
Remember me




This study is designed as a multicentre two-group parallel randomised controlled trial (RCT), to be conducted within psychiatric services in the Swedish regions of Västra Götaland, Skåne, and Halland. Several additional regions have shown interest and may be added. Participants are randomly assigned to either:
a)a brief 3–5 session preventive intervention (approx. 1 session per week), the Attempted Suicide Short Intervention Program for Older Adults (ASSIP-OA), which is an add-on to usual treatment.
b)a control group receiving treatment as usual (TAU) only.
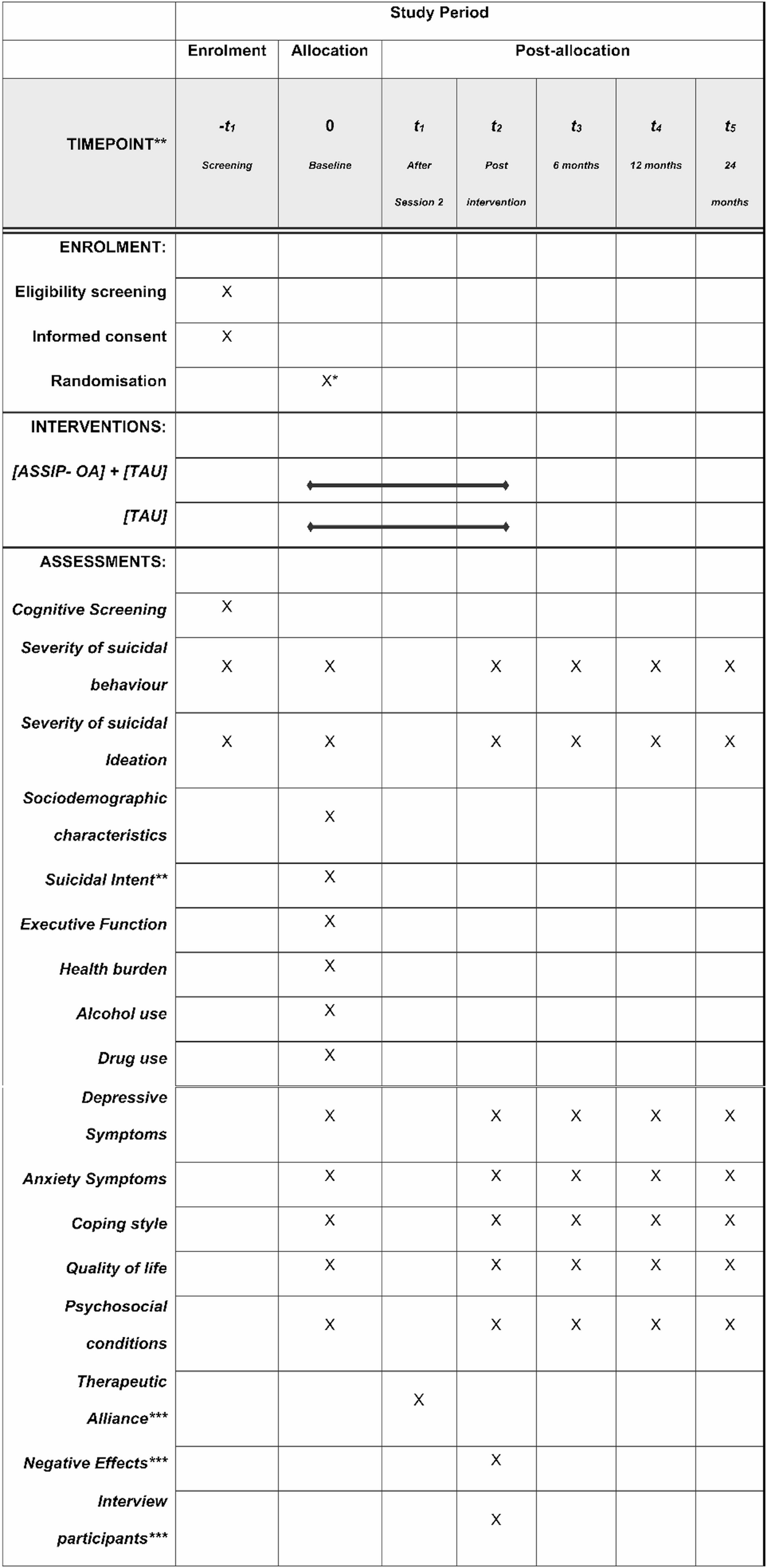
Measurements will be taken prior to randomisation and after the last session (or after 5 weeks for the control group) and follow-up measurements (see below) will be assessed at 6, 12 and 24 months after the last session. An overview of data to be collected at the various timepoints is shown in Fig. 1. Following the baseline measurement, randomisation will take place electronically via REDCap (Research Electronic Data Capture) [28] and will be conducted using block randomisation with varying block sizes and with an allocation ratio of 1:1 between intervention groups. The randomisation procedure was designed by a statistician at the University of Gothenburg, independent of the research group. Randomisation will be blinded to the data processors, as well as to the researchers and clinicians conducting the initial assessments and screening (prior to randomisation). The size of the randomisation blocks will remain undisclosed. Due to the design of the intervention, blinding participants to their assigned group will not be possible. As it is anticipated that usual treatment will vary somewhat between the study locations, it will be mapped for each patient. Data on clinical diagnoses, healthcare contacts and treatments for mental health concerns during 24 months before and after baseline measurements are derived from medical records.
