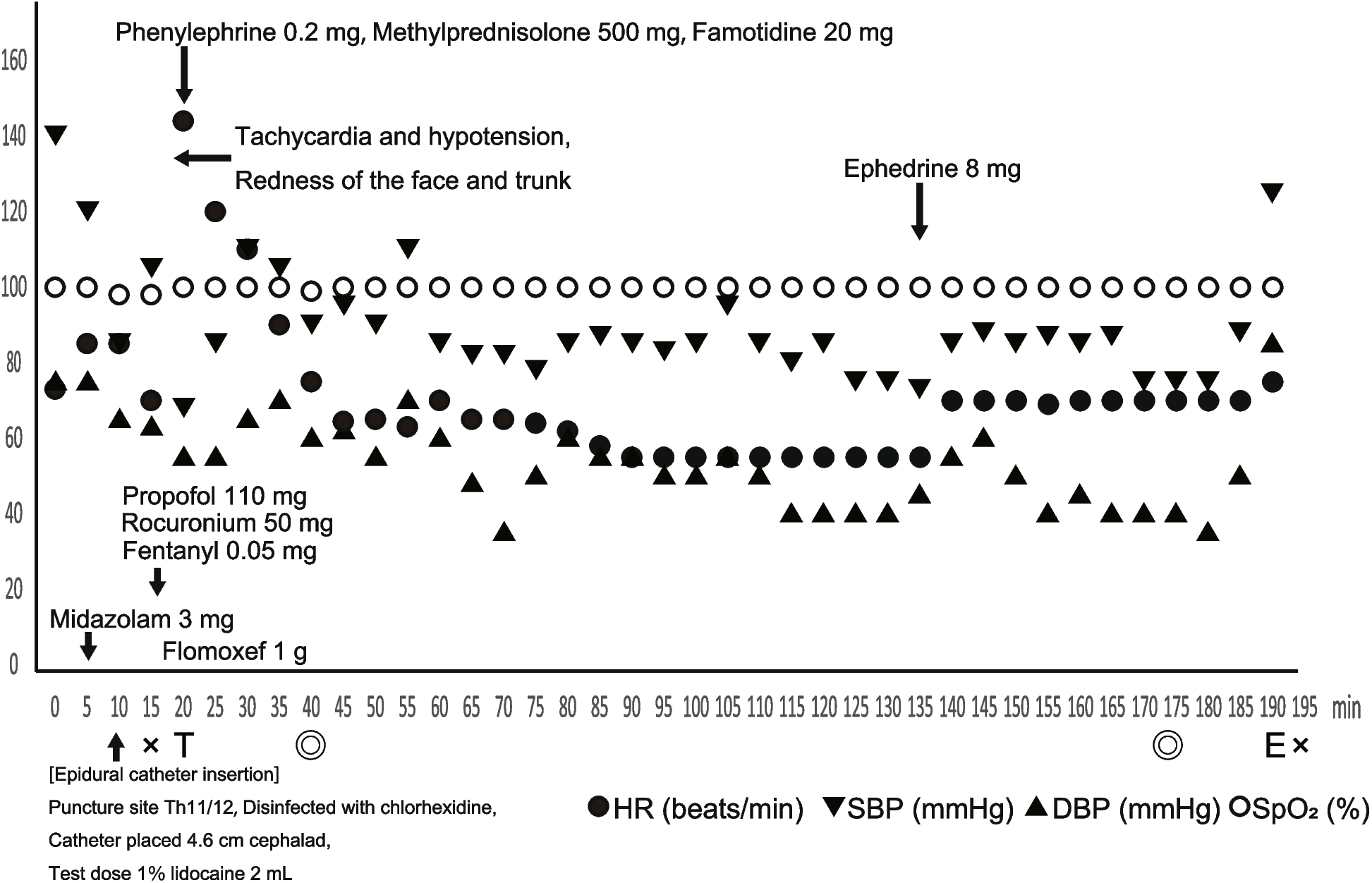
In the present case, anaphylaxis occurred after the induction of general anesthesia, and the causative agent was midazolam administered during epidural anesthesia before the induction of general anesthesia.
Perioperative anaphylaxis is often different from non-perioperative anaphylaxis, and there are many differential diagnoses [6]. Diagnosing perioperative anaphylaxis requires a combination of several methods in addition to the diagnostic criteria given by the World Allergy Organization (WAO) [7]. In the present case, the clinical score [1] was used to diagnose perioperative anaphylaxis.
