This was a cross-sectional study conducted in Albania during January 2025.
Study population and sampling
Study population and sampling are described in detail in Appendix 1. Briefly, the study population included 367 participants (response rate: about 90%).
Measuring instruments and data collection
A structured questionnaire was designed in SurveyMonkey to assess WRIMC stress among physicians in Albania. The questionnaire consisted of 36 items organized into three sections: [1] Demographic and professional characteristics [2], Exposure to WRIMC and associated psycho-physiological factors [3], Perceived Stress Scale (PSS-10) and two additional items regarding the overall perceived impact of work or WRIMC exposure on stress.
The demographic and professional section included 9 items, each operationalized as a variable measured as follows: age (continuous), gender (males vs. females), education level (general practitioner) vs. specialist vs. doctorate vs. postdoctoral), specialty (nominal), residence (categorical), healthcare institutions (categorical), job count (single or part-time job vs. 2 or more jobs), years of experience (continuous), employment status (employed, unemployed, retired, or other), and survey completion context (working during the day, on-call, leisure time, official leave, weekend work, medical leave, or other).
The next section of the questionnaire included 15 items, each operationalized as a variable measured as follows: phone usage frequency for work during a typical workday (never, 1–2 times/day, 3–5 times/day, 6–10 times/day, more than 10 times/day), total time spent on work-related phone use per day (less than 15 min, 15–30 min, 30–60 min, more than 1 h), frequency of receiving WRIMC during a typical workday (never, 1–3 times/day, 4–10 times/day, more than 10 times/day), frequency of receiving WRIMC outside of working hours (never, 1–2 times/day, 3–5 times/day, 6–10 times/day, more than 10 times/day), frequency of using instant messaging apps for work (never, 1–2 times/day, 3–5 times/day, 6–10 times/day, more than 10 times/day), WRIMC frequency during vacations (never, 1–2 times during vacation, 3–5 times, 6–10 times, more than 10 times), WRIMC frequency at night (after 10:00 pm) (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, always), perceived obligation to respond immediately to WRIMC (never, 1–2 times/month, 1–2 times/week, 3–5 times/week vs. always), anxiety when not responding immediately (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, always), interruptions of personal activities due to WRIMC (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, daily), mental fatigue caused by WRIMC (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, daily), irritability due to WRIMC interruptions (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, daily), WRIMC interfering with sleep quality (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, always), persistent work-related thoughts outside office hours (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, daily), and guilt for not responding to WRIMC (never, 1–2 times/month, 1–2 times/week, 3–5 times/week, always).
The third section included 10 items of the PSS-10, an internationally validated questionnaire used to measure stress levels [19], and two additional questions: perceived impact of work on stress level (PIWOSL) (not at all important vs. slightly important vs. moderately important vs. very important vs. extremely important), and perceived impact of WRIMC on stress level (not at all important vs. slightly important vs. moderately important vs. very important vs. extremely important).
The first two sections and the last two items were formulated based on literature research, particularly on techno-stress and occupational stress among healthcare professionals [10, 20,21,22,23,24,25]. Content validity was assessed through expert review by three specialists in public health and occupational medicine. A pretest was conducted with 20 physicians to assess the clarity, comprehension, and reliability of the questionnaire. Based on their feedback, minor phrasing modifications were made. The questionnaire was distributed via a SurveyMonkey-generated link through physicians’ mobile messaging applications and was self-administered.
Responses to items in the second and third sections were recoded into 4- or 5-point Likert-type scales. Internal consistency, measured by Cronbach’s alpha, was 0.916 for the second section of the instrument and 0.865 for the PSS-10. For the PSS-10, reverse scoring was applied to positively worded items (PSS-4, PSS-5, PSS-7, PSS-8) before computing reliability.
Data analysis
The PSS-10 score was calculated by reversing the required items and summing all responses, yielding a total score ranging from 0 to 40. Based on established cutoffs, stress levels were categorized as low (0–13), moderate [14,15,16,17,18,19,20,21,22,23,24,25,26], and high [19, 27,28,29,30,31,32,33,34,35,36,37,38,39,40].
Frequencies and their respective percentages were calculated for categorical variables, while means and standard deviations were calculated for continuous variables. For ordinal Likert-type items, mean values reflect central tendencies across categories, and not exact counts or durations.
