
Remember me
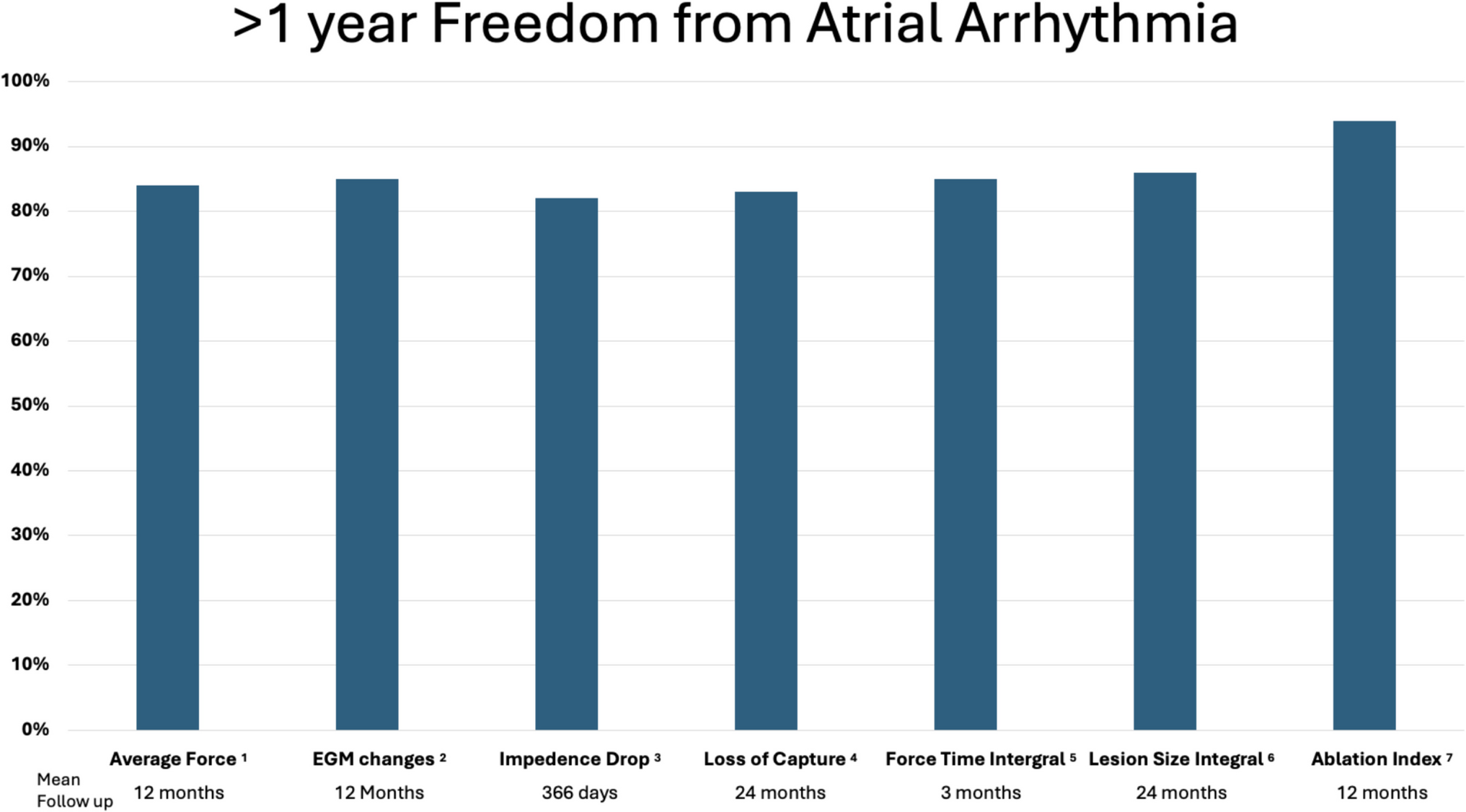

Pulmonary vein isolation (PVI) has emerged as the foundational strategy for rhythm control in symptomatic atrial fibrillation (AF) patients. Central to the efficacy of catheter ablation is the creation of durable, transmural lesions. Incomplete or non-transmural lesions are associated with pulmonary vein reconnection and arrhythmia recurrence. As our understanding of lesion biophysics has matured, so too has the array of tools available to guide and assess lesion formation. Among the earliest advancements was the incorporation of contact force (CF) sensing [1]. Contact force alone does not capture the biophysical elements lesion quality. Other markers of lesion formation include termination of unipolar negativity of electrogram (EGM) [2], a drop in local impedance of ≥ 10 ohms [3], and loss of local capture [4]. Composite indices including force–time integral (FTI) [5], lesion size index (LSI) [6], and ablation index (AI) [7] —which integrates CF, time, and power into a single, real-time metric have led to modest improvement in arrhythmia-free survival following AF ablation (Fig. 1).
