Ameloblastoma, a Potential Diagnostic Pitfall in Head–Neck Oncology: An Experience From a Tertiary Cancer Care Institute
Introduction
The significant bulk of oncopathology cases coming from head–neck surgery comprise cases of squamous cell carcinoma, particularly from an Indian perspective, due to indulgence in the habit of tobacco chewing. Odontogenic tumours, though not very uncommon, often remain outside clinical suspicion.
Case details
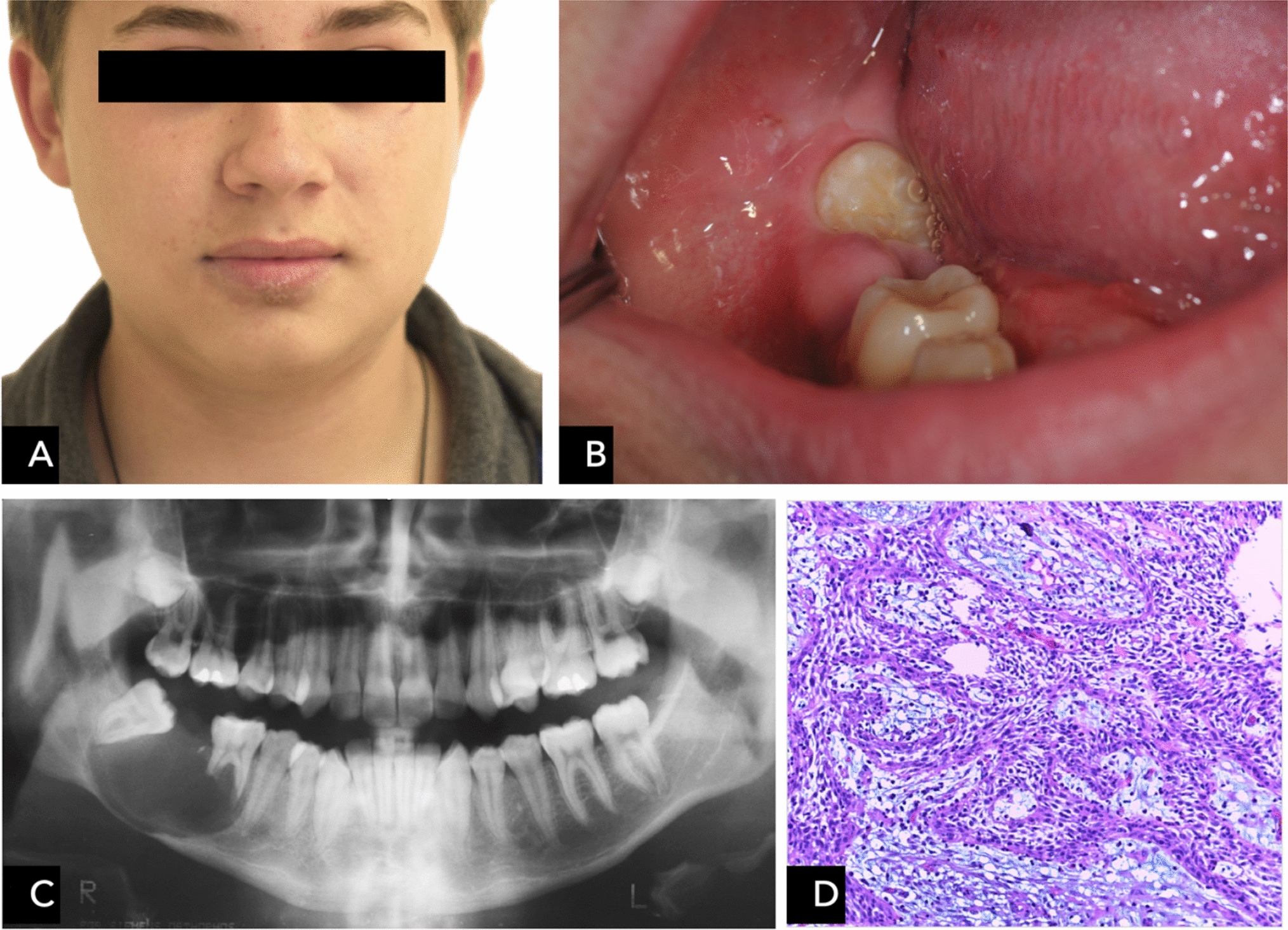
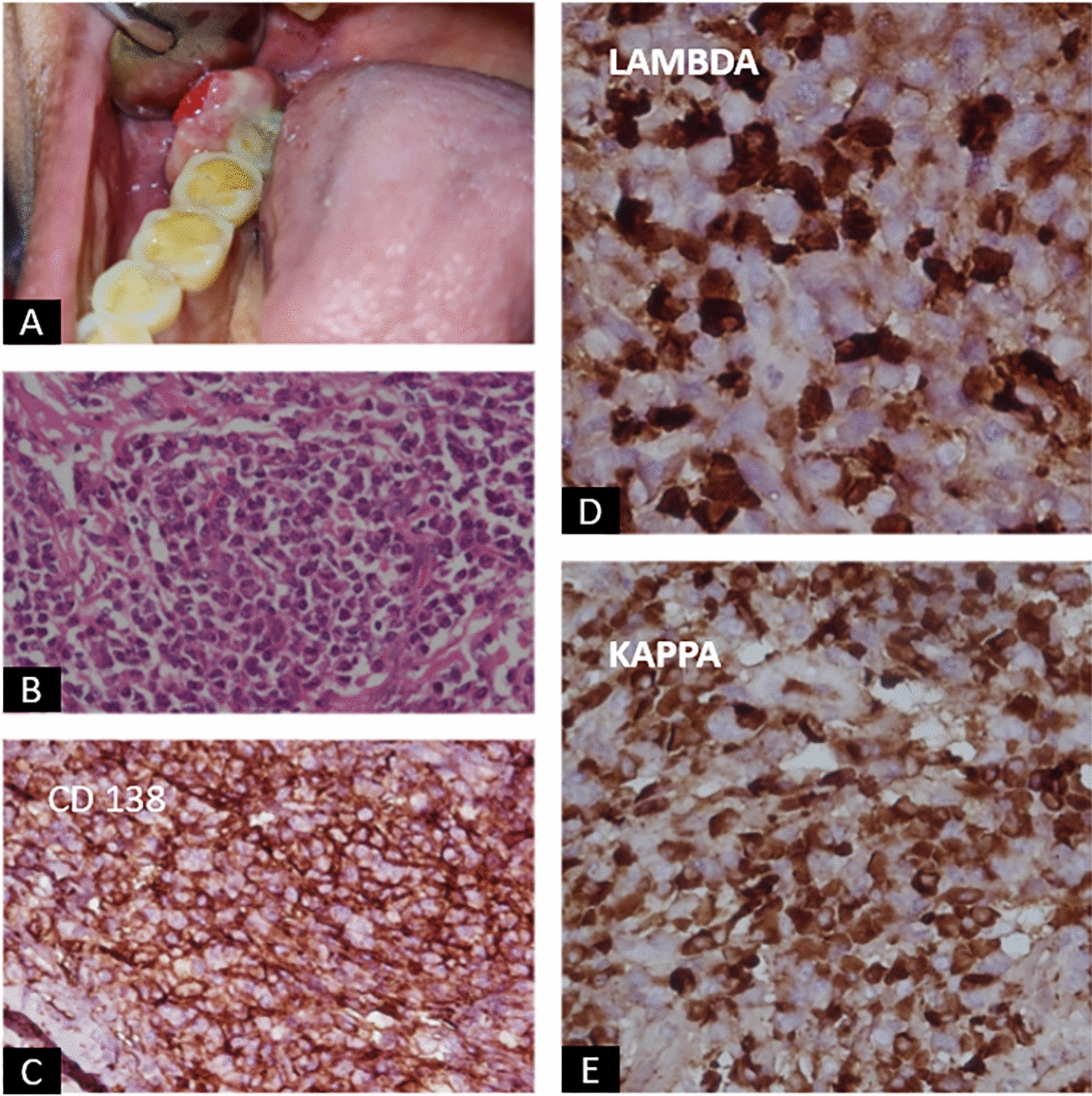
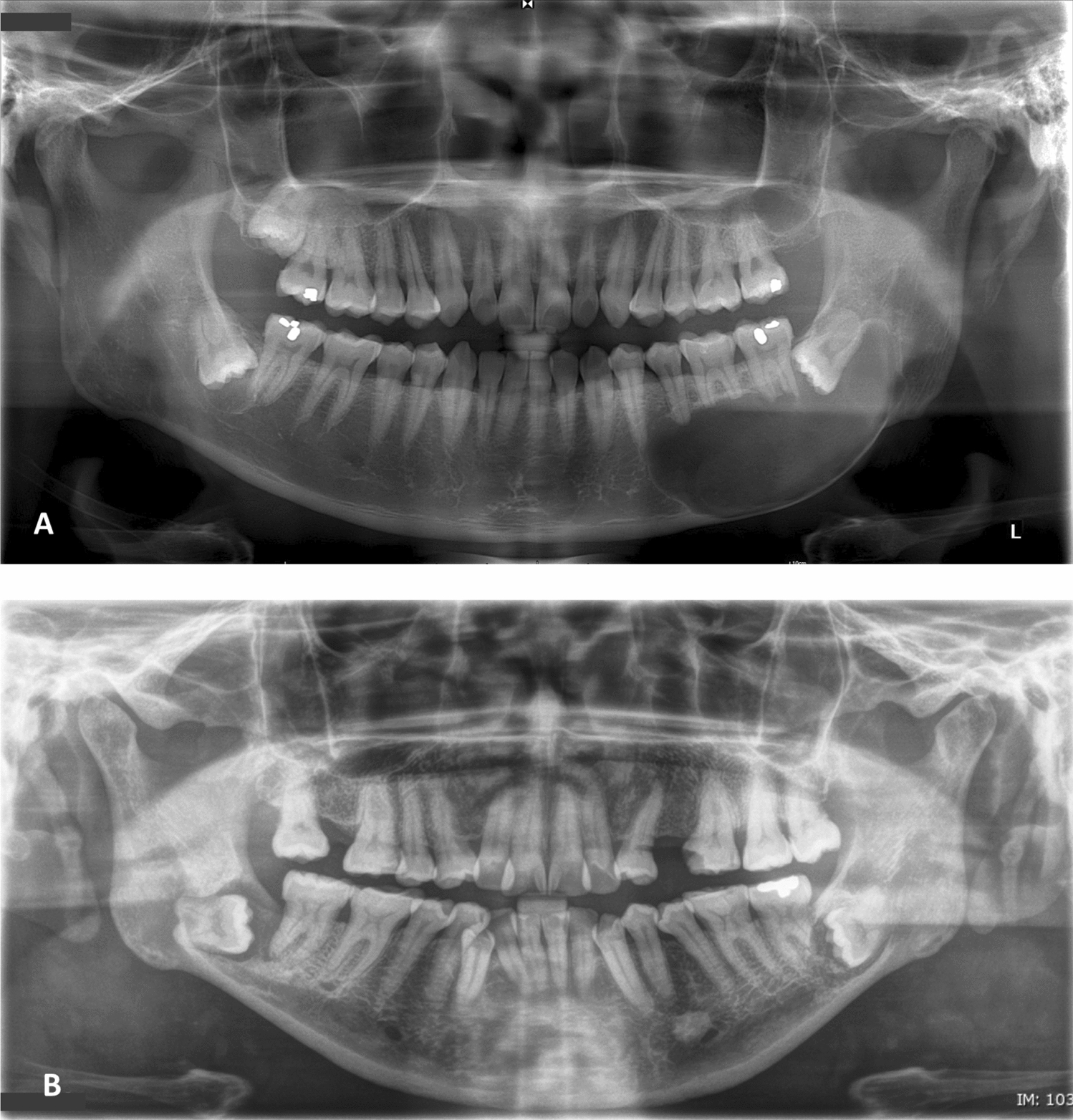
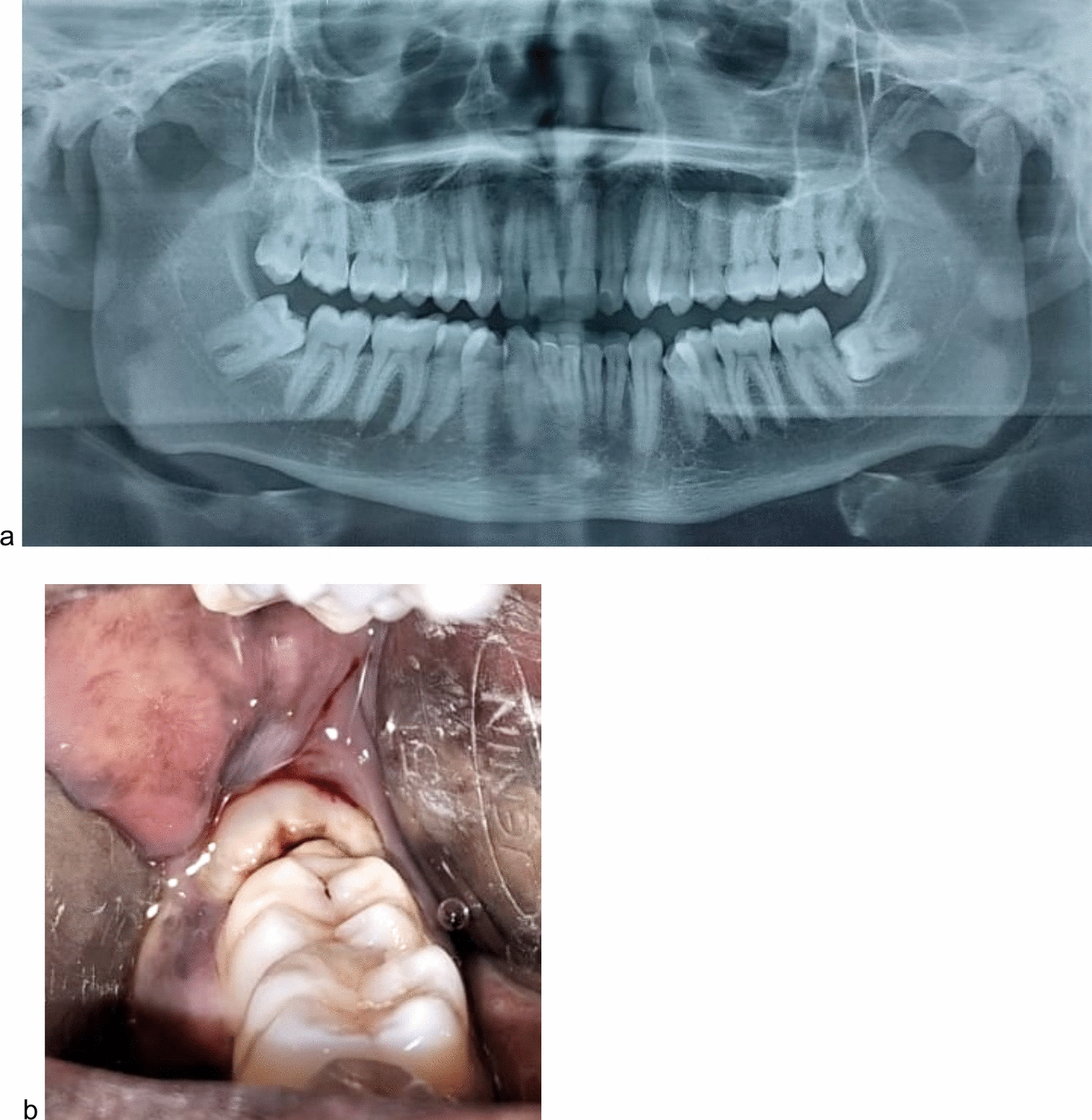
Here, we describe four cases of ameloblastoma initially misdiagnosed as other malignant entities. Two of the cases were associated with mandible, two others arose from uncommon location; one from maxilla presenting as a palatal mass and the other from sinonasal cavity.
Conclusion
With its diverse histomorphological spectrum, ameloblastoma can be quite confusing in small biopsy specimens in head–neck oncology and can be easily misdiagnosed if not included in the differentials. Virtually in every odd cases of head–neck neoplasm with bony involvement, this differential should be borne in mind to alleviate the hazard of misdiagnosing it as malignancy.



Comments (0)