In this study, response to lomitapide treatment was assessed via the change in LDL-C levels in patients with HoFH. Patients possessed different SNPs in the MTTP gene, which our previous small study (n = 4) hypothesized would affect LDL-C reduction after lomitapide treatment, owing to the possible effect genetic variants may have on the mechanism of action of lomitapide as an inhibitor of MTP [17].
According to previous methodology [17], it could be argued that the unique variants identified in this patient cohort may be associated with the degree of response to lomitapide treatment. Of note in the present study is the rs982424 variant, which was only seen in patients with lower response (LDL-C reduction ≤ 50%). This variant does not alter amino acid sequence of the protein unlike other identified variants which affect non-coding regions of the gene and may regulate gene expression.
Interestingly, all the variants identified as potentially associated with reduction in LDL-C > 50% in our previous study were found in the present cohort and were determined to be significantly more common in the higher response group reported here. This supports the hypothesis that these variants are associated with greater response to lomitapide treatment; rs17533489 is associated with the strongest evidence for this as it is present in patients with the greatest reduction in LDL-C following lomitapide treatment. Another highlighted variant, rs745075, was found in a study of 202 statin-treated patients to be significantly associated with LDL-C lowering compared with patients without the variant (p = 0.035) [18]. Although low patient numbers in the present study potentially prevented a significant association between this variant and a high response, the findings presented here suggest that the variant may also be associated with lipid-lowering response to lomitapide.
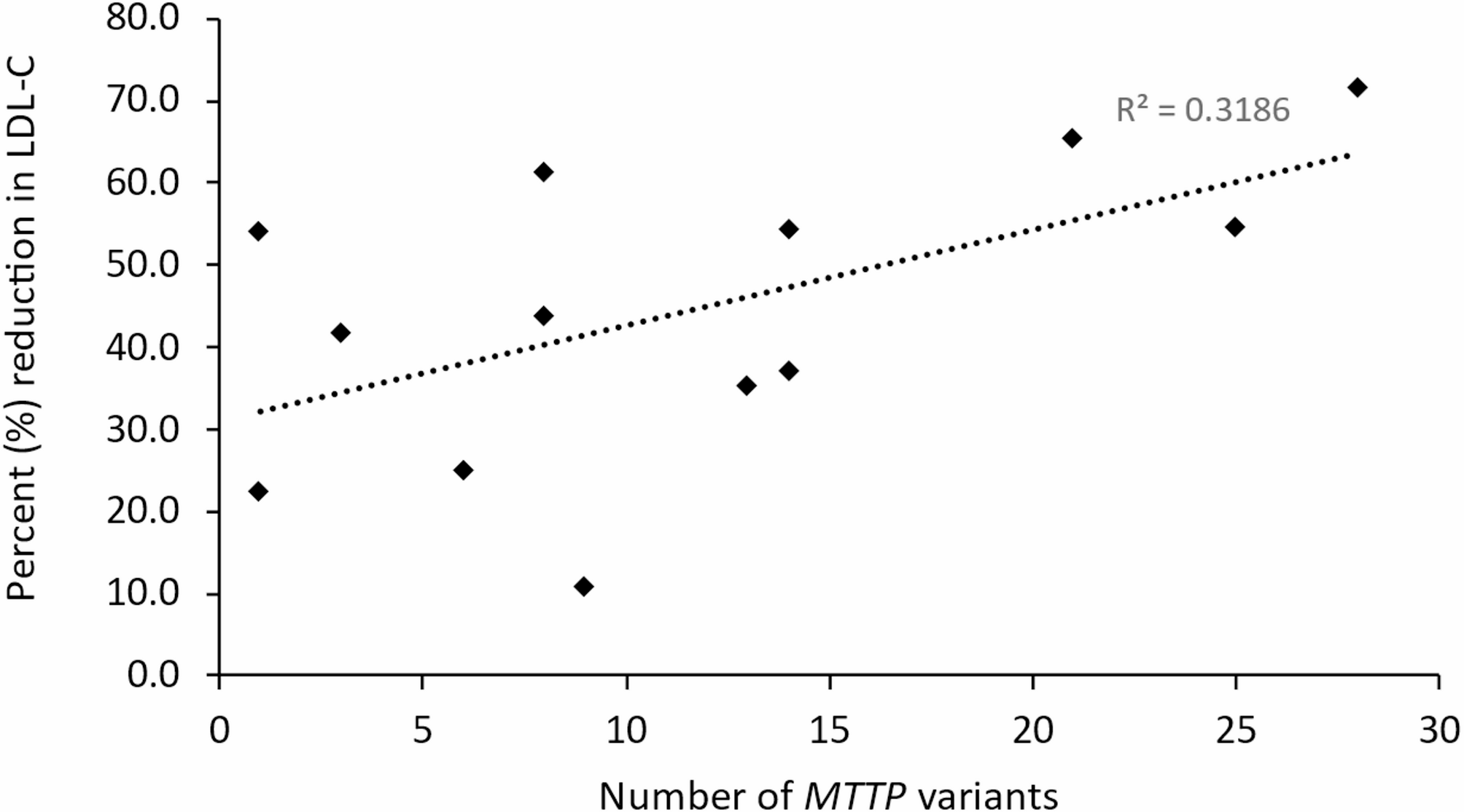
In addition to some individual variants potentially being associated with reduction in LDL-C > 50%, there was evidence that the cumulative effect of multiple minor variants could also be associated with this, as a greater number of variants were observed in the LDL-C > 50% reduction group vs. the LDL-C ≤ 50% reduction group. This is further supported by the weak/moderate positive correlation between LDL-C reduction following lomitapide treatment and the number of MTTP variants found in each patient. A possible explanation for this may be that the cumulative effect of multiple minor genetic variants within the MTP protein causes aberrant function/secretion to an extent that lomitapide binds a higher proportion of MTP protein, thereby increasing the treatment effect.