The study will follow the CONSORT guidelines and was pre-registered at Clinical Trial.gov NCT06831942 on February 21, 2025 and revised May 21, 2025. The present study protocol follows the recommendations for clinical trial protocols from the SPIRIT Declaration [29, 30], see Supplementary material 1 for checklist.
Participants and recruitmentParticipants are recruited from psychiatric healthcare settings at participating centres, including inpatient psychiatric wards, outpatient psychiatric services, emergency care, and medical wards via consultation liaison services. Patients (65+) who have been hospitalised (minimum 1 night) in connection with a suicide attempt during the last 3 months or an episode of serious suicidal planning during the last month at any of the participating clinics are eligible for participation in the study. Unit managers, doctors and medical staff working in the inpatient wards, outpatient clinics and consultation psychiatric services will be informed about the study and asked to identify potential participants and provide interested patients with oral and written information about the trial.
Individuals who meet the eligibility criteria (see below) are invited to a brief screening to confirm their suitability for the study. If they remain eligible and wish to receive more information, the staff will provide detailed study information, which participants can review at their own pace. They will also have the opportunity to ask questions, which can be addressed by the study researcher as needed. The study researcher will then contact the patient to discuss the research details and answer any remaining questions. If the patient chooses to enrol, they will sign the consent form, and baseline measurements will begin. After the baseline assessment, the participant is randomised to either the intervention group (ASSIP OA + TAU) or the control group (TAU). Participants receive information about allocation in connection with the baseline visit, along with information about their scheduled appointment with an ASSIP-OA therapist or their next scheduled research assessment.
All quantitative data will be securely stored in REDCap and presented at the group level to ensure anonymity.
Eligibility criteriaInclusion criteriaAge 65 and above at time of index suicide attempt or hospitalisation for serious suicidal plans.
A mental health care contact during the active treatment period.
Capable of understanding study procedures and providing informed consent.
Exclusion criteriaClinical diagnosis of dementia or Montreal Cognitive Assessment (MoCa) score less than − 2 standard deviations from the normative score for education and age [31]. Ongoing delirium, or any other condition impeding the comprehension of the study’s procedures and implications that hinder the provision of informed consent.
Severe ongoing psychosis, severe ongoing substance use disorder, emotionally instable personality syndrome and any other condition that would require longer specialized treatment to reduce future suicidal behaviour (e.g. DBT).
Terminal illness.
Insufficient knowledge of the Swedish language (requires interpreter).
Aphasia or other severe communication issue or severe hearing and/or severe visual impairment despite corrective aids that render the intervention unfeasible.
In connection with post-treatment data collection, a purposive sample of approximately 15 participants who took part in ASSIP-OA sessions will be asked to participate in an interview to generate a deeper picture of participants’ experiences of ASSIP-OA. In addition, we will use focus group interviews to examine ASSIP-OA therapists’ experiences of the training and application of ASSIP-OA in their clinical settings, including their experiences of obstacles and opportunities in connection with the delivery of ASSIP-OA. We anticipate that all the ASSIP-OA therapists (n = approx. 14) will be interested in taking part in two sets of focus groups, but participation is voluntary.
Sample sizeA total of 132 participants will be included in the trial. The power calculation, i.e., the number of participants needed in each intervention group, is based on the previous ASSIP study of Gysin-Maillart and colleagues [17]. In that study, 26.7% of the participants in the control group, usual treatment, and 8.3% in their intervention group, ASSIP, reattempted suicide during follow-up. Based on clinical experience as well as prospective data from our previous multicentre study [12] for persons 65 + receiving usual treatment, we choose to calculate power based on an expected repetition risk of 30% in our control group (usual treatment), and 10% in our intervention group receiving ASSIP-OA plus TAU. Furthermore, given a desired power of 0.80 (a 4/5 chance of discovering an effect if it exists, regarded as adequate in this context) and a risk level of 5%, 60 participants in each condition is needed. We further expect a dropout rate of 10%, thus each group will therefore comprise 66 participants.
