In this study, a novel approach was used to categorize orbital wall fractures (C/S/A), revealing that fractures in the S2, S3, and A1 regions had a higher likelihood of causing diplopia. Additionally, multiple fractures in the sagittal plane (S2 + S3) was associated with an increased risk of diplopia.
Our study identified preoperative diplopia development was not influenced by age (p = 0.50), etiology (p = 0.07), or gender (p = 0.91). As expected, males constituted the majority (68.4%) of our sample, with an average age of 40.4 years [15]. However, our findings slightly differed from the literature regarding the most affected age group, as nearly half of our participants (45.8%) were over forty [16, 17]. This discrepancy may be attributed to the study area’s demographics, which include a significant aging population, with over 30% of residents aged forty and above.
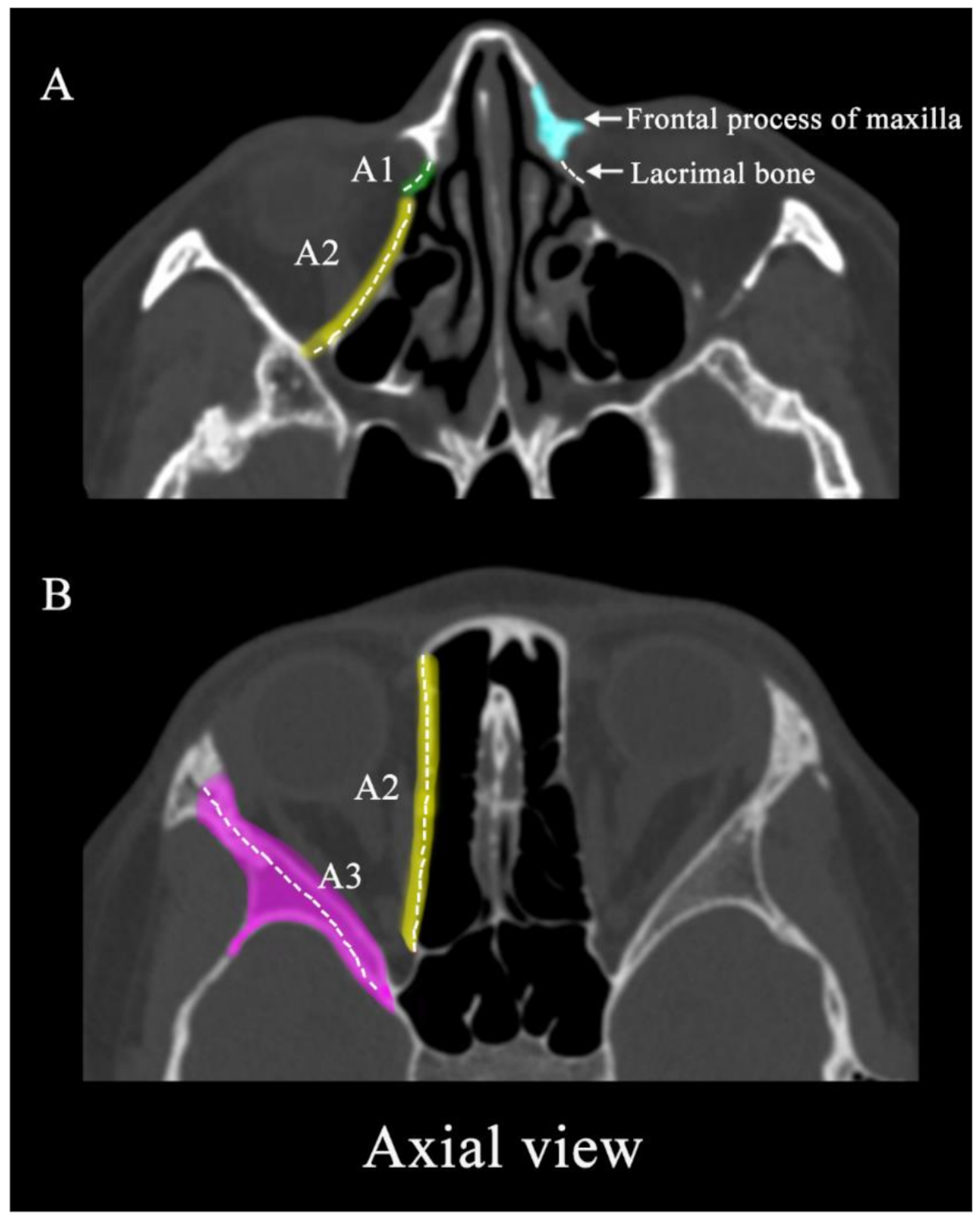
CT scanning is widely considered the definitive method for the initial radiological assessment of mid-face trauma, including orbital fractures. In our study, we artificially delineated detailed regions (C1-3, S1-3, A1-3) on sagittal, coronal, and axial CT scans. Then, we found a significant association between diplopia and specific regions, namely A1, S2, and S3, in cases of single-region fractures. Yao et al. [18] emphasized the critical importance of modified inferomedial orbital strut (mIOS), illustrating that the integrity of mIOS significantly reduces the risk of diplopia [19], which is consistent with our study. Moreover, the multifactorial analysis within this study revealed that A1 exerted the most substantial influence (exp = 2.377), further elucidating the significance of mIOS. Previous studies have also found the statistically significant relationship between elevated diplopia and fundus fractures, as well as between horizontal diplopia and medial wall fractures [20]. This may explain why these areas are more prone to diplopia. Unfortunately, we could not obtain detailed statistics on the specific directions of diplopia occurrence.
