Study design and setting
We conducted a cross-sectional study analysing baseline data collected from March 2023 to June 2024 for an ongoing prospective cohort study (The MeTS-HIV cohort) recruiting newly diagnosed ART naive PLWH. The cohort was assembled across four HIV high burden facilities namely the Greater Accra Regional Hospital, the Korle-Bu teaching hospital, Tema General Hospital and the Ga West Municipal Hospital who all operate out-patient ART clinics for PLWH. Further details on the cohort can be found in our previously published protocol [10]. Study participants included newly diagnosed ART naïve PLWH aged ≥ 18 years from the study sites. PLWH who were bedridden, pregnant women and individuals diagnosed with cancer and on corticoid treatment were excluded.
Sample size and sampling
The sample size was calculated using the standard sample size for estimating a proportion in a single population [n = Z2 p (1-p)/D2] with 5% margin of error and a 1.96 z-value for a 95% confidence interval (CI) [11]. Estimated prevalence of MetS among ART naïve PLWH of 23.6% from a previous Ghanaian study was utilized [7]. Additionally, we added a 15% non-response rate, and this gave a minimum sample size of 326 participants. However, since this was a baseline for an ongoing prospective study, the data for all 347 participants was analysed.
Across the four recruiting sites, newly diagnosed PLWH who were above 18 years old were enrolled consecutively into the study until the sample size was reached. Given the era of treat all policy in Ghana (All diagnosed must receive ART at diagnosis), the study utilized counsellors as trained data collectors. Recruitment into the study was done by counsellors on day of diagnosis with consenting and study questionnaire administered immediately post initial diagnosis counselling.
Data collection, anthropometric and biochemical measurements
Trained research assistants at each site interviewed consenting participants using a structured questionnaire modified from the WHO STEPS survey.
Height of participants was measured using a Seca 285 standing stadiometer on the wall at the study sites with participants standing upright to the nearest 0.1 cm. Weight was measured using a portable Seca® 763 electronic scale with participants in light clothing and bare feet to the nearest 0.5 kg. Waist circumference (WC) was measured in the mid-axillary line at the midpoint between lower margin of the last palpable rib and the top of the iliac crest at the end of normal expiration using an inelastic tape measure to the nearest 0.1 cm.
Right arm systolic and diastolic blood pressure were measured using Omron M3 comfort automatic upper arm blood pressure monitor by trained nurses and research assistants. Before measurement, participants relaxed for 5 min. Three measurements were taken ten minutes apart with participants feet on the floor and arms supported at heart level. The average of the three readings was calculated.
After an 8-hour fast by participants, 5 ml of venous blood was collected antecubital fossa for biochemical analysis. Blood samples were left undisturbed for 30 min, spun using a centrifuge and blood serum separated for storage. The frozen serum was transported from the four study sites to a central laboratory with cold chain maintained (between temperature of 2 °C and 8 °C). Analysis of high-density lipoprotein cholesterol [HDLc], low-density lipoprotein cholesterol [LDLc], total cholesterol and triglycerides was conducted on the samples at one designated central laboratory.
Data management and analysis
Data collected were downloaded in Microsoft Excel format from Kobo collect, cleaned, and imported to STATA version 17 for statistical analysis.
BMI was calculated using the standard formula of weight(kg)/height (m2) and categorized as underweight (< 18.5), healthy (18.5–24.9), overweight (25–30) and obese (> 30). WHO clinical stages were determined following the criteria from WHO. The criteria groups HIV patients according to the symptoms with asymptomatic cases classified as stage one, mildly symptomatic as stage two, moderately symptomatic and severely symptomatic as stages three and four respectively [12]. Exercise levels were categorized as none, low intensity, moderate intensity and high intensity respectively based on participants responses to the level of exercise involved in their work and leisure tasks. For alcohol consumption and smoking, previous drinkers/smokers were ever drinkers/smokers that have not consumed alcohol/smoked in the past 12 months.
Categorical variables were presented using frequencies and percentages. Median and 25th–75th percentiles were reported for continuous variables based on their distribution.
