The use of neuromuscular blocking agents should be avoided in MG patients whenever possible, as they exhibit marked sensitivity to these agents, often resulting in unpredictable or prolonged neuromuscular blockade [3]. However, neuromuscular blocking agents are known to improve surgical conditions not only during laparoscopic surgery, but also during thoracoscopic surgery [4]. Moreover, robotic surgery, in particular, requires secure immobilization of the patient to ensure safety, as accessing the patient becomes difficult once the robot is docked with the patient, and movement by the patient can lead to iatrogenic injury. In the present case, therefore, we planned to use rocuronium with utmost caution under strict neuromuscular monitoring, and to reverse the rocuronium-induced neuromuscular blockade with sugammadex at the end of surgery.
Although the current guidelines for neuromuscular monitoring do not specifically address the preferred neuromuscular monitoring method, whether acceleromyography or electromyography [5, 6], it has been demonstrated that electromyographic neuromuscular monitoring is less variable than acceleromyography and is similar to mechanomyography [7], which is considered the “gold standard” method of neuromuscular monitoring [8]. Additionally, the ability to obtain reliable measurements even when the arms and hands are tucked and access to patients is limited due to surgical positioning is one of the advantages of electromyography. Therefore, electromyography is considered suitable for neuromuscular monitoring during robotic surgery. However, to the best of our knowledge, no studies comparing acceleromyography and electromyography in patients with MG have been reported. In this case, the patient’s position during surgery did not interfere with the setup of acceleromyography. Although electromyography was also used, acceleromyography was chosen for neuromuscular management due to the wealth of our own clinical experience with this device [9].
When using acceleromyography, normalization (dividing the measured TOF ratio by the baseline value) is generally recommended, as the baseline TOF ratio obtained with acceleromyography is often greater than 1.0 [5, 10]. This requires neuromuscular monitoring at the beginning of general anesthesia induction, although it can complicate the process of induction. On the other hand, electromyography does not require normalization, which is another of its advantages. However, even when using electromyography, neuromuscular monitoring at the induction of general anesthesia is still essential in patients with MG, because the dose of neuromuscular blocking agents should be carefully titrated under neuromuscular monitoring.
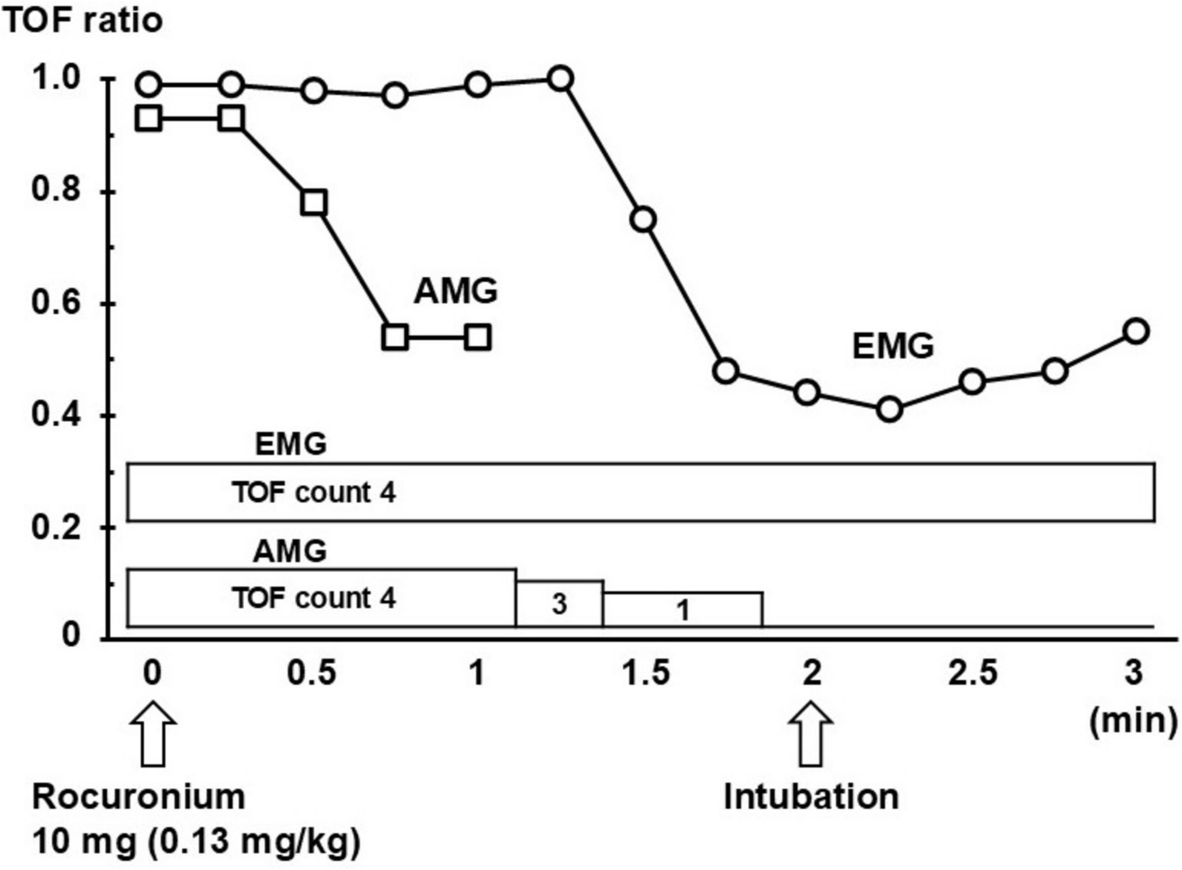
A decreased baseline TOF ratio, defined as less than 1.0 with acceleromyography at AP muscle and less than 0.9 with electromyography at hypothenar muscles (i.e., the ADM, flexor digiti minimi brevis, and opponens digiti minimi), has been reported as a determinant of an increased response to neuromuscular blocking agents [9, 11]. In the present case, the acceleromyographic baseline TOF ratio was decreased and an increased response to rocuronium was observed at the induction of general anesthesia, as seen by the fact that a much smaller-than-usual dose resulted in complete neuromuscular blockade. In contrast, neither a decreased baseline TOF ratio nor an increased response was observed with electromyographic monitoring at the ADM muscle. Our case report suggests that recognition of the potential for such a discordance between monitoring methods is important.
