cortical protection features, aiming to address complex conditions such as spinal degeneration and osteoporosis more effectively than existing systems. For example, its real-time pressure monitoring allows the system to shut down promptly when encountering abnormal resistance in cartilaginous or osteoporotic bone, minimizing potential injury to surrounding tissues. Multimodal image fusion also eliminates the need for invasive reference frames. This study analyzes the accuracy and risk factors of the ORTHBOT system in clinical use based on this design philosophy.
Future directions for RASS
RASS is expected to see broader development and application in the future. On the one hand, the rise of artificial intelligence and machine learning has led to a surge in studies focused on surgical prediction and automatic image recognition in spine surgery. AI algorithms can perform deep learning on vast preoperative and intraoperative imaging datasets, offering personalized recommendations for disease type, surgical approach, and screw sizing and trajectory, as well as real-time optimization based on anatomical and pathological variations. This approach provides more accurate and efficient decision support in patient selection, surgical planning, and postoperative recovery, reducing overtreatment and complications to achieve better clinical outcomes [30]. On the other hand, mixed reality (MR) technologies are rapidly emerging in spine and orthopedic surgery. Studies show that head-mounted augmented reality devices can achieve comparable precision to robotic systems in pedicle screw navigation [31,32,33,34,35,36,37]. During surgery, AR technology overlays digital images onto real anatomical views, allowing real-time visualization of spinal structures, blood vessels, and nerve pathways, enhancing targeting precision, reducing radiation exposure time, and alleviating surgeon fatigue [34, 38].
Importantly, the application of robotic technology in spine surgery extends beyond pedicle screw insertion. Bibliometric analysis of research trends indicates emerging focus on cortical bone trajectory screws. Robotic systems have also been used in laminectomy, spinal canal decompression, spinal tumor resection, and various endoscopic procedures to enhance precision and safety [39, 40]. Some new robotic systems have been applied in multi-level lumbar fusions, scoliosis correction, and complex spinal reconstruction surgeries [16, 41]. Others have explored their use in accurate puncture and injection during vertebroplasty [31]. Robot assistance has also shown value in endoscopic surgery. A prospective cohort study compared percutaneous endoscopic robot-assisted transforaminal lumbar interbody fusion (PE RA-TLIF) with traditional minimally invasive TLIF (MIS-TLIF) in patients with L4-5 spondylolisthesis. The study included 58 patients, with 26 undergoing PE RA-TLIF using robotic-guided screw insertion, full endoscopic decompression, and interbody fusion, while the MIS-TLIF group used conventional techniques. Results showed early postoperative advantages for the PE RA-TLIF group, such as smaller incisions, reduced blood loss, and less incision-related pain. Although this group had longer operation times, duration decreased with experience. Both groups showed no significant differences in long-term outcomes, including JOA scores, disability index, leg pain relief, and fusion rates, but the PE RA-TLIF group had better low back pain relief. The authors concluded that PE RA-TLIF enhances screw accuracy, reduces surgical trauma, and supports faster recovery, though it presents a steep learning curve and requires long-term follow-up to confirm lasting efficacy. Robotic systems also show promise in other orthopedic subspecialties. For example, in knee ligament reconstruction, smart planning of tunnel angles and depths can reduce overlap or collisions, lowering intraoperative errors and postoperative complications [42]. With continued upgrades in hardware and surgical workflow, new-generation spinal robots are expanding to broader indications. Studies have shown robotic systems to be safe and feasible for laminectomy [40], and systems like TiRobot offer superior accuracy and fewer complications in percutaneous pedicle screw placement for thoracolumbar fractures compared to conventional fluoroscopy [43]. RASS also yields satisfactory imaging and clinical outcomes in elderly osteoporotic patients undergoing cement augmentation, adolescent idiopathic scoliosis (AIS) correction, and spine trauma surgeries [19, 43,44,45]. Current research suggests no significant differences in blood loss and complication rates between RASS and traditional techniques, but robot-assisted surgery offers potential advantages in reducing surgeon fatigue, streamlining workflows, and enhancing screw or drill positioning accuracy [43]. As costs decline and surgical team training improves, RASS is expected to become more widely adopted, especially in resource-limited regions where it may enhance surgical quality and reduce error rates [45].
In addition to technical and clinical advancements, future studies should also focus on the economic implications of robotic systems. A comprehensive cost-effectiveness analysis comparing ORTHBOT with other mainstream robotic platforms (such as Mazor X, ROSA Spine, and TiRobot) would provide valuable insights into the balance between surgical efficiency, clinical outcomes, and healthcare expenditure. Such evidence would further clarify the clinical and economic utility of ORTHBOT and support its broader adoption in spine surgery practice.
Overall, the integration of advanced technology with robotic systems has created new possibilities for spine and broader orthopedic surgery. Continued expansion in procedures such as deformity correction, laminectomy, and endoscopic decompression is making surgery increasingly personalized, precise, and minimally invasive. Meanwhile, robotic and navigation technologies are extending into joint surgery. With the advancement of randomized controlled trials and multicenter studies, the next generation of RASS will become more refined, enriching its indications and safety evaluation frameworks, and playing an increasingly important role in orthopedic clinical decision-making and surgical operations.



Comments (0)