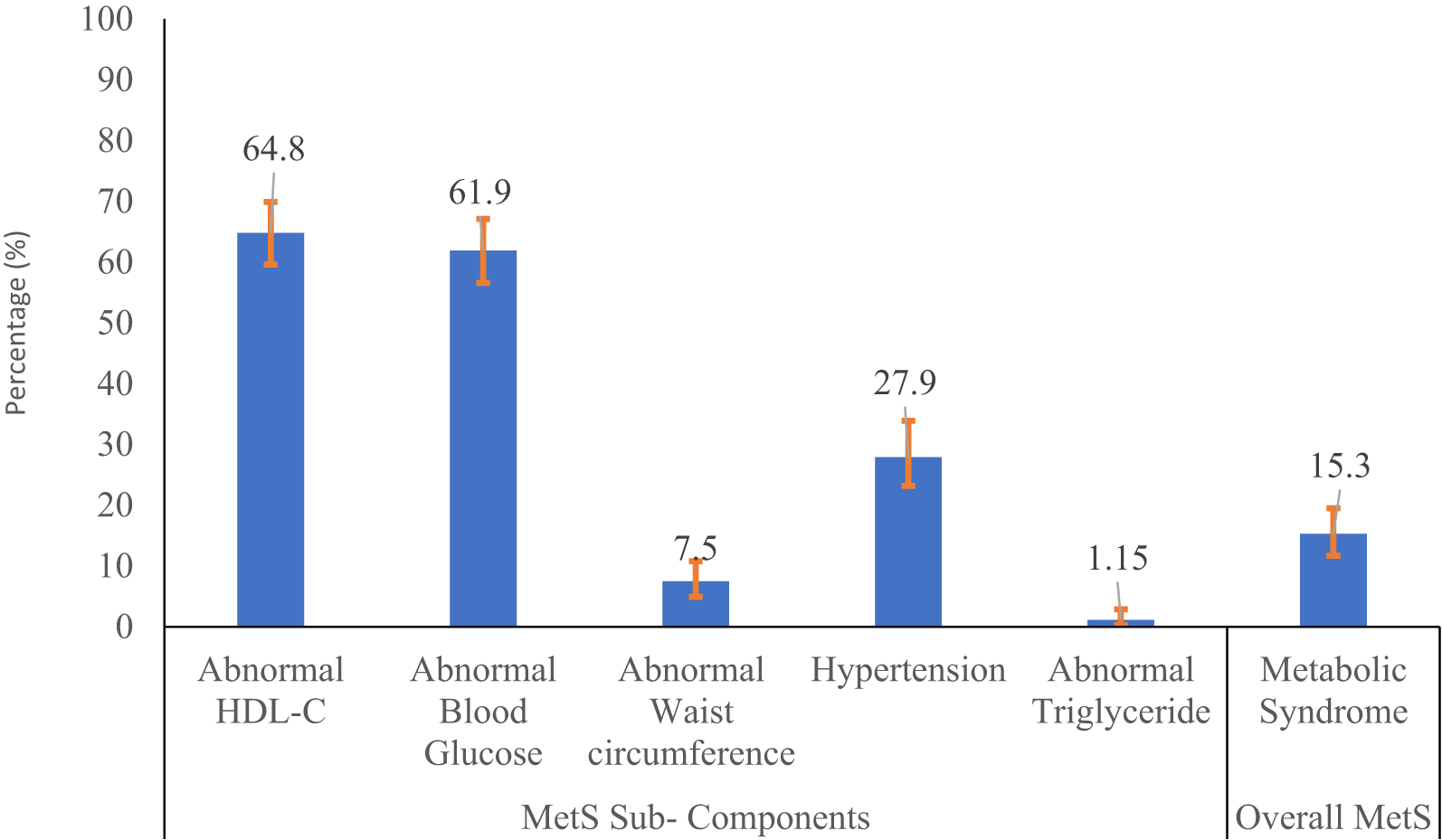
The primary outcome of Metabolic Syndrome (MetS) was defined using the Joint consensus definition that combines the International Diabetes Federation (IDF) and the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) definitions as having any three of the following [1]: (i) elevated waist circumference of > 80 cm in women and > 94 cm in men (adjusted for the African population), (ii) Triglycerides 150 mg/dl (3.88mmol/l) or greater or on treatment for dyslipidemia, (iii) HDLc < 40 mg/dl (1.03 mmol/l) in men and < 50 mg/dl (1.29 mmol/l) in women or on treatment for dyslipidemia, (iv) BP 130/85 mmHg or greater or on treatment for hypertension, (v) fasting glucose 100 mg/dl (5.6 mmol/l) or greater or on treatment for diabetes [1].