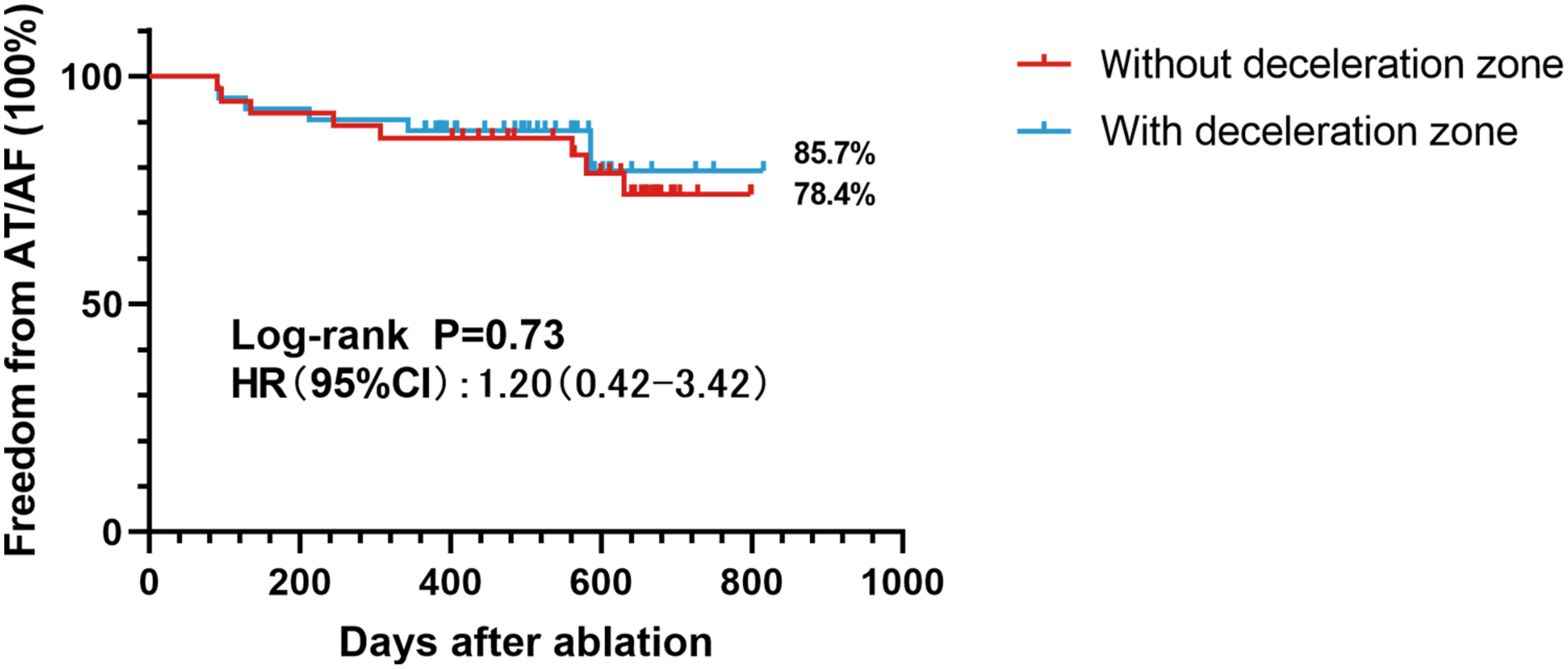
Fig. 1
Freedom from atrial arrhythmia during radiofrequency atrial fibrillation ablation using various measurements
Lesion formation during radiofrequency (RF) ablation involves the interplay of resistive and conductive heating at the catheter–tissue interface. While histologic validation remains the gold standard for assessing “transmurality” and lesion completeness, it is not feasible in vivo. In the absence of direct tissue characterization, surrogate measures are needed to evaluate lesion formation during and after ablation. One such surrogate is high-sensitivity troponin I (hs-TnI), a well-established biomarker of myocardial injury. Troponin release following RF ablation correlates with the extent of cardiac myocyte necrosis and has been shown to reflect the volume and depth of tissue injury. Prior studies have demonstrated that lower post-procedural troponin levels are associated with incomplete lesions and higher rates of pulmonary vein reconnection, underscoring its potential utility as an indirect indicator of lesion quality. Although it cannot localize gaps or provide real-time procedural feedback, troponin measurement offers a simple, scalable method to compare the biological effect of different ablation strategies on myocardial tissue.