We previously highlighted rs3816873 as a variant of interest [17], suggesting that this is a variant that confers reduced structural stability of MTP and decreased binding to apoB, and possibly associated with a higher risk of CVD through the overloading of triglycerides in the myocardium [19]. In this patient cohort there was no significant difference in this variant between the LDL-C > 50% and LDL-C ≤ 50% reduction groups; rs3816873 occurred in both patient groups.
Several other variants identified in this study have been reported as being associated with lipid dysfunction. Dai et al. [20]. reported that rs2306986 was associated with non-alcoholic fatty liver disease (NAFLD) in obese children. It was concluded that the observed effect associated with this MTTP variant may alter lipid metabolism by disrupting the MTP protein function, leading to aberrant triglyceride storage in the liver. In the present study, rs2306986 was unique to the patient in LDL-C ≤ 50% reduction group with the smallest change in LDL-C levels, and this could be related to the above previously identified change in function. Furthermore, a cross-sectional study reported that rs2306986, along with rs3792683 and rs2306985, were associated with significantly lower serum triglycerides [21], with rs2306985 also associated with increased risk of NAFLD. Similar to rs2306986, rs3792683 was uniquely identified in the LDL-C ≤ 50% reduction group in the present study.
The MTTP variant rs1800804 encodes a T > C alteration in the promoter region of the MTTP gene [22]. There is prior research to suggest that deletion from the region where this variant lies may increase promoter activity by 250% [23]; however, rs1800804 has previously been reported as not affecting lipid measurements or angiographically assessed coronary stenosis [22, 24, 25] suggesting it does not lead to increased MTP expression [22]. Both rs1800804 and rs1057613 have also been shown to be associated with NAFLD risk (increased and decreased risk, respectively) [14]; however, the current study identified these variants in both patient groups, suggesting that, as with rs3816873, they do not influence how lomitapide binds with MTP and response to lomitapide treatment is unaffected. While these variants may not directly affect response to lomitapide treatment, their presence may influence subsequent hepatic steatosis status. The liver ultrasound data available for this cohort of patients with HoFH receiving lomitapide treatment indicated that the highest liver steatosis grading was 1 (mild), and there was, therefore, little evidence that particular MTTP variants are contributing to steatosis in these patients prior to initiation of lomitapide treatment. It is recommended that in the event of liver-related AEs, such as hepatic steatosis or increased aminotransferase levels, patients either reduce their dose of lomitapide or temporarily suspend treatment. Dose reduction or suspension of treatment may then lead to an increase in LDL-C levels.