The clinical score is based on the sum of the scores of the following five items: cardiovascular symptoms, respiratory symptoms, skin symptoms, combination of symptoms, and time from administering the suspected drug to the appearance of symptoms. Because the clinical score for this case was 14 points in total, likely to be an immediate hypersensitivity reaction [1], perioperative anaphylaxis was suspected. However, perioperative anaphylaxis could not be diagnosed based on the clinical score alone. Therefore, histamine, tryptase, and skin test results were used to diagnose perioperative anaphylaxis.
There are currently several diagnostic thresholds of tryptase for perioperative anaphylaxis. Recently, the tryptase threshold specified by the European Academy of Allergy and Clinical Immunology (EAACI), calculated as 1.2 × baseline tryptase + 2 µg·L−1 [3], has shown high accuracy [8, 9]. Furthermore, the histamine threshold for perioperative anaphylaxis also has high accuracy [2]. In the present case, both tryptase and histamine levels were above the thresholds.
Skin testing is essential to diagnose perioperative anaphylaxis and identify the causative agent. According to the JSA guideline, all agents used before the onset of anaphylaxis should be tested [6]. Generally, rocuronium and antibiotics, usually used during general anesthesia induction, are the common causative agents of perioperative anaphylaxis [6, 10,11,12]. In addition, chlorhexidine, the antiseptic used most often in the perioperative period, has been reported as the third most common cause of perioperative anaphylaxis in a recent large-scale study conducted in the 6th National Audit Project (NAP6) [11]. However, midazolam, which was used before the induction of general anesthesia, was the causative agent of perioperative anaphylaxis in the present case. The present case showed that the causative agent of perioperative anaphylaxis should not be identified only by the timing of the onset of anaphylaxis.
However, other agents used in the skin tests may have shown false-negative results. Therefore, duplicate skin tests could have been done to confirm the diagnosis.
Skin testing should be administered within the maximum concentrations indicated in the guidelines to avoid false-positive results [6]. The maximum concentration of midazolam (intradermal test) was 500 μg·mL−1 in the 2011 guideline in France and the 2021 guideline by the JSA for perioperative anaphylaxis [5, 6], whereas a concentration of 50 μg·mL−1 is recommended in the 2019 guideline for perioperative anaphylaxis [3]. Although the intradermal test was positive for midazolam at both 50 and 500 μg·mL−1 in the present case, anesthesiologists should be aware of the concentrations of suspected agents for skin testing. In addition, skin testing carries a risk of triggering anaphylaxis [6]. In the present case, midazolam 50 μg·mL−1 was positive on the intradermal test. Therefore, we did not have to test midazolam 500 μg·mL−1 to avoid the recurrence of anaphylaxis that may occur during the test. Furthermore, the intradermal test result of 500 µg·mL−1 midazolam might cause a false-positive result.
In addition, the composite score specified by JESPA [13] was used for diagnosis. The composite score is determined by summing the scores of three items: (1) clinical score, (2) tryptase level, and (3) skin test and basophil activation test results. A score of 2 or more indicates perioperative anaphylaxis. The composite score for the present case was 3 points, indicating perioperative anaphylaxis. The composite score may be helpful when perioperative anaphylaxis is difficult to diagnose with a clinical score of 21 or less, as in the present case.
