Among CALHIV, the overall rate of viral suppression was 91.6%. Multivariable regression modelling revealed several factors significantly associated with viral suppression. This included age, WHO Clinical stage, prior DTG status, duration on ART, being on MMD, malnutrition status, retention and geographical zones. Specifically, older adolescents (15–19 years), WHO stage I and II, being on MMD were more likely to achieve viral suppression. Contrarily, regional disparities in viral suppression rates were observed, suggesting possible differences in program implementation or healthcare access.
We found a high (91.6%) proportion of viral suppression among CALHIV on a DTG-based regimen. Furthermore, 66.2% of previously unsuppressed became suppressed and 88.5% of previously suppressed remained suppressed. The proportion of HIV viral suppression on a DTG-based regimen CALHIV in our study is approximately similar to 91.5% and 92% as reported in Nigeria [7] and Ethiopia [5]. However, it was a bit higher compared to 84.0% and 80.0% which were reported in the USA [8] and Kenya [9]. These variations could be explained by the patient management and guidelines in viral load measurements.
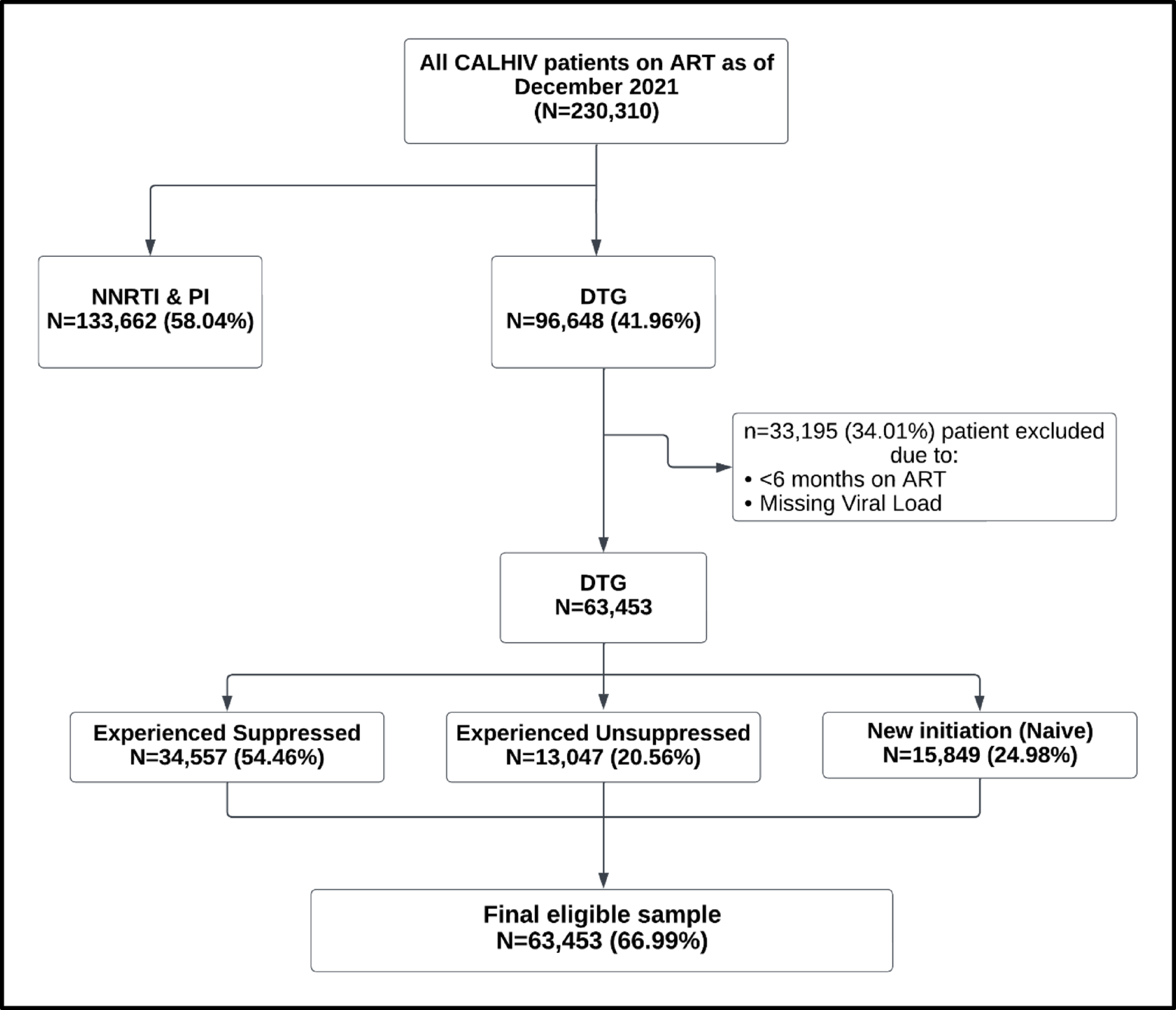
Among previously unsuppressed CALHIV at baseline, 66.1% achieved viral suppression after shifting to a DTG-based regimen and among previously suppressed CALHIV at baseline, 88.4% remained suppressed. The proportion is approximately similar to studies in Italy, Ireland, and Nigeria [6,7,8,9,10,11,12]. Among ART-naïve participants on a DTG-based regimen, viral suppression of 91.7% after six months. The proportion is relatively similar to studies in Uganda and France [9, 10]. In addition, ART naïve participants had a higher proportion of viral suppression (93.2%) compared to ART experienced who shifted to a DTG-based regimen with 91.4%. The findings are similar to studies in western India [15], Nigeria [11], and Uganda [13]. It showed a good response to the DTG-based regimen, which may reduce the risk of developing viral resistance [16].
This study found several factors independently associated with viral suppression including duration on ART of more than 24 months.
Similar findings have been reported elsewhere in the USA [17], France [14], and Kenya [9]. It can be explained by the evidence from clinical practice, which suggests that prolonged ART can reduce viral load below the limit of detection for a long-term period [5].