TherapistsThe therapists (psychiatrists, psychologists, nurses in psychiatric care, or social workers) all work as mental health professionals at the participating clinics, and all have clinical experience with suicidal patients. Presumptive ASSIP-OA therapists are required to have basic education in psychotherapy. The training to become a certified ASSIP therapist includes two days of theoretical lectures and skills training followed by supervision for approximately one year (5 patients under supervision, supervision on every session). The ASSIP-OA therapist training also includes theoretical lectures about suicidal behaviour in older adults as well as information about how the intervention has been modified to apply to older participants. The ASSIP-OA therapists are trained by a certified ASSIP supervisor (A.E.), as well as clinical gerontologists experienced in geriatric psychiatry. Only fully trained and certified ASSIP therapists or therapists in training with supervision after each session will conduct ASSIP-OA sessions with participants in this study. During the course of the project, the ASSIP-OA therapists have group meetings and continued regular supervision in groups or individually even after certification.
InterventionsTreatment groupThe treatment group will receive TAU with the addition of a modified versionof ASSIP. The full treatment protocol for ASSIP-OA is described in Table 1. The novelty of this program for older adults and the main modifications include:
Flexibility in treatment delivery, such as offering home visits, breaks and shorter/longer sessions as needed.
Optional additional session together with one or two close relatives or other support person(s), chosen by the participant.
Optional additional session to further train safety strategies (may be needed more frequently for participants with MCI or other disabilities).
Homework, letters, and case conceptualization adapted linguistically and content-wise to the target group.
ASSIP-OA also includes participants with a suicidal crisis (e.g. suicide plans/thoughts requiring hospital care).
Clinical psychologists and a psychiatrist, experienced in geriatric psychiatry in Sweden, have drawn on insights from the geriatric psychiatry clinic in Bern (personal communication, Anja Gysin-Maillart, 2025) to tailor the treatment protocol to the Swedish context. Gysin-Maillart stresses that it is not the specific components of ASSIP that require change, but rather that there should be a greater focus on the patient’s individual needs of support in areas such as loneliness, chronic pain, physical limitations and in some cases milder cognitive impairment. Gysin-Maillart highlights the need for a higher degree of flexibility when delivering ASSIP to older adults, especially for the “older older”. Providing home visits is one way to improve adherence [32]. Older adults may require extra support in communicating their needs. As most suicidal older adults are dealing with chronic medical conditions and have regular appointments with primary care, it is important to share the case conceptualisation with the patient’s GP and other relevant care providers, once permission is given by the patient. Moving to long term care was a particularly vulnerable time for older adults at the Bern clinic, an observation we have also made in our own Swedish research [33]. In such cases, ASSIP could better fit the older person’s needs by including a session with a nurse or other staff member at the care facility, chosen by the older adult, after the tree core sessions to support the translation of ASSIP warning signs and coping strategies into everyday life. Another reflection from the Bern clinical experience was that, while the video playback was not an issue for most older participants, some older men found it problematic to watch. This could be ameliorated by the therapist taking a more supportive role than they might have done with a younger patient. A more active role by the therapist may also be appropriate for older adults experiencing cognitive impairment. Enhancing problem-solving abilities is a key component of treatment protocols for individuals with suicidal tendencies and executive dysfunction [34].
Table 1 Treatment protocol for the attempted suicide short intervention program for older adults (ASSIP-OA)Control groupParticipants randomised to the control group will receive TAU in line with the regional and national guidelines. Treatment as usual (TAU) was selected as the comparator to reflect the standard care typically provided to suicidal older adults in real-world clinical settings. TAU may vary between the participating hospitals. The cornerstone of treatment as usual for suicidal older adults consists of antidepressant medication, alone or in combination with other types of psychoactive drugs (sedatives/antipsychotics/hypnotics/mood stabilisers). Persons with serious or treatment-resistant depression may be offered electroconvulsive therapy (ECT). Some persons may receive supportive/therapeutic contacts with mental health professionals (nurses/social workers/psychologists) but no psychosocial interventions designed specifically for suicidal older adults are offered as part of ordinary treatment at the participating clinics.
