Consistent with the human resources policies of the SFVAHCS, nearly 100% of the HCP involved had received a primary COVID-19 vaccination series. The outbreaks we report all occurred in fairly rapid serial succession during the months of June through August 2023. Notably, there were no other outbreaks that occurred during this period and the examples did not reflect “selection” among a larger group of events. Although HCP occupational transmission might have occurred even with aggressive use of personal protection, maximal ventilation, and appropriate distancing, we did not experience other outbreaks of this magnitude absent these potential deficiencies, as noted. But we would not make the counter argument that the presence of such protective measures provides absolute assurance of successful control.
We did not perform genotyping which was difficult to obtain at our institution. This means that we cannot definitively link all of the infections through molecular biologic testing. The outbreaks, however, occurred telescoped in space and time, presumed to be due to the widely circulating COVID-19 strain in the community during the period in question.
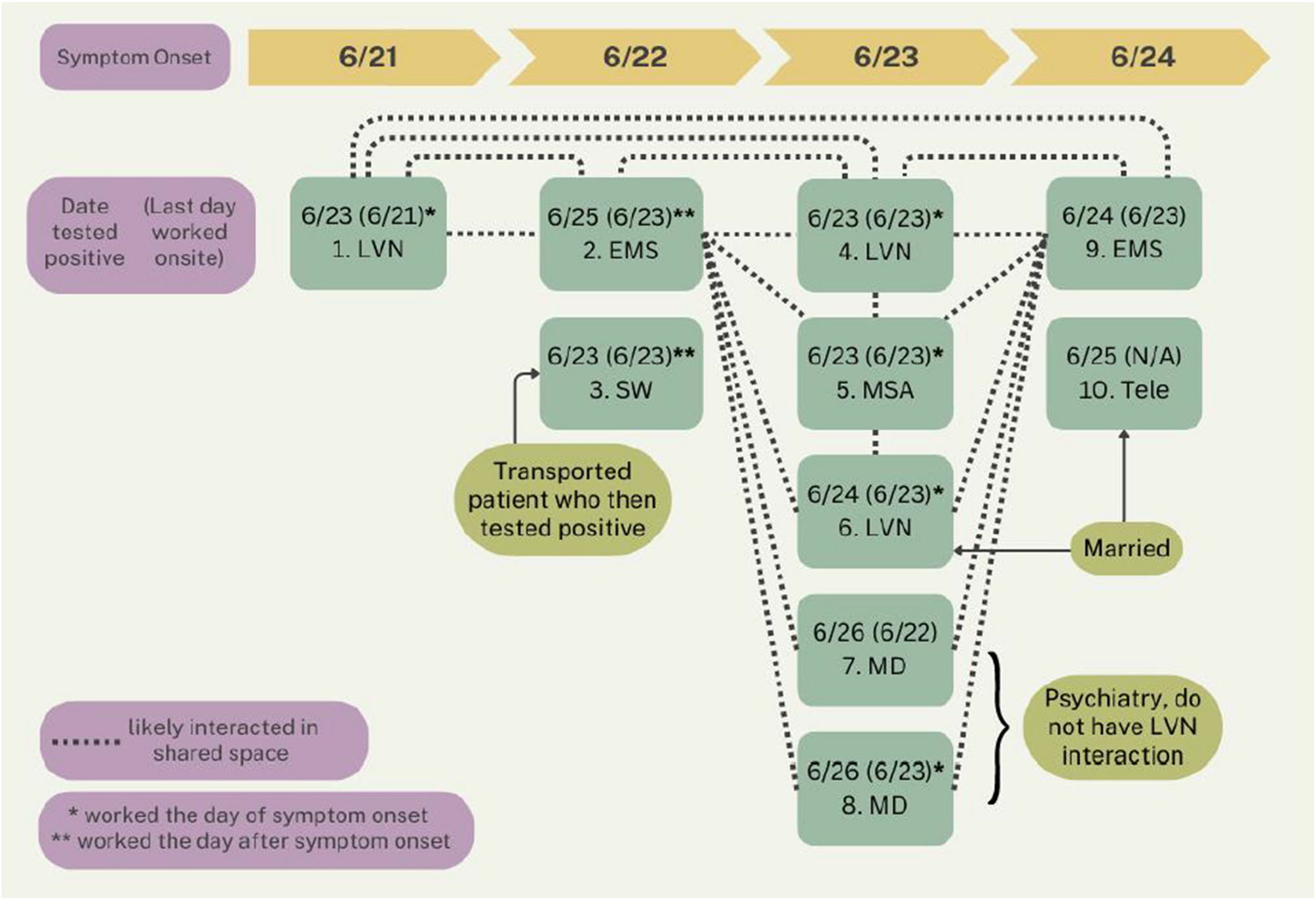
The findings of our study support the view that nursing staff can be disproportionately impacted by work-related COVID-19 among HCP consistent with their frontline roles. This has been observed by others [10, 11]. This was more pronounced in Outbreak 3, however, where 15 out of 23 affected staff members were from the nursing service, because the staff who participated in the team-building exercise that led to the outbreak were from the nursing service only. Further, while Outbreak 3 was a work-related incident due to its alignment with efforts to enhance patient care services, it is important to emphasize that the outbreak occurred in a non-occupational setting.
The overall attack rate for the three outbreaks combined was 25% (95% CI: 18–32%). Although we calculated a combined attack rate for the outbreaks in order to provide an integrated public health context, this should not be misconstrued to imply homogeneity among the three events, particularly the scenario that was work-related but transpired outside the physical workspace for the purposes of team building. The three outbreak scenarios we describe may not be generalizable to health care facilities that adopted very different approaches to COVID-19 prevention among HCP during the epidemic phase and that also may undertake alternative control strategies in future infectious disease outbreaks.