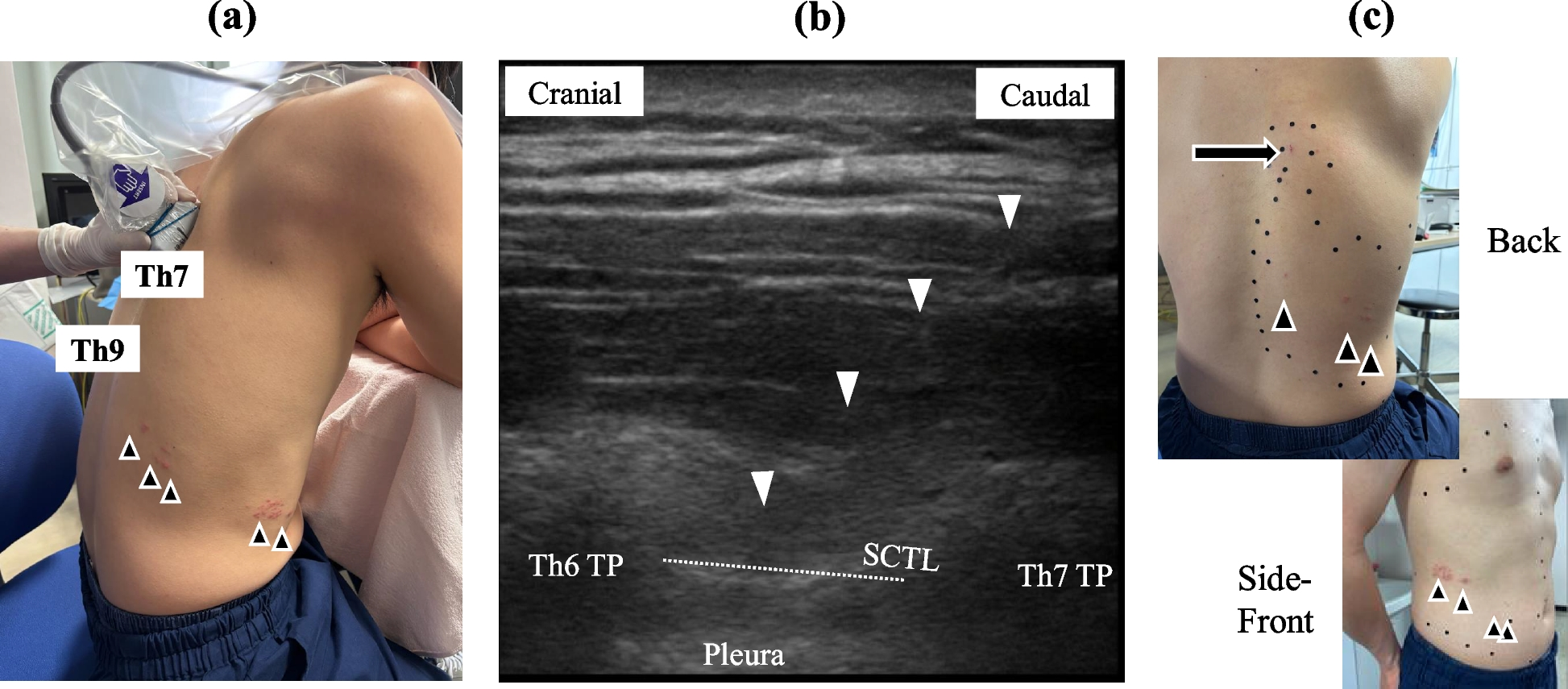
In the present case, the timing from midazolam administration to the onset of anaphylaxis was 17 min. The median time to the onset of symptoms of anaphylaxis caused by midazolam is 2 min [14]. Regarding the clinical score, shorter intervals between administration of the suspected agent and symptom onset are associated with higher scores. Specifically, 5 and 15 min are the criteria for the time from administering the causative agent intravenously to the onset of anaphylaxis [1]. This is particularly relevant for intravenous drugs, since the rapid onset of symptoms is considered to support the likelihood of causality. In the present case, midazolam was administered intravenously before inserting the epidural catheter, and the patient was sedated during the epidural catheter insertion. Therefore, midazolam was unlikely to remain in the intravenous drip route until the onset of anaphylaxis.
Several reports have shown that anaphylaxis does not develop immediately after midazolam administration. The time from administering midazolam intramuscularly to the onset of anaphylaxis was 30 min [15]. The time from administering midazolam intranasally to the onset of anaphylaxis was 11 min [16]. The onset of anaphylaxis caused by non-intravenous causative agents might be delayed.
However, there is a case in which the time from administering midazolam to the onset of anaphylaxis was 42 min [14]. Although the cause of this is unclear, several cases showed that anaphylaxis does not always develop immediately after administering the causative agent; further studies might show their epidemiological and other characteristics.
This report had several limitations. First, substances such as remimazolam were not tested in the skin test, which has been reported to exhibit cross-reactivity with midazolam [17]. Since the present patient might have examinations under sedation in the future, a search for alternative medications should be conducted. We would like to perform further tests if the patient wishes to test for cross-reactivity with other benzodiazepines.
Second, decimal values were not noted in the skin tests. Although we believe the skin test results were reliable, we will record the decimal values in future studies.
Third, adrenaline was not administered in this case. The first-line treatment for anaphylaxis is adrenaline [6], which should be administered early once symptoms of anaphylaxis have been recognized or suspected [18]. Thus, we should treat future anaphylaxis cases with adrenaline as soon as possible.
A case of perioperative anaphylaxis caused by midazolam, which was used before the induction of general anesthesia, was described. A definitive diagnosis of midazolam-induced anaphylaxis was supported by a non-low clinical score, positive findings on skin testing and serological evaluations, and a high score on the recently proposed composite scoring system.


Comments (0)