Lomitapide is a small-molecule that is metabolized by CYP3A4 in the liver [26, 27]. As such, lomitapide response is likely influenced by CYP3A4 enzyme activity, which can show significant inter-patient variability and can be impacted by commonly prescribed drugs in cardiovascular disease such as diltiazem or verapamil [28]. While CYP3A4 activity with concomitant medication was not accounted for in this study, the patient with the highest response to lomitapide was also receiving a low dose of amiodarone, a weak inhibitor of CYP3A4 [29, 30]. This may suggest that the higher response to lomitapide was partially aided by the inhibition of CYP3A4 and a reduction in metabolism of the small molecule; however, no other patients were receiving any concomitant medications that may have affected the activity of CYP3A4 (Supplementary Table 1, Additional File 1) and several were able to maintain high levels of LDL-C reduction. Of note, in the previous studies, our group examined, the relationship between polymorphic enzyme P450 oxidoreductase (POR)*28 polymorphism, which is associated with increased activity of CYP3A enzymes, and the response to atorvastatin and simvastatin, in 350 hyperlipidemic patients [31]. The POR*28 allele was not associated with the lipid-lowering effect of atorvastatin and the results were replicated in an independent simvastatin-treated population. We also analyzed inter-individual variability in relation to CYP3A4 intron 6 C > T polymorphism (CYP3A4*22 allele, rs35599367) and the response to atorvastatin and simvastatin [32]; there was no association with the lipid-lowering response to both drugs [33].
Despite the variability in lomitapide response seen in the present cohort, it is encouraging that the majority of patients (8/13) showed at least a 40% reduction in LDL-C subsequent to the introduction of lomitapide. It is also encouraging that the great majority of cardiovascular events were reported prior to lomitapide initiation; however, as only two patients fell under or approached the current European Atherosclerosis Society recommended target LDL-C level of < 70 mg/dL for adults without atherosclerotic CVD risk factors and no patient achieved the < 55 mg/dL for adults with atherosclerotic CVD or major atherosclerotic CVD risk factors [2], this highlights the challenge of achieving these levels in patients with HoFH, and the need for dosage up-titration or adding another drug such as evinacumab if available. Lipoprotein apheresis is also a valuable tool for achieving recommended target LDL-C level. Lipoprotein apheresis sessions remove about 60–70% of.
LDL-C, but the LDL-C reduction is transitory and associated with a rebound elevation in lipid levels after 7–14 days. In some cases, hybrid (all available drug treatment and lipoprotein apheresis) therapy may be needed.
There were several limitations to the present study. Firstly, there are the limitations inherent to any retrospective observational study with respect to the potential for bias. In addition, the study design meant that dosage of lomitapide was not standardized, while the changes in LDL-C attributed to the introduction of lomitapide were not time-averaged but were those assessed at the last follow-up. The data are therefore a ‘snapshot’ of response to lomitapide and could have shown variability across the course of treatment. As such, and with respect to the analysis of the influence of MTTP variants, patients could have fallen on either side of the 50% reduction threshold at different points in time between commencement of lomitapide treatment and last follow-up. An alternative way of conducting the analysis would be to compare the upper and lower quartiles of response; however, this approach would require a much larger sample size, which is very difficult for a rare disease as HoFH. The current study can only be considered as an extension of our previous hypothesis-generating study [17]. Further research, such as in vitro binding studies or computational modeling is required to confirm whether particular MTTP variants indeed abrogate or enhance the effectiveness of lomitapide. Further research could also examine the extent to which genetic variation in CYP3A4 influences response to lomitapide.







Comments (0)