Further, we cannot exclude all alternative factors that might have contributed to the outbreaks beyond lax masking, suboptimal ventilation, failure of HCP with symptoms to quickly self-quarantine, and, in the case of the offsite team building exercise, other unaccounted for external sources of contagion. In terms of sub-optimal ventilation specifically, even if this cannot be implicated with certainty, recommend guidelines for air exchanges and maintenance of filtering systems for health care facilities should be followed rigorously, even in satellite facilities.
These HCP outbreaks shed light on lingering vulnerabilities in our defenses against occupational COVID-19 [1,2,3,4]. This offers valuable lessons for bolstering infection control practices and preventing future transmission among HCP and their patients [12]. The liberal masking practices at the outpatient clinic sites likely facilitated viral spread [13]. There was indeed a lack of uniformity in masking policy, but there also was inconsistency in complying with whatever policy was current at the time. That is, some of the staff were not masking even where it was mandated to do so. Also, staff members were coming in to work despite having symptoms (some without masking) for which work absence until negative testing was mandated, failing to call the COVID hotline for guidance as required. There were no changes in staff interactions or space sharing introduced during the outbreaks, except for rapid activation of mandatory stricter masking for all out-patient clinic staff at all times and reinforcing a standard mandate that symptomatic staff not come to work until testing negative for COVID-19. The lack of additional physical distancing between HCP could represent a missed intervention. Additionally, ventilation systems in buildings could have contributed to spread at these sites [14]. Although the building leasing agents stated that air exchanges were appropriate to standards this could not be independently confirmed. In the absence of the verified air exchanges, the potential role of ventilation in COVID-19 transmission dynamics should not be discounted. The third outbreak provided ample opportunity for person-to-person spread including very high exposure scenarios such as group car travel and shared accommodations without masking.
Take-away lessons include rapid implementation of stricter masking as early as possible when an emerging outbreak is suspected, aggressive surveillance testing early in response to an outbreak in a discrete HCP working group and reinforcing education regarding not coming to work (or work events) when symptoms suggestive of COVID-19 are present [12, 13]. Finally, building ventilation may have contributed to two of the outbreaks and always needs to be checked periodically.








Comments (0)