We also found ‘Ever received a multi-month prescription (MMP)’ to be significantly related to viral suppression compared to participants who never received a multi-month prescription. Participants who have ever received multi-month prescriptions are 1.25 times more likely to achieve viral suppression compared to those who never received multi-month prescriptions, which is consistent with the findings of studies conducted in Ethiopia [18] and Kenya [19]. It may be the case that those who do not receive this multi-month prescription for viral suppression have poor adherence due to a drop in drug concentration in body fluids because their viral load increases because of their inability to suppress HIV replication, which in turn causes their viral load to increase.
In this study, at baseline, we also found the age of children and adolescents living with HIV to have a significant effect on viral suppression. Children and adolescents living with HIV aged 5–14 years were less likely to achieve viral suppression compared to children and adolescents living with HIV aged 1–4 years. The results are consistent with reports from the USA [20] and Zimbabwe [21]. This can be explained by the fact that adolescents and young adults living with HIV experience multiple barriers to adherence, including developmental, physical, emotional, behavioural, and social dynamic changes.
Furthermore, in this study, those not retained in care were less likely to achieve viral suppression compared to CALHIV retained in care, which mirrors the findings of the study done in South Africa [22]. This indicates that CALHIV being retained in care were more likely to achieve viral suppression compared to those not retained in regular care since adolescents seem to have lower retention rates compared to other age groups due to psychosocial and emotional challenges which are led by stigma and discrimination, peer pressure and identity development, and mental health issues.
This study utilized the nationally representative data of children and adolescents living with HIV. Hence, enough statistical power increases the precision of the estimates and makes the findings generalizable to treatment naïve and experienced CALHIV. This is the first study in Tanzania to evaluate the HIV viral suppression on a dolutegravir-based regimen and associated factors among CALHIV. Therefore, our study has provided a basis for the estimation of viral suppression amongst CALHIV on a DTG-based regimen in Tanzania.
This study has several limitations related to its retrospective nature which utilized secondary data, which might threated data quality issues which includes missing values in viral load and explanatory variables. Additionally, unmeasured confounding variables, such as underlying health status, partner behaviors, or provider-level factors could not be assessed. The inability to conduct drug resistance testing and antiretroviral drug level testing, which could have helped to determine the contributions of resistance before switching to DTG to the risk of treatment failure, especially among virally unsuppressed CALHIV on ART.







Comments (0)