In this issue of the Journal of Interventional Cardiac Electrophysiology, Yano and colleagues present a compelling retrospective analysis comparing the degree of myocardial injury and systemic inflammation between AI-guided and conventional CF-guided AF ablation [8]. Drawing from a single-center registry of 794 patients, they examined procedural characteristics, biomarker responses, and pulmonary vein reconnection rates in patients undergoing PVI with CF guidance (n = 241) versus AI guidance (n = 553). One of the most striking findings was that, despite shorter ablation times and fewer lesions delivered, patients in the AI group demonstrated significantly higher post-procedural hs-TnI levels. This suggests that AI guidance enabled the creation of deeper, more effective lesions with greater myocardial impact, despite reduced RF time—underscoring lesion quality over quantity.
Yano et al. found no significant differences between the AI and CF groups in systemic inflammatory markers such as white blood cell count, neutrophil-to-lymphocyte ratio (NLR), and C-reactive protein (CRP). This is a reassuring observation, indicating that the increased myocardial injury associated with AI-guided ablation did not translate into heightened systemic inflammation or a disproportionate physiological response. The study also showed that pulmonary vein reconnection was less frequent among patients who underwent AI-guided ablation—an observation aligned with prior studies suggesting superior lesion durability with this approach. Taken together, these findings support the conclusion that AI-guided ablation may provide more efficient and durable lesion formation, with a safety profile similar to or better than conventional CF-guided ablation.
While clinical endpoints such as arrhythmia recurrence remain the ultimate measure of success, biomarkers offer real-time insights into the physiological effects of ablation. Elevated troponin levels, while not specific to lesion efficacy, are known to correlate with the volume of myocardial necrosis. Previous studies have shown that patients with lower troponin levels post-ablation are more likely to experience pulmonary vein reconnection, reinforcing the idea that troponin may serve as a surrogate marker for lesion completeness. The observation by Yano et al. that AI-guided ablation produced significantly higher hs-TnI levels, even after adjusting for lesion number and RF time, provides mechanistic support for the clinical advantage of AI.
Nevertheless, The study has limitations. As a retrospective, observational analysis, it is subject to potential confounding by factors such as procedural era and operator experience. The CF-guided procedures were performed earlier in the study period, and improvements in technique, adjunctive imaging, or catheter technology may have contributed to some of the observed differences. Additionally, the study did not include baseline hs-TnI values, which limits interpretation of absolute changes in myocardial injury. Pulmonary vein reconnection data were only available for patients who returned for repeat ablation, introducing the potential for selection bias. Moreover, the findings, while internally consistent, reflect the practices and protocols of a single institution and may not be generalizable across centers with different technologies or operator expertise.
The findings presented by Yano and colleagues are consistent with and complementary to the broader body of literature validating AI-guided ablation. Meta-analyses and prospective cohort studies have demonstrated that AI-guided lesion formation is associated with higher rates of durable PVI, reduced ablation times, and improved arrhythmia-free survival. The integration of lesion metrics into ablation workflows represents an important evolution in procedural standardization and personalization. Importantly, the use of AI also facilitates more reproducible outcomes across operators and institutions, a key goal as ablation becomes more widely available to patients with paroxysmal and persistent AF.
This study by Yano et al. adds valuable data to the growing evidence base supporting AI-guided ablation for AF. By demonstrating that AI enables the delivery of more impactful lesions with comparable safety and improved long-term lesion durability, it advances the field. Future prospective, randomized studies are warranted to confirm these findings and to explore how lesion metrics can be integrated with advanced imaging and real-time tissue assessment to further enhance procedural efficacy. For now, their work affirms a central message: optimizing lesion quality—not simply achieving isolation—is the key to durable success in AF ablation.
Comments (0)