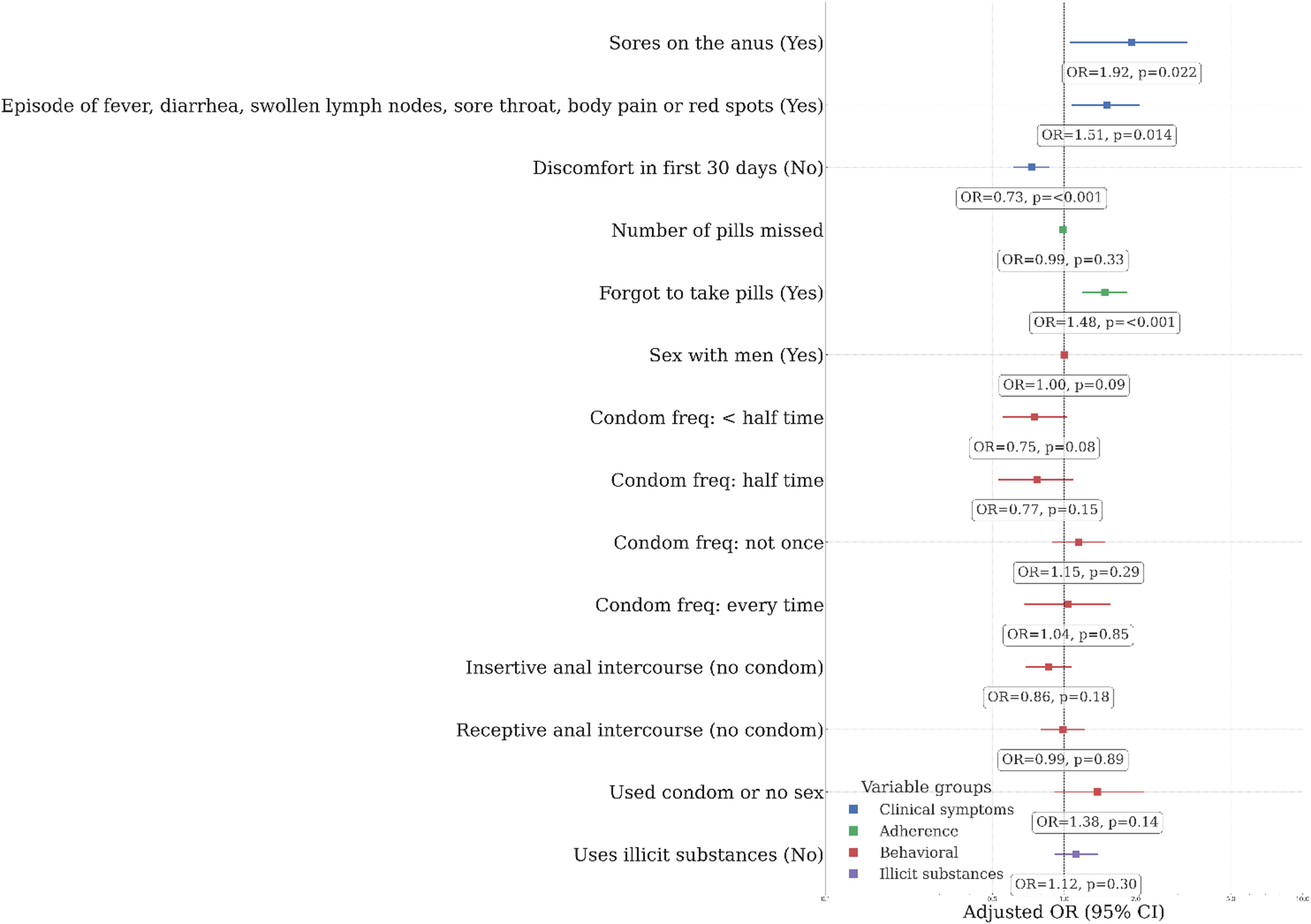
Prevalence of MetS was calculated as the number of participants with three or more MetS components divided by the total number of participants screened. To determine factors associated with prevalence of MetS among ART naïve PLWH, logistic regression was conducted to model the log-odds of MetS.
Unadjusted odds ratios (ORs) and adjusted odds ratios (aORs) with surrounding 95% Confidence Intervals (95%CI) were used to summarize strengths of associations of interest. Variables with significance (p value < 0.05) at bivariate level were fitted into the multivariable logistic model. We used both the magnitude of the effect size (OR ≥ 1.5) and coverage of 95% CI (including the majority of effect sizes in one direction) to report on clinically and statistically meaningful findings.







Comments (0)