Concurrently, our study found that fractures in the S2 and S3 region of the orbital floor were significantly correlated with the occurrence of diplopia, irrespective of whether in single or multiple-region fractures, which was consistent with previous studies [20]. It is well known that the region beneath the S2 and S3 of the orbital floor corresponds to the thickest segment of the inferior rectus muscle. Mansour et al. [21] identified that the displacement of the thickest segment of the inferior rectus muscle may alter the orbital volume, potentially leading to enophthalmos. Parameswaran et al. [22] also confirmed a significant linear relationship between enophthalmos and intraorbital volume in fractures involving the internal orbit. Moreover, alterations in the orbital volume ultimately influenced the occurrence of diplopia [23]. In our study, of the 26 individuals who sustained S area fractures and subsequently experienced diplopia, 25 demonstrated damage to the inferior rectus muscle. This direct injury to the inferior rectus may be associated with the onset of diplopia, potentially resulting from edema and functional impairment of the muscle.
Our findings did not indicate a significant association between the timing of surgery and the persistence of postoperative diplopia (p = 0.36). Some studies have proposed that early intervention in patients with prominent symptoms of orbital trauma could improve postoperative visual outcomes [24]. In a prospective comparative study by El-Ghafar, early surgical intervention within three weeks of orbital floor fracture injury was associated with reduced postoperative diplopia [25]. Most orbital apex fractures can be managed conservatively [26]. Isolated infraorbital wall fractures typically do not require immediate surgical intervention unless there is entrapment of the extraocular muscles, in which case a 1 to 2-week observation period is recommended to allow edema and patient complaints to resolve. Repair may be indicated within this 2-week period under certain conditions [27]: (1) persistent diplopia, (2) ocular invagination > 2 mm, (3) incorrect eye position, (4) large orbital floor fracture (greater than 50% of the floor) or significant increase in orbital volume with a tendency towards ocular invagination. In contrast, the healing process for medial wall fractures is slower than for orbital floor fractures, extending beyond three months post-surgery and showing improvement even at six months [28]. Thus, orbital floor fractures generally achieve full recovery within three months, whereas medial wall fractures require a longer observation period without additional intervention [28].
Although this study investigates factors influencing diplopia in orbital fractures, several limitations must be acknowledged. On the one hand, as a retrospective study, it is limited in accurately capturing changes in diplopia and obtaining synchronous imaging information, precluding the analysis of potential time-related confounding factors. On the other hand, in our cohort, only one-third of orbital fracture cases were treated surgically, which may have influenced some inconsistent observations.
In summary, our findings confirm a correlation between facial orbital fractures and diplopia. We identified significant associations between diplopia and specific regions, namely A1, S2, and S3, in single-region fractures. Additionally, diplopia was notably associated with multiple-region fractures such as S2 + S3. These findings suggest that surgeons should prioritize attention to regions with a high incidence of diplopia before surgery to improve surgical outcomes and clearly communicate the potential for persistent diplopia postoperatively to manage patient expectations.









Comments (0)