An investigation of ipsilateral and simultaneous comparisons of TOF responses at the AP muscle using acceleromyography and electromyography in a general surgical population has shown that acceleromyography is more sensitive in detecting early neuromuscular recovery [12]. It has also been reported that the TOF response measured by acceleromyography at the AP muscle is greater and recovers more rapidly than that measured by electromyography at the first dorsal interosseus muscle [13]. Similarly, when acceleromyographic TOF responses at the AP muscle are compared with electromyographic TOF responses at the ADM muscle, the former are generally reported to recover more rapidly [14]. Contrary to these previous reports, however, the earlier recovery of the electromyographic TOF responses was observed in the present case. Had neuromuscular management been based solely on electromyography, the amount of rocuronium administered in the present case would likely have increased, potentially resulting in increased morbidity and the need for postoperative mechanical ventilation [15].
Sugammadex, administered at appropriate doses based on neuromuscular monitoring, similar to those in patients without MG, has been reported to be effective for reversal of rocuronium-induced neuromuscular blockade even in patients with MG [16, 17]. However, the recommended dose of sugammadex (2 mg/kg at a TOF count of 2) is based on studies using acceleromyography [18,19,20], and the appropriate dose of sugammadex based on electromyography is uncertain. Furthermore, in the present case, the acceleromyographic TOF count recovered to 2 later than recovery of the electromyographic TOF count to 2. Therefore, 2 mg/kg of sugammadex would have been insufficient if its administration was guided only by an electromyographic TOF count of 2. Thus, we recommend using electromyography in combination with acceleromyography when using sugammadex in MG patients, at least until further evidence clarifying the difference in neuromuscular recovery of myasthenic patients as measured by acceleromyography and electromyography becomes available.
While the AP muscle is usually used for acceleromyographic neuromuscular monitoring, not only the AP but also the ADM and other muscles are used for electromyographic neuromuscular monitoring. Since different muscles may be affected in each patient with MG [21], the results of neuromuscular assessment can vary depending on the monitoring methods used. This may be one of the possible explanations for the discordance in responses to neuromuscular blockade between monitoring methods and the contradictory finding regarding neuromuscular recovery in the present case, which contrasts with previous reports.
Additionally, in MG, the difference in the electrical current used for supramaximal stimulation between acceleromyography and electromyography may also influence the results of neuromuscular assessment. Acceleromyography has been reported to require a higher electrical current than electromyography to obtain adequate twitch responses for the acceleration transducer in certain populations with limited thumb movement, such as pediatric patients [22]. As with these patients, in myasthenic patients, the supramaximal current required for acceleromyography is expected to be higher than that for electromyography. When the electrical current increases, muscle activation may increase, causing muscle fatigue and weakening neuromuscular transmission. Furthermore, prior repetitive stimulations to stabilize acceleromyographic TOF responses might also have caused latent muscle fatigue in the present case. However, the critical data related to acceleromyography, such as the stimulating current and the sensitivity of the acceleration transducer after calibration, are unavailable in the present case. This is one of the limitations of this case report. The lack of peripheral surface temperature measurements is also another limitation of this case report. It is known that electromyographic amplitude increases as surface temperature decreases [23, 24]. Further well-designed prospective investigations are required.
In conclusion, this is the first case report comparing electromyography with acceleromyography for neuromuscular monitoring in a patient with MG, highlighting important considerations when using electromyography in such patients. This case might contribute to accumulating clinical evidence on new electromyographic devices in patients with MG, for which further data are needed.


Comments (0)