ScreeningPotential participants receive written information about the research project prior to screening. The screening begins with information about what it means to be part of the study. In order to determine eligibility, the short form of the Columbia Suicide Severity Rating Scale (C-SSRS) [35] is employed to investigate suicidal planning and behaviour. The Montreal Cognitive Assessment (MoCA) [36] is applied for cognitive screening. Severe ongoing psychosis, severe ongoing substance use disorder and emotionally instable personality syndrome are screened through the patients’ medical record. The screening procedure takes place at the patient’s ward/outpatient clinic.
Sociodemographic and clinical characteristicsTo characterise participants, data on demographic variables including age, sex (woman, man, non-binary or other), marital status, ethnicity, education level, and occupation prior to retirement will be gathered after study inclusion.
The Trail Making Test (TMT part A and B) [37] will be employed to assess executive function. The full (original) version of the Columbia-Suicide-Severity-Rating Scale (C-SSRS) [35] will be administered by the interviewer for history of suicidal episodes and to provide information for a global clinical risk assessment (the short form of the C-SSRS has been administered at the screening, see Fig. 1). For actual suicide attempts, suicidal intent is measured with Beck’s Suicide Intent Scale (SIS) [38]. Overall health burden will be rated with the Cumulative Illness Rating Scale for Geriatrics (CIRS-G) [39]. Alcohol use will be self-reported at this time with the Alcohol Use Disorders Identification Test (AUDIT) [40], and persons who acknowledge drug use will complete the Drug Use Disorders Identification Test (DUDIT) [41].
Outcome measuresPrimary outcomeThe primary outcome variable at 6-, 12- and 24-month follow-up is any “new suicidal episode,” a composite rating that is coded “yes” in the event of (a) a new suicide attempt as registered in the participant’s medical record or the national hospital register or (b) suicide death as registered in the national cause of death register.
Secondary outcomesThe following secondary effect measures will be collected at baseline, immediately after the intervention (for the control group 5 weeks after baseline) as well at the 6-, 12- and 24-month follow-ups.
Severity of suicidal ideationSeverity of suicidal ideation will be rated with the Columbia-Suicide Severity Rating Scale (C-SSRS) [35]. Scores range from 0 to 5, where higher scores indicate more severe ideation.
Depressive symptomsTo assess depressive symptoms the Montgomery-Åsberg Depression Rating Scale (MADRS) [42], will be applied. Each item yields a score of 0 to 6; the overall score thus ranges from 0 to 60. Higher MADRS score indicates more severe depression.
Anxiety symptomsGeneralized Anxiety Disorder 7-item scale (GAD-7) [43] will be used to assess anxiety symptoms. Each item yields a score of 0 to 3; the overall score thus ranges from 0 to 21. Higher GAD-7 score indicates more severely elevated anxiety.
Coping styleCoping styles will be assessed by Brief - Coping Orientation to Problems Experienced Inventory (Brief-COPE) [44]. The 28-item self-report scale is scored from 1 to 4 where 1 = I haven’t been doing this at all 2 = A little bit 3 = A medium amount 4 = I’ve been doing this a lot. The Brief COPE consists of 14 subscales, each representing a specific coping strategy. Each subscale consists of 2 items, making the full scale 28 items in total. Scores are presented as average scores (sum of item scores divided by number of items), indicating the degree to which the respondent has been engaging in that coping style.
Quality of lifeHealth-related quality of life is rated with the The EuroQol 5-Dimension 5-Level (EQ-5D-5 L) [45]. The EQ-5D-5 L consists of the EQ-5D descriptive system and the EQ visual analogue scale (EQ VAS). The descriptive system comprises five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression): Each dimension has 5 levels: A higher 1-digit number mean a worse outcome. Higher scores on the EQ VAS mean a better outcome.
Psychosocial conditionsIn addition, participants will fill in a brief psychosocial questionnaire with 6 single item questions inspired by scales employed in previous studies focusing on older adults’ mental health [46, 47, 48, 12]. Items are scored on a four-point Likert-scale (0–3). “Do you feel that you matter to others?” “Have you felt like a burden to others recently?” “Do you believe others would be better off without you?” “Have you had problems with loneliness recently?” “Do you feel that your situation has been hopeless recently?” “Have you had difficulties in your relationship with a partner, family member, or another important person recently?”
Therapeutic alliance, health-care utilization, negative effects of treatment and feasibility measuresTherapeutic allianceThe Working Alliance Inventory-Short Revised (WAI-SR) [49], is used to measures therapeutic alliance on 12 items on a 7-point Likert scale from 1 = “never” to 7 = “always”, after the second ASSIP-OA session.