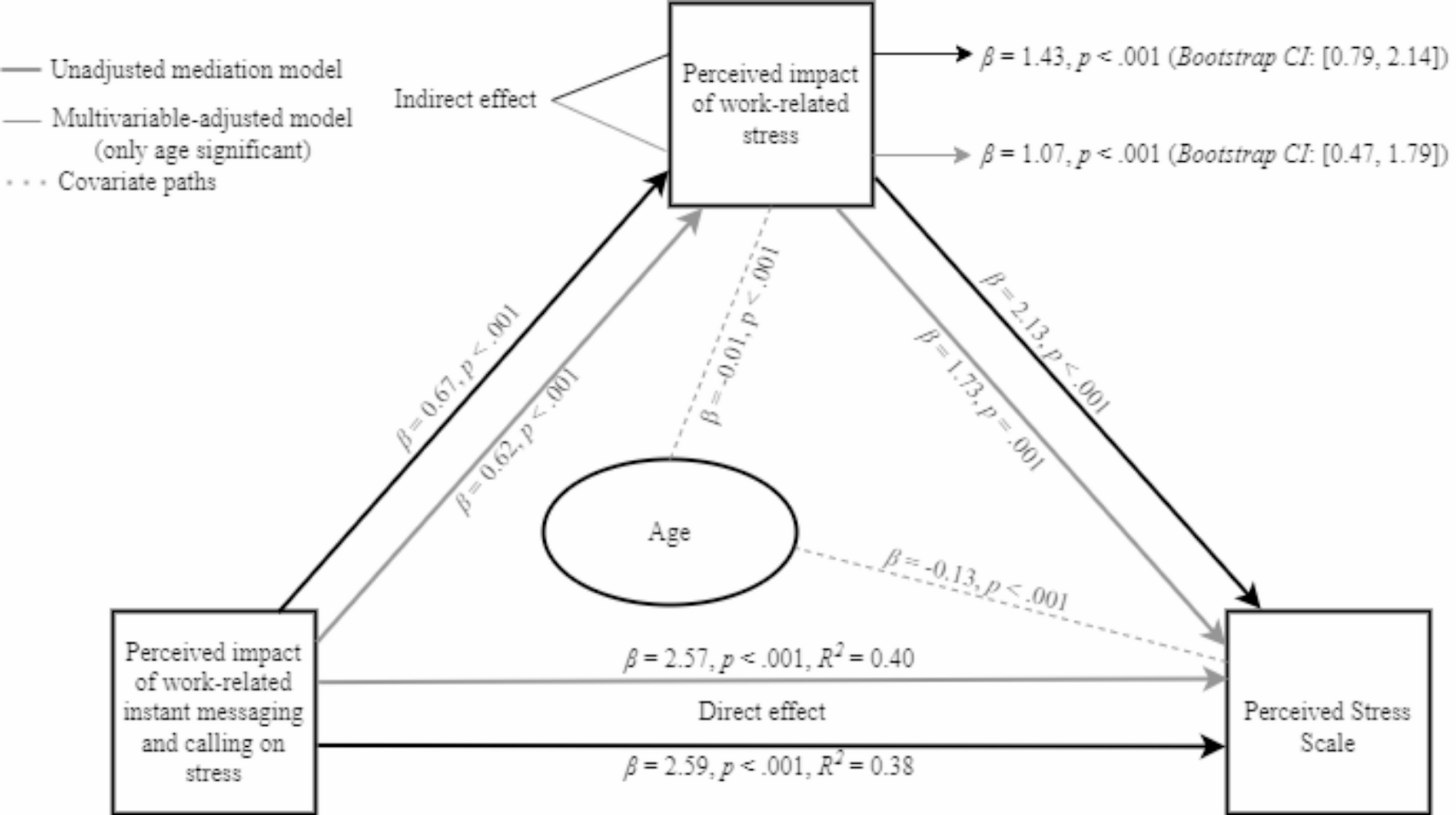
A multivariable-adjusted ordinal logistic regression model was used to assess the direct association between exposure to WRIMC, associated psycho-physiological factors, and perceived stress. A mediation analysis was conducted to examine the indirect effects of WRIMC on perceived stress with the PIWOSL as a mediator. Both crude and multivariable-adjusted models were used to test for potential confounders. Additionally, a moderation analysis was conducted to assess whether the PIWOSL influenced the strength of these associations; however, no significant moderating effect was observed. Other mediators were identified from psycho-physiological factors that showed significant associations with perceived stress in the ordinal logistic regression analysis (specifically irritability, mental fatigue, and guilt related to WRIMC). The mediation analysis included WRIMC exposure factors as independent variables and PSS as the dependent variable. Statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS) version 26, with mediation and moderation analyses performed through the PROCESS v5.0 beta2 macro by Hayes (Model 4), implemented in SPSS.
A p-value of ≤ 0.05 was considered as statistically significant.








Comments (0)