Health-care utilisationWe will assess psychiatric inpatient hospitalizations, as well as the number and type of psychiatric healthcare contacts, based on medical records at 12- and 24-month follow-ups.
Negative effectsFurther, the Negative Effects Questionnaire (NEQ) [50], will be applied after the last ASSIP-OA session to answer the research question on side effects. NEQ contains of 32 items that are scored on a five-point Likert-scale (0–4) and differentiates between negative effects that are attributed to treatment and those possibly caused by other circumstances. At the end of the questionnaire there is also one open-ended question: “Describe in your own words if any other negative events or effects occurred, and what characterised them.”
Feasibility measuresThe following feasibility measures is used to investigate if the modified ASSIP intervention is feasible in older adults: Acceptability will be addressed in the qualitative interviews with participants post intervention. Appropriateness is measured by Cronbach alpha and mean inter-item correlation in our questionnaires (see above under effect measures). Deliverability is measured by examining that all components of the ASSIP- OA are provided on the 3–5 sessions without having to stress through them. Video recordings will be used to explore this. Fidelity: To ensure good administration of the ASSIP-OA: (1) training manuals with checklists for the therapists will be used to check after each session, and (2) video recordings of randomly selected ASSIP- OA sessions (15%) are reviewed by independent assessors using a checklist to rate the therapist’s competence and adherence to the intervention (Adherence and Competence Scale (ACS)– Gysin-Maillart et al., soon to be submitted).
Fig. 1
SPIRIT flow diagram. Schedule of enrolment, interventions, and assessments. * Participants are randomised after completion of the baseline assessment. **Suicide attempters only. *** Participants allocated to ASSIP-OA only
RetentionParticipants will always receive a scheduled appointment for an ASSIP-OA session in writing, either by mail, text message, or directly handed to them. The research team will remind participants of scheduled times to administer questionnaires by phone. Each participating centre will have a designated contact person available to address questions about the study or the recruitment process. Additionally, the research team will make regular visits to participating centres to provide support, answer questions, and reinforce awareness of the trial among healthcare staff.
Data managementAll quantitative data will be managed by Research electronic data capture (REDCap) an electronic software solution [28] that will be used for data collection and randomisation in the planned study. As REDCap is used for data monitoring, and given that this is a very brief intervention, consistent with other ASSIP trials, it does not warrant extensive oversight, and a Data Monitoring Committee (DMC) is thus not required. Qualitative data will be audio-recorded and transcribed in by a professional. All data will be kept in in fire-safe locked cabinets at the research unit to ensure participant confidentiality, and the code key will be stored separately. All data will be presented at group level so that no individual can be identified. All members of the research theme are educated and will adhere to the principes of Good Clinical Practice (GCP).
Data analysisWe will use an intention-to-treat analysis. The primary outcome will be analysed using chi-square analyses. The secondary outcomes will be analysed using a so-called “mixed effect model approach” with the aim of examining changes before and after treatment as well as during the follow-ups. This approach can take into account data clustering and covariates as well as possible dropouts.
We will examine effects both between and within groups, to be able to determine if the preventive intervention ASSIP-OA in addition to TAU has a better effect than the control group, treatment as usual (TAU), after the intervention (between-group effect). Further, we want to find out whether ASSIP-OA and the control group have improved over time (within-group effect) and, if the ASSIP-OA has any effect, whether such effect is “driven” by the ASSIP-OA (interaction effect). The statistical approach is based on regression analyses. Contrary to more traditional variable-oriented analyses for repeated measurements, it has the benefit of taking into consideration the fact that data are not independent at repeated measurements over time and provides better handling of missing data by incorporating all available information. This method is now regarded as preferable to using more traditional methods for missing data in clinical studies.
For qualitative data collected through individual and focus group interviews, transcribed interviews will be analysed, and themes and subthemes will be identified and categorised following Braun and Clarke’s thematic analysis [51].
EthicsEthical approval for the planned trial was granted by the Swedish Ethical Review Authority (2024-07392-01). The study therapists will continuously evaluate the participants’ suicidal ideation/planning at each treatment session. Any indication of increased suicidal ideation at any point during the project will prompt immediate contact with the participant’s care professionals. The participant’s physician will be informed without delay if a clinically relevant rise in suicidal ideation or other signs of acute distress are noted during the study. Adverse events will be registered at each session. Participation will be entirely voluntary, with no financial or other incentives, and all participants must provide written informed consent. In line with our ethical approval, patient insurance coverage is ensured and available to participants should the need